
Easy explanation according to Ms 1 level
Musculoskeletal Module CBL 1 - Easy Explanation (MS1 Level)
The Clinical Story (What is happening to this patient?)
- A crack on her nipple - this is a gateway for bacteria to enter
- A hot, red, tender lump in her right breast - this is an abscess (collection of pus)
- A 4x4 cm lump in her right armpit (axilla) - this is a swollen lymph node
- Swelling of her right arm - the lymph node is blocking lymph drainage from the arm
- Fever - her body is fighting an infection
Learning Objective 1: Anatomy of the Breast
- The flesh = glandular tissue (lobes and lobules that make milk)
- The juice channels = lactiferous ducts that carry milk to the nipple
- The skin = overlying skin with nipple and areola
- The breast sits on top of the pectoralis major muscle
Key zones of the breast:
| Quadrant | % of Breast Tissue | Clinical Note |
|---|---|---|
| Upper Outer | ~50% | Most cancers occur here |
| Upper Inner | ~15% | |
| Lower Outer | ~11% | Our patient's lump is here |
| Lower Inner | ~6% | |
| Central (areola) | ~18% |
Learning Objective 2: Boundaries of the Axilla
| Wall | Made of |
|---|---|
| Anterior wall | Pectoralis major + minor muscles |
| Posterior wall | Subscapularis, teres major, latissimus dorsi |
| Medial wall | Serratus anterior on the ribs |
| Lateral wall | Intertubercular groove of humerus (narrowest part) |
| Apex | Opens into the neck (between clavicle, 1st rib, scapula) |
| Base | Axillary fascia (the skin of your armpit) |
- Axillary artery and vein
- Brachial plexus (nerves to the arm)
- Axillary lymph nodes (30-60 nodes) - most important for this case!
- Fat and connective tissue
Learning Objective 3: Why the Axilla Matters in Breast Disease
Q1 - Lymphatic Drainage of the Breast
- 75% → Axillary lymph nodes (main route - why the armpit swells!)
- Rest → Internal mammary nodes (along the sternum), supraclavicular nodes, opposite breast
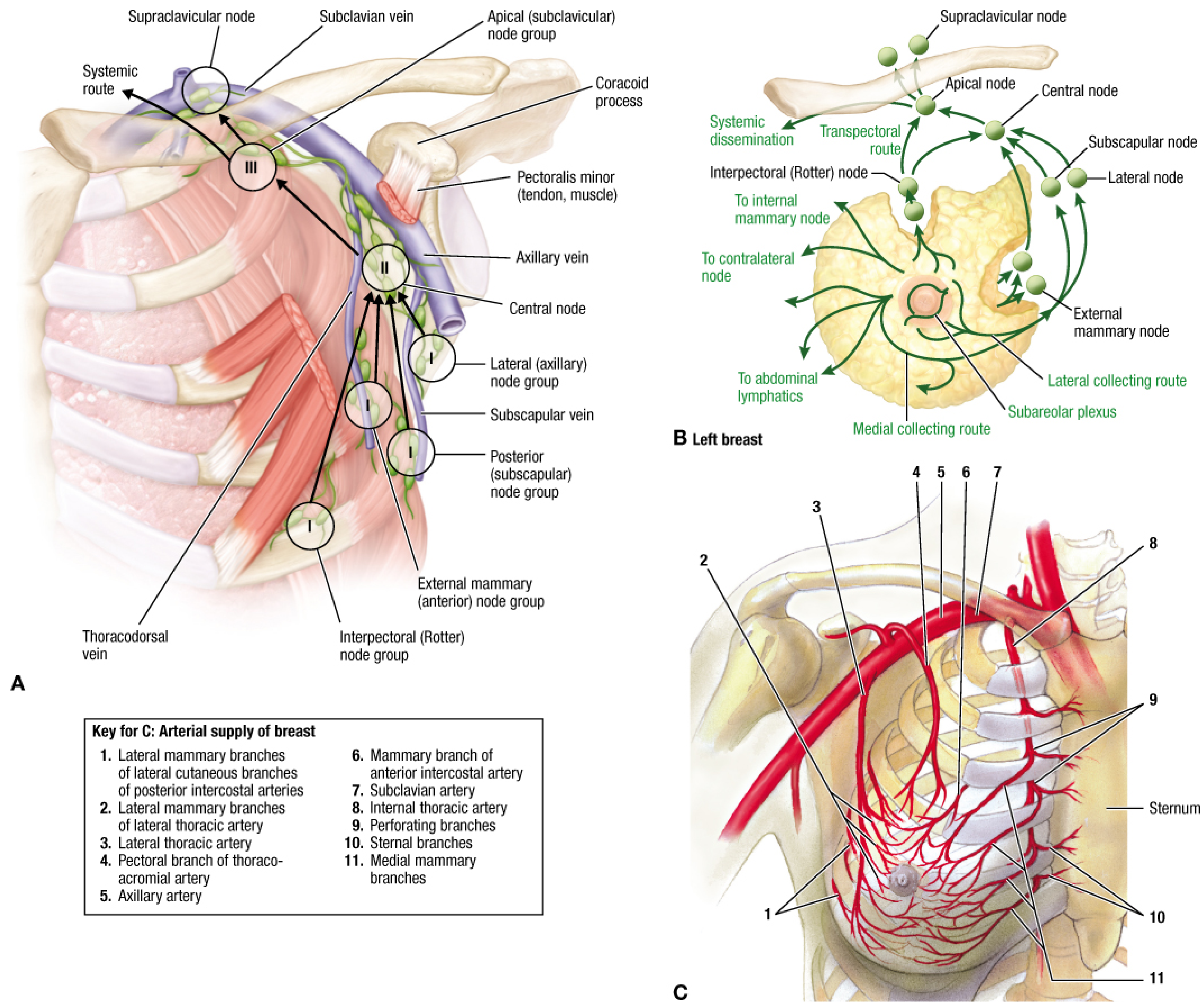
| Level | Location | Nodes Included |
|---|---|---|
| Level I (Ground floor) | Lateral to pectoralis minor | Pectoral, subscapular, lateral, paramammary nodes |
| Level II (1st floor) | Behind pectoralis minor | Interpectoral (Rotter's), central nodes |
| Level III (2nd floor) | Medial to pectoralis minor | Apical nodes |
Q2 - Differential Diagnosis of a Breast Lump (in a Lactating Woman)
- Breast Abscess ← most likely in this patient (hot, red, tender, febrile, cracked nipple)
- Mastitis (early stage before abscess forms - no fluctuant mass yet)
- Lactating Adenoma (benign tumor of glandular tissue that grows during lactation)
- Fibroadenoma (most common benign lump in young women - smooth, mobile, rubbery)
- Galactocele / Milk retention cyst (milk blocked in a duct, forms a cyst)
- Fibrocystic Disease (multiple tender lumps, vary with cycle)
- Phyllodes Tumor (rare benign or low-grade tumor)
- Breast Cancer (must NEVER miss this - inflammatory carcinoma can mimic an abscess)
Note from Creasy & Resnik's Maternal-Fetal Medicine: "80% of breast biopsies in pregnant women are benign, but any lump present for 2-4 weeks should be biopsied."
Q3 - Investigations to Suggest
| Investigation | Why? |
|---|---|
| Breast Ultrasound | #1 choice - confirms abscess cavity (dark fluid collection), guides aspiration; safe, cheap, no radiation |
| FNA / Pus Culture & Sensitivity | Find out which bacteria it is (usually S. aureus) so you can pick the right antibiotic |
| CBC (Full Blood Count) | High WBC confirms infection/inflammation |
| Blood Culture | If she looks very sick (sepsis) |
| Mammography | Less useful here (young, dense breast + lactating = high false-negative rate), but can be done if cancer suspected |
| MRI | Not first-line, but can show extent; avoid gadolinium if still lactating |
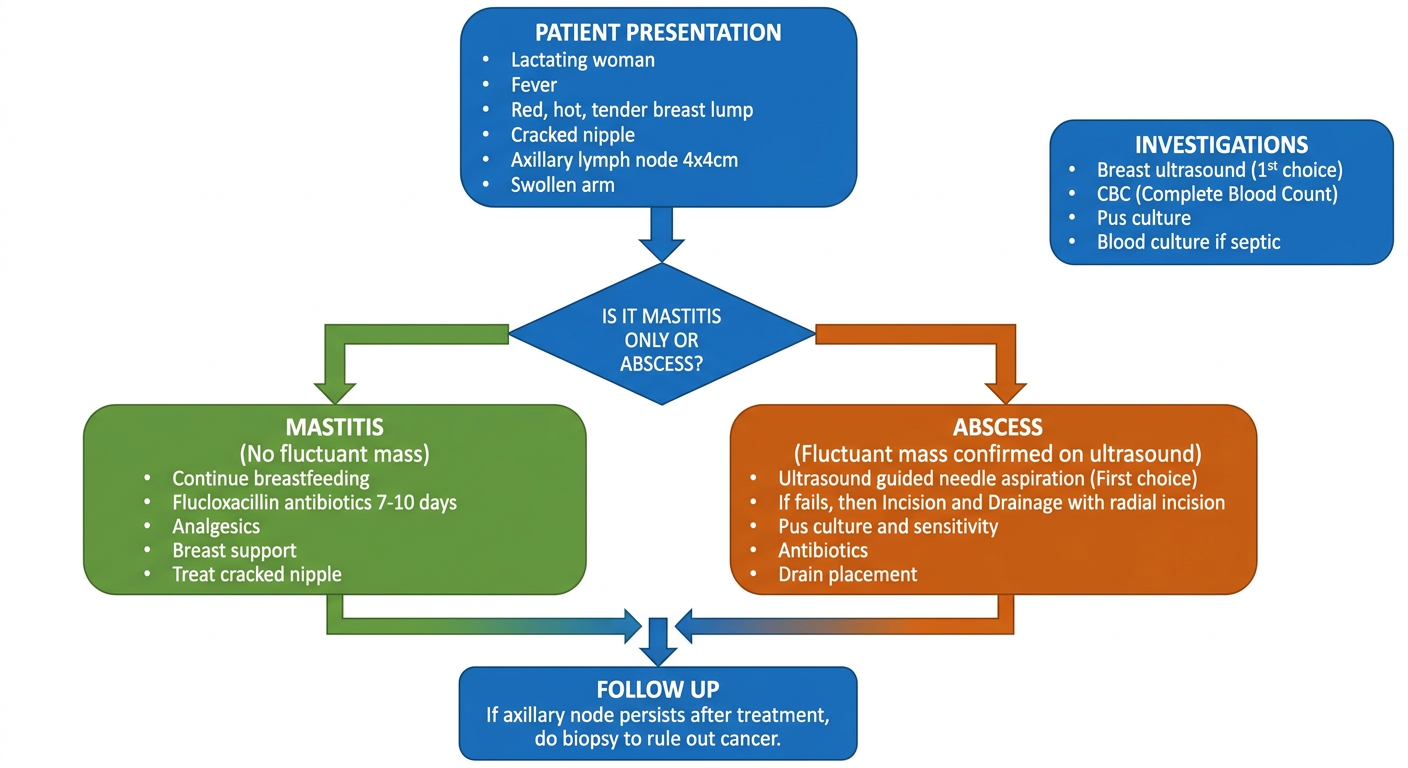
Q4 - Management
Step 1: Treat the Infection
- Do NOT stop breastfeeding (continuing feeding actually helps drain the breast)
- Antibiotics: Dicloxacillin or Flucloxacillin (covers S. aureus, including penicillin-resistant strains) for 7-10 days
- Analgesics (paracetamol/NSAIDs) for pain and fever
- Breast support
- Ultrasound-guided needle aspiration - preferred first-line (less scarring, preserves breastfeeding)
- If aspiration fails → Incision & Drainage under general anaesthetic
- Radial incision near nipple (to protect the milk ducts)
- Break down loculi (pockets of pus) with a finger
- Send pus for culture
- Place drain if needed
- Continue antibiotics
Step 2: Protect the Nipple (entry point)
- Treat the cracked nipple - proper latch-on technique teaching, nipple cream
- This prevents re-infection
Step 3: Address the Axillary Node
- If the axillary node is reactive (due to infection), it will shrink once the breast infection is treated
- If it persists after treatment → biopsy to rule out lymphoma or breast cancer spread
Step 4: Patient Education
- Breastfeeding technique
- Breast hygiene
- Early presentation if symptoms recur
Quick Memory Summary
Cracked nipple → bacteria enter → Mastitis → Abscess
↓
Lymph drainage → Axillary nodes get infected/enlarged
↓
Enlarged node blocks arm lymph → Arm swells
Treatment: Antibiotics + Ultrasound-guided drainage + Fix the nipple
- General Anatomy and Musculoskeletal System (THIEME Atlas), p. 230
- Fischer's Mastery of Surgery, 8th ed., p. 1396
- Creasy & Resnik's Maternal-Fetal Medicine, p. 987
- Pye's Surgical Handicraft, 22nd ed., p. 3668
- Berek & Novak's Gynecology, p. 987
Explain with a pictorial representation or a vidoe
Medical education diagram for MS1 students showing breast anatomy and axillary lymph node levels. Left side: labeled cross-section of female breast showing lobes, lobules, lactiferous ducts, nipple, areola, subareolar plexus, pectoralis major muscle, axillary tail of Spence, and breast quadrants (upper outer 50%, upper inner 15%, lower outer 11%, lower inner 6%, central 18%). Right side: anterior view showing the axilla as a pyramid shape with labeled walls (anterior wall = pectoralis major/minor, posterior wall = subscapularis/latissimus dorsi, medial wall = serratus anterior, lateral wall = humerus), and axillary lymph node levels I, II, III relative to pectoralis minor muscle. Color coded, clean white background, educational style with clear labels and arrows.
Medical education flowchart diagram showing lactational breast abscess pathophysiology for medical students. Step by step visual: Step 1 shows cracked nipple with bacteria (Staphylococcus aureus) entering. Step 2 shows mastitis - red inflamed breast tissue with white blood cells. Step 3 shows abscess formation - collection of pus inside breast, hot red swollen lower quadrant. Step 4 shows lymphatic spread - bacteria traveling through lymphatic vessels to axillary lymph nodes causing node enlargement (4x4cm). Step 5 shows blocked lymph drainage from arm causing arm swelling (lymphedema). Arrows connect each step. Differential diagnosis box on side listing: abscess, mastitis, fibroadenoma, galactocele, fibrocystic disease, breast cancer. Clean medical illustration style, color coded, white background.
Medical education diagram showing lymphatic drainage of the breast for MS1 students. Central image of a left breast (front view) with labeled arrows showing: subareolar plexus under nipple collecting lymph from all quadrants. Main route (75%) with thick green arrow going to axilla showing Level I nodes (pectoral/external mammary, subscapular, lateral nodes - lateral to pectoralis minor), Level II nodes (central, interpectoral/Rotter nodes - behind pectoralis minor), Level III nodes (apical/subclavicular nodes - medial to pectoralis minor). Secondary routes shown with thinner arrows: to internal mammary/parasternal nodes along sternum (medial drainage), to supraclavicular nodes, to contralateral breast, to abdominal lymphatics. Clinical significance box: Level I involvement = 65% 5yr survival, Level II = 31%, Level III = near 0%. Color coded levels (green=I, yellow=II, red=III). Clean white background, educational medical illustration.
Medical education management algorithm diagram for lactational breast abscess for MS1 students. Decision tree format. Top: Patient presentation box - lactating woman, fever, red hot tender breast lump, cracked nipple, axillary lymph node 4x4cm, swollen arm. Arrow down to: Is it mastitis only or abscess? Left branch MASTITIS (no fluctuant mass): green box - continue breastfeeding, flucloxacillin antibiotics 7-10 days, analgesics, breast support, treat cracked nipple. Right branch ABSCESS (fluctuant mass confirmed on ultrasound): orange box - ultrasound guided needle aspiration (first choice), if fails then incision and drainage with radial incision, pus culture and sensitivity, antibiotics, drain placement. Bottom box: Follow up - if axillary node persists after treatment do biopsy to rule out cancer. Investigations box on side: Breast ultrasound (1st choice), CBC, pus culture, blood culture if septic. Clean white background, color coded flowchart, medical illustration style.
Diagram 1 - Breast Anatomy + Axilla Boundaries
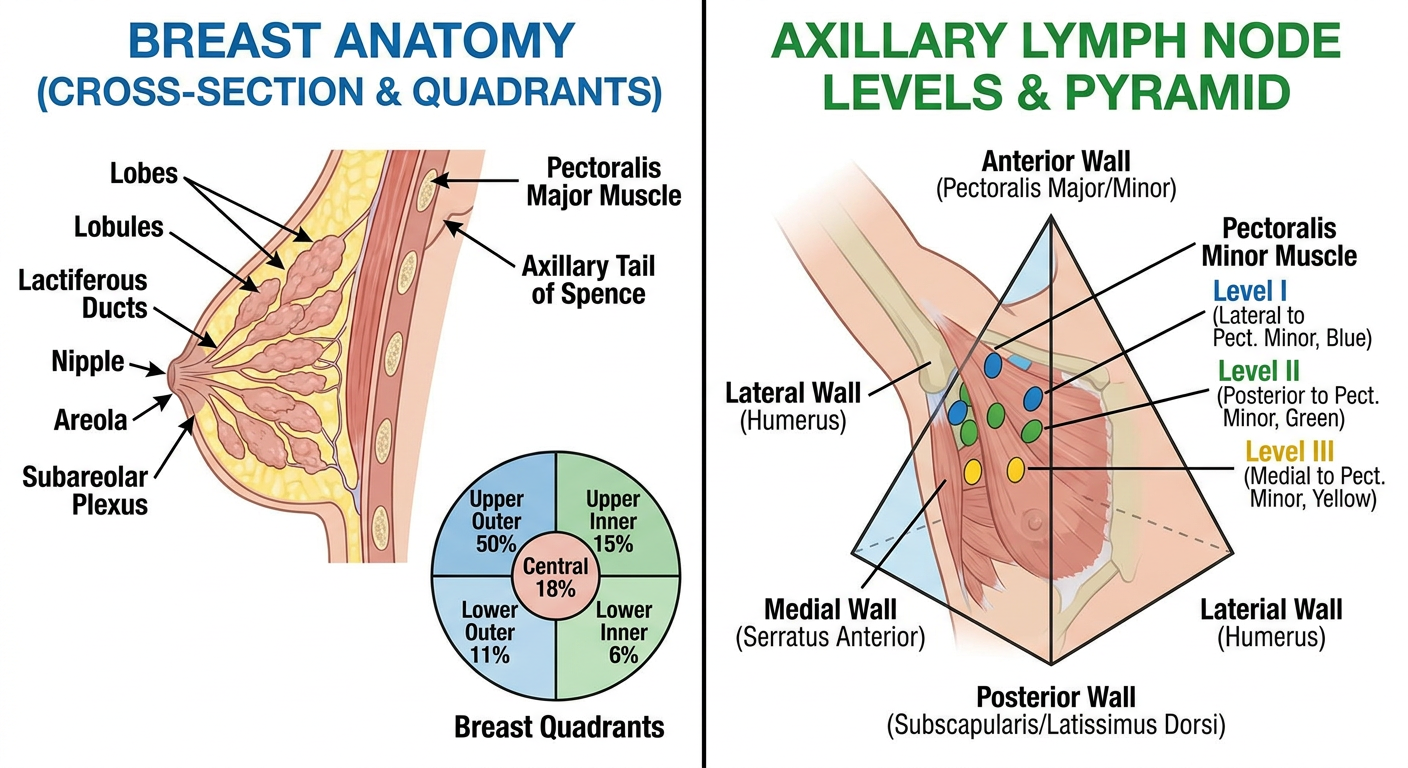
- The breast sits on pectoralis major
- The axillary tail is where breast tissue sneaks into the armpit - that's why breast problems affect the axilla
- The axilla is a pyramid - 4 walls, an apex (opens to neck), and a base (armpit skin)
Diagram 2 - What Happened to This Patient (Pathophysiology)
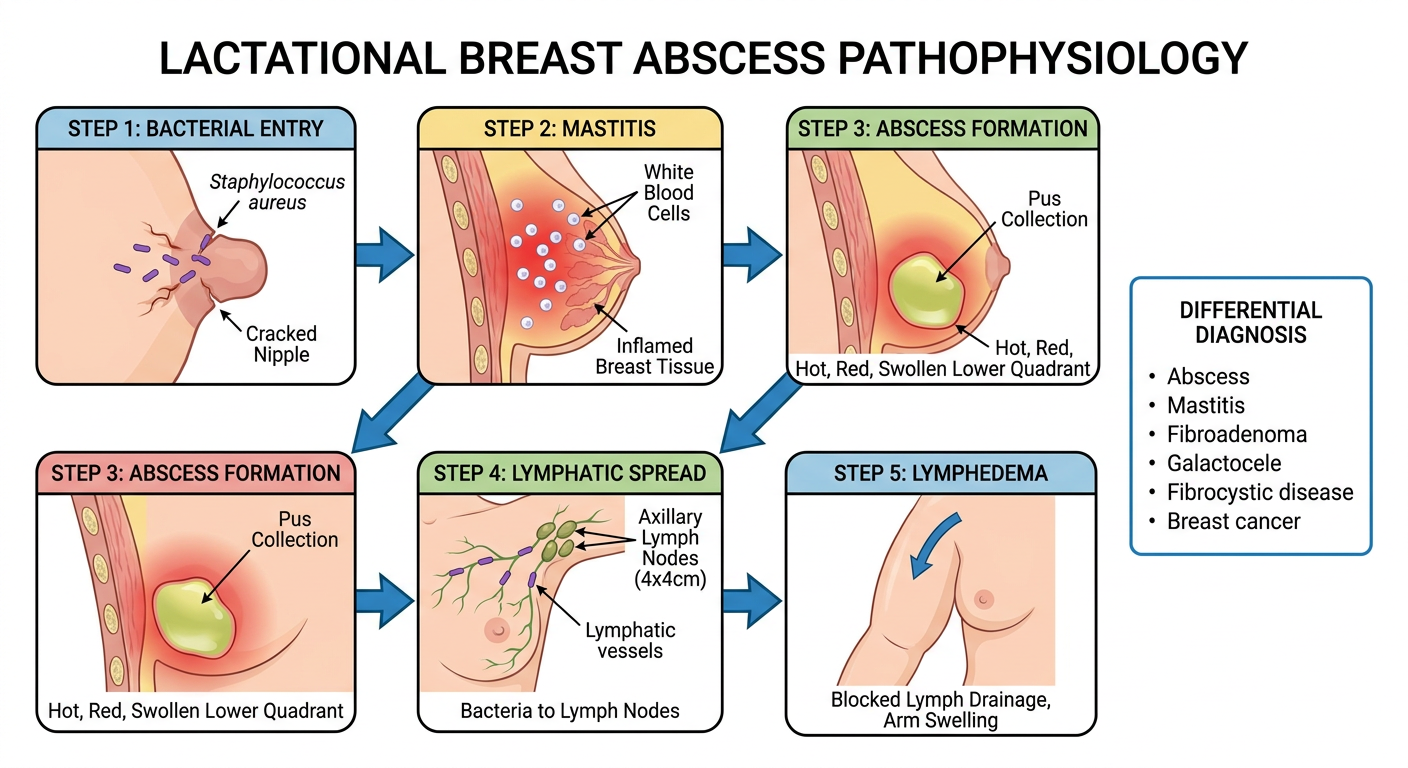
Diagram 3 - Lymphatic Drainage (Q1 Answer)
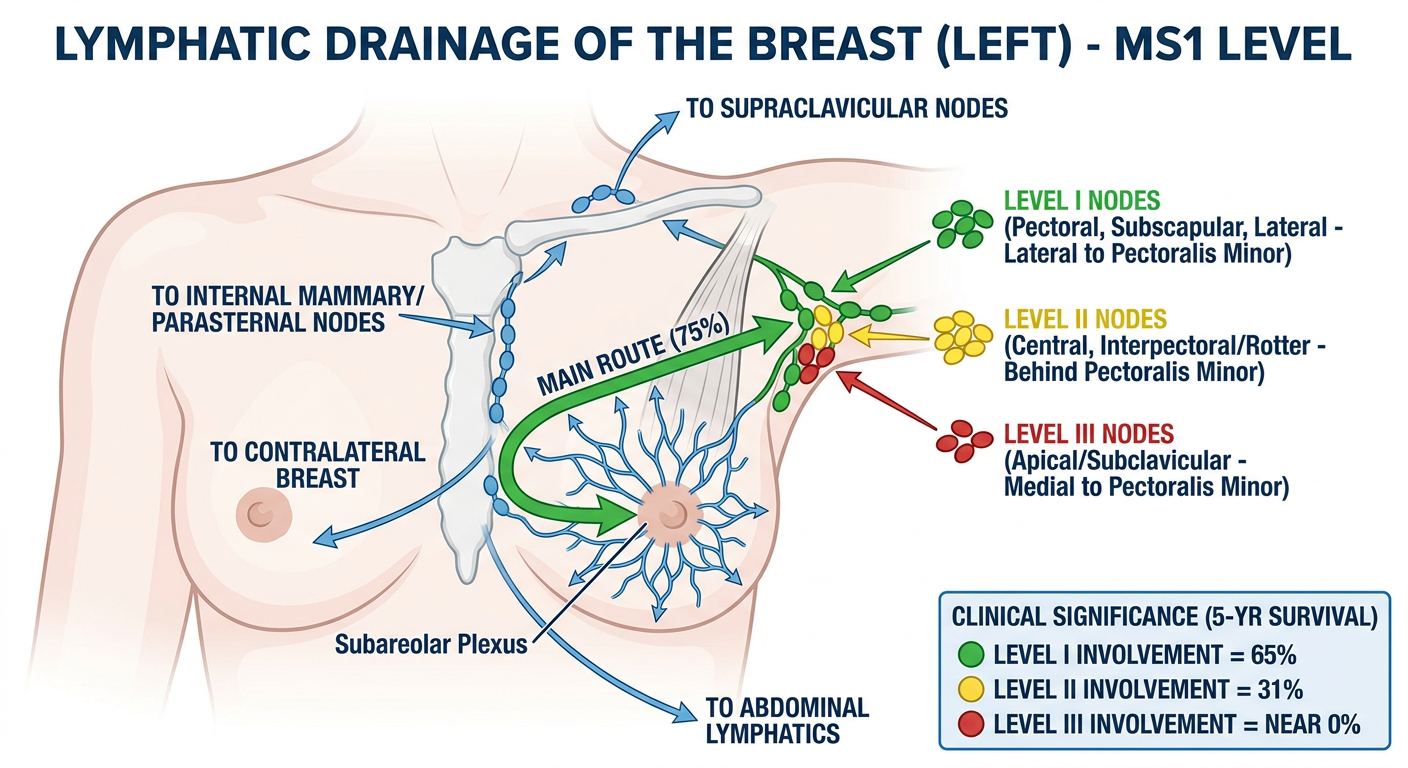
- Level I nodes affected → 65% 5-year survival
- Level II nodes affected → 31%
- Level III nodes affected → nearly 0%
Diagram 4 - Management Flowchart (Q3 + Q4 Answer)
Regarding a Video
- Breast anatomy: Search "Breast anatomy Armando Hasudungan" on YouTube - best illustrated walkthrough for MS1
- Lymphatic drainage: Search "Lymphatic drainage of breast Ninja Nerd" - very clear level-by-level explanation
- Breast abscess: Search "Lactational mastitis and abscess Osmosis" on YouTube - animated pathophysiology with clinical correlation
- Axilla boundaries: Search "Axilla anatomy Zero to Finals" - concise MS1 level explanation