Describe different method of cervical screening in detail. Mention about sensitivity, specificity of all method,. Which method is preferred for primary screening and why. Also describe methods of screening in low resource setting. Explain using latest guidelines, and use tables wherever required.
Reading File
Finding Sources
Finding Sources
Searching PubMed
cervical cancer screening HPV primary screening guidelines
Searching the Web
cervical screening methods sensitivity specificity HPV test Pap smear VIA 2024 2025 guidelines WHO
Reading File
Reading File
Reading File
Reading Web Page
cervical screening sensitivity specificity HPV Pap smear VIA low resource settings guidelines
Reading File
Loading Image
Searching PubMed
VIA visual inspection acetic acid cervical cancer screening sensitivity specificity low resource
I now have comprehensive information to write a detailed response. Let me compose the full answer:
Cervical Cancer Screening: Methods, Performance, and Guidelines
Cervical cancer is one of the most preventable cancers because it progresses through well-characterized precursor lesions (CIN 1-3) over years to decades before becoming invasive. Effective screening can detect and treat these precursors, reducing incidence by up to 79% and mortality by 70%.
1. Overview of Screening Methods
| Screening Method | Principle | Setting | Laboratory Required |
|---|---|---|---|
| Conventional Pap smear | Cytology of exfoliated cells | Resource-rich | Yes |
| Liquid-based cytology (LBC) | Improved cytology technique | Resource-rich | Yes |
| HPV DNA testing | Molecular detection of HR-HPV | Any | Yes (molecular lab) |
| Co-testing (HPV + cytology) | Combined approach | Resource-rich | Yes |
| Visual Inspection with Acetic Acid (VIA) | Naked-eye inspection | Low-resource | No |
| Visual Inspection with Lugol's Iodine (VILI) | Iodine-based visual test | Low-resource | No |
| Colposcopy | Magnified visual examination | Diagnostic (not primary) | No |
| HPV Self-sampling | Patient-collected sample for HPV testing | Expanding | Yes |
2. Conventional Pap Smear (Cervical Cytology)
Technique
A spatula or endocervical brush is used to scrape cells from the transformation zone circumferentially. Cells are smeared onto a glass slide, fixed, and stained using the Papanicolaou method. Conventional or automated image analysis systems screen the slide for cellular abnormalities.
Reporting (Bethesda System 2014)
- NILM (Negative for Intraepithelial Lesion or Malignancy)
- ASC-US (Atypical Squamous Cells - Undetermined Significance)
- ASC-H (cannot exclude HSIL)
- LSIL (Low-grade Squamous Intraepithelial Lesion)
- HSIL (High-grade Squamous Intraepithelial Lesion)
- AGC (Atypical Glandular Cells)
- Carcinoma
Performance
| Parameter | Conventional Pap |
|---|---|
| Sensitivity (CIN2+) | 47-62% (single test) |
| Specificity | 60-95% |
| False-negative rate | ~49% |
| Unsatisfactory sample rate | 2-5% |
- Berek & Novak's Gynecology, p. 845: The Agency for Healthcare Research and Quality concluded the sensitivity of conventional cytology in detecting cervical cancer precursors was 51%, with an estimated false-negative rate of 49%.
Limitations
Errors arise from three sources:
- Sampling errors - lesion too small to exfoliate, device did not pick up cells
- Fixation/preparation errors - air drying, blood/mucus obscuring the slide
- Interpretive errors - missed by the cytotechnologist
3. Liquid-Based Cytology (LBC)
Technique
The cervical sample is collected with a plastic broom or endocervical brush + spatula and rinsed thoroughly into a vial containing liquid alcohol-based preservative. In the laboratory, the liquid is filtered to trap larger epithelial cells, yielding a thin, uniform monolayer free of debris.
FDA-approved systems: ThinPrep (Hologic) and SurePath (BD Diagnostics).
Advantages Over Conventional Cytology
- 80-90% of cells transferred to liquid media vs. only 10-20% with conventional smear
- Eliminates air-drying artifact
- Reduces unsatisfactory samples by 70-90%
- Residual fluid can be used for HPV testing, STI testing, and repeat smears (one sample, multiple tests)
Performance
| Parameter | LBC | Conventional |
|---|---|---|
| Sensitivity (CIN2+) | ~60-70% | 47-62% |
| Specificity | ~85-95% | 60-95% |
| Unsatisfactory rate | <1% | 2-5% |
| Cell transfer | 80-90% | 10-20% |
Automated Systems
The FDA has approved automated image-guided slide screening systems (e.g., ThinPrep Imaging System) that couple an automated microscope with a digital camera. Computer algorithms rank slides by probability of abnormality. This reduced the false-negative rate by 32%.
Limitation
More expensive than conventional cytology; this compromises utility in lower-resource settings.
4. HPV DNA Testing
Principle
Detects the DNA (or RNA) of high-risk HPV genotypes (predominantly HPV 16, 18, 31, 33, 45, 52, 58) in cervical specimens. HPV 16 and 18 account for approximately 70% of all cervical cancers.
FDA-Approved Assays (as of 2025)
| Assay | Target | Technique | Typing | ASC-US Triage | Co-test | Primary Screen |
|---|---|---|---|---|---|---|
| Hybrid Capture 2 (Qiagen) | DNA genomic | DNA:RNA hybridization | No | Yes | Yes | No |
| Cervista (Hologic) | L1 DNA | Invader technology | 16/18 reflex | Yes | Yes | No |
| Cobas HPV (Roche) | L1 DNA | PCR TaqMan | 16/18 | Yes | Yes | Yes |
| BD Onclarity (BD) | E6/E7 DNA | PCR | 16/18/others | Yes | Yes | Yes |
| Alinity m HR HPV (Abbott) | DNA | PCR | 16/18 | Yes | Yes | Yes |
From: Berek & Novak's Gynecology, Table 16-2; Harrison's Internal Medicine 22e
Performance
| Parameter | HPV DNA Testing |
|---|---|
| Sensitivity (CIN2+) | 88-97% (higher than cytology) |
| Specificity (CIN2+) | 84-92% |
| Negative predictive value | >99% (single most important feature) |
| Sensitivity for CIN3+ | ~95% |
A 2024-2025 study from a tertiary center in India found HPV DNA testing showed sensitivity of 92.4% and specificity of 89.1% for CIN2+ detection, superior to both Pap smear and VIA.
Why High Sensitivity Matters
The very high negative predictive value of HPV testing means a woman who tests HPV-negative has an extremely low risk of developing significant cervical disease in the next 5+ years. This is the biological basis for extended screening intervals.
Clinical Use of Genotyping
- HPV 16 or 18 positive: Direct referral to colposcopy (high enough positive predictive value in the general population)
- Other high-risk HPV types positive: Reflex cytology obtained first before colposcopy decision
- HPV negative: Reassurance for 5 years
Limitation in Women <30 Years
HPV testing is NOT recommended as a primary screen in women under 30 because transient HPV infections are very common in this age group, leading to low specificity and unnecessary colposcopy referrals. - Robbins, Cotran & Kumar, p. 926
5. Co-Testing (HPV + Cytology)
This approach simultaneously performs both HPV testing and cytology on the same liquid-based sample, providing the highest sensitivity of any current screening combination.
Performance
| Parameter | Co-testing |
|---|---|
| Sensitivity (CIN3+) | ~99% |
| Specificity | Slightly lower than cytology alone |
| NPV | Very high (~99.9%) |
Guidelines for Co-testing
- USPSTF (endorsed by ACOG, ASCCP, SGO): Acceptable option for women aged 30-65, every 5 years
- ACS 2025 update: Acceptable if primary HPV testing is unavailable
Advantage
Allows extended 5-year screening intervals when both tests are negative, reducing the screening burden on the healthcare system.
6. Visual Inspection with Acetic Acid (VIA)
Principle
A 3-5% acetic acid solution is applied to the cervix. After 1-2 minutes, the cervix is inspected with the naked eye (or a simple halogen lamp). Abnormal squamous epithelium (dysplasia/CIN) appears as dense acetowhite lesions at or near the transformation zone.
Technique
- Patient positioned in lithotomy position
- Cervix visualized with speculum
- 3-5% acetic acid applied for 1 minute
- Cervix inspected with adequate light
- Result interpreted immediately ("screen and treat" approach possible)
Performance
| Parameter | VIA |
|---|---|
| Sensitivity (CIN2+) | 49-79% (highly variable; comparable to or slightly lower than Pap) |
| Specificity | 49-86% (lower; leads to higher referral/overtreatment rates) |
| Positive predictive value | ~10-20% |
| NPV | ~97% when negative |
A recent multicenter Indian study (2024-2025) reported VIA sensitivity of 62.7% and specificity of 81.4% for CIN2+, noting it as the lowest-performing of the three modalities studied.
Key Advantage: Screen-and-Treat
Because results are immediate, patients can undergo cryotherapy or LEEP at the same visit without needing to return for a second appointment. This is highly valuable where patient follow-up is unreliable.
Limitation
- Highly operator-dependent
- Low specificity leads to overtreatment
- Cannot detect endocervical lesions
- Postmenopausal patients: transformation zone may be inside the canal, reducing accuracy
- No permanent record
7. Visual Inspection with Lugol's Iodine (VILI)
Principle
Lugol's iodine (strong iodine solution) applied to the cervix. Normal glycogen-containing squamous epithelium stains mahogany brown/black (iodine-positive). Abnormal areas lacking glycogen remain mustard yellow (iodine-negative = positive VILI test).
Performance
| Parameter | VILI |
|---|---|
| Sensitivity (CIN2+) | 72-91% |
| Specificity | 64-85% |
VILI may have slightly higher sensitivity than VIA in some studies. Less data are available for VILI than VIA.
Comparison: VIA vs. VILI
| Feature | VIA | VILI |
|---|---|---|
| Stain used | 3-5% acetic acid | Lugol's iodine |
| Positive result | Acetowhite areas | Yellow/mustard areas |
| Training needed | Moderate | Moderate |
| Cost | Very low | Very low |
| Specificity | Lower | Slightly higher |
| Evidence base | Extensive | More limited |
8. Comparative Performance Summary
| Method | Sensitivity (CIN2+) | Specificity (CIN2+) | NPV | Cost | Lab Required | Interval |
|---|---|---|---|---|---|---|
| Conventional Pap smear | 47-62% | 60-95% | High | Low | Yes | 3 years |
| Liquid-based cytology | 60-70% | 85-95% | High | Moderate | Yes | 3 years |
| HPV DNA testing (primary) | 88-97% | 84-92% | >99% | Moderate | Yes | 5 years |
| Co-testing (HPV + cytology) | ~99% | Moderate | ~99.9% | Higher | Yes | 5 years |
| VIA | 49-79% | 49-86% | ~97% | Very low | No | 2-3 years |
| VILI | 72-91% | 64-85% | High | Very low | No | 2-3 years |
| HPV Self-sampling | ~88-94% | ~88-92% | High | Moderate | Yes | 3-5 years |
9. Primary Screening: Preferred Method and Why
Current Recommendation: Primary HPV Testing
All major guidelines as of 2025 prefer primary HPV testing as the first-line screening method:
| Organization | Preferred Method | Age | Interval |
|---|---|---|---|
| ACS (2025 update) | Primary HPV testing | 25-65 years | Every 5 years |
| USPSTF (2018, still current) | Cytology alone OR HPV alone OR co-testing | 21-65 years | 3 years (cytology), 5 years (HPV or co-test) |
| WHO (2021) | HPV DNA testing | 30-49 years (priority) | Every 5-10 years |
| ASCCP/ACOG/SGO | Primary HPV testing preferred | 25-65 years | 5 years |
Why HPV primary screening is preferred:
- Superior sensitivity (88-97% vs. 47-62% for cytology) - detects more true cases
- Very high NPV (>99%) - confidently excludes disease, allowing longer intervals
- Longer reassurance period - a negative HPV test predicts very low risk for 5+ years
- Objective test - not affected by sampling or slide preparation artifacts
- Genotyping capability - identifies HPV 16/18 positive women who need immediate colposcopy
- Extended interval - every 5 years reduces patient burden and healthcare costs
- Self-sampling option - 2024-2025 FDA approvals allow home-based or clinic-based self-collection, improving access
The ACS December 2025 update specifically introduced self-collected vaginal specimens as an acceptable option for HPV testing. Clinician-collected cervical specimens are preferred (repeat every 5 years), but self-collected specimens can be used (repeat every 3 years when HPV negative).
If Primary HPV Testing Is Unavailable:
- Co-testing (HPV + cytology) every 5 years: acceptable alternative
- Cytology alone every 3 years: least preferred option in resource-adequate settings
10. Cervical Screening in Low-Resource Settings
WHO Recommended Approach: "Screen-and-Treat"
The WHO recommends a screen-and-treat (or screen, triage, and treat) strategy to minimize the number of clinic visits and reduce loss to follow-up.
Preferred Strategy Hierarchy (WHO 2021)
| Priority | Method | Comment |
|---|---|---|
| 1st choice | HPV DNA testing (screen) + treat screen-positives | Best if molecular capacity available |
| 2nd choice | VIA (screen) + immediate cryotherapy or LEEP | "See-and-treat" same-day approach |
| 3rd choice | Cytology (screen) + colposcopy (diagnose) + treat | Requires multiple visits |
Specific Low-Resource Screening Methods
VIA as the Primary Tool
- No laboratory required
- Immediate results
- Enables same-visit treatment (cryotherapy)
- Cost: ~$1-5 per woman screened
- Can be performed by trained nurses or midwives
Point-of-Care HPV Testing
Newer molecular platforms (Xpert HPV by Cepheid, careHPV by Qiagen) provide near-patient HPV testing in 1-3 hours without a sophisticated lab infrastructure. These are transforming low-resource screening:
- Sensitivity comparable to standard lab HPV tests (90%+)
- Can be used at district hospitals or health centers
- The WHO now includes these as part of recommended strategies in LMICs
HPV Self-Sampling
- Patient collects vaginal swab herself (privately, in a clinic bathroom, or at home)
- Sample mailed or brought for HPV testing
- Sensitivity and specificity approach clinician-collected sample (~88-94% sensitivity)
- Dramatically increases coverage among women who avoid pelvic examination
- Several sub-Saharan African and Latin American studies show promising results for self-sampling in low-resource populations
VILI
Used as an alternative or adjunct to VIA, particularly when colposcopy is unavailable. Results immediately visible; slightly higher sensitivity than VIA in some studies.
WHO-Recommended Algorithms for Low-Resource Settings
Algorithm 1: HPV-based screen-and-treat (where molecular capacity exists)
HPV Test
├── Negative → Reassure, next test in 5 years
└── Positive →
├── Visually inspect (VIA/VILI) or triage cytology
│ ├── Negative on triage → Retest in 1 year
│ └── Positive on triage → Treat (cryotherapy/LEEP)
Algorithm 2: VIA-based screen-and-treat (lowest resource)
VIA
├── Negative → Reassure, next VIA in 2-3 years
└── Positive →
├── Eligible for cryotherapy → Treat same visit
└── Not eligible (large lesion, extends into canal) → LEEP referral
Practical Considerations for Low-Resource Settings
| Factor | Consideration |
|---|---|
| Training | VIA/VILI can be taught to nurses and community health workers in 2-3 days |
| Equipment | Only a speculum, lamp, cotton swabs, acetic acid - minimal investment |
| Follow-up | Screen-and-treat avoids need for multiple visits |
| Cost-effectiveness | VIA + cryotherapy is highly cost-effective in LMICs |
| Overtreatment | VIA's low specificity means ~20-50% of screen-positives treated unnecessarily, but benefits outweigh harms |
| Cold chain | VIA/VILI requires no cold chain; LBC and HPV kits may need temperature-controlled storage |
11. Colposcopy (Diagnostic, Not Primary Screening)
Colposcopy is performed after an abnormal screening result - it is not a primary screening tool. The cervix is examined with a magnifying colposcope (10-40x) after applying acetic acid. Acetowhite areas, vascular patterns (punctation, mosaic, atypical vessels), and abnormal transformation zones are identified. Targeted biopsies are taken.
12. Special Populations
| Population | Screening Approach |
|---|---|
| HIV positive women | Cytology preferred; begin within 1 year of HIV diagnosis; annual smears until 3 consecutive negatives; HPV co-testing added after age 30 |
| Immunocompromised (transplant, long-term steroids) | Annual cytology |
| DES daughters | Annual cytology beginning at age 21 |
| Post-hysterectomy (benign indication, no CIN history) | Can discontinue screening |
| Age <21 years | No screening regardless of sexual activity onset |
| Age >65 (adequate prior negative screening) | Discontinue screening per ACS 2025: require two negative HPV tests (or co-tests) at ages 60 and 65 |
| Pregnant women | Pap smear safe during pregnancy; biopsy if HSIL suspected |
13. Cytopathology of CIN: What Is Seen on the Pap Smear
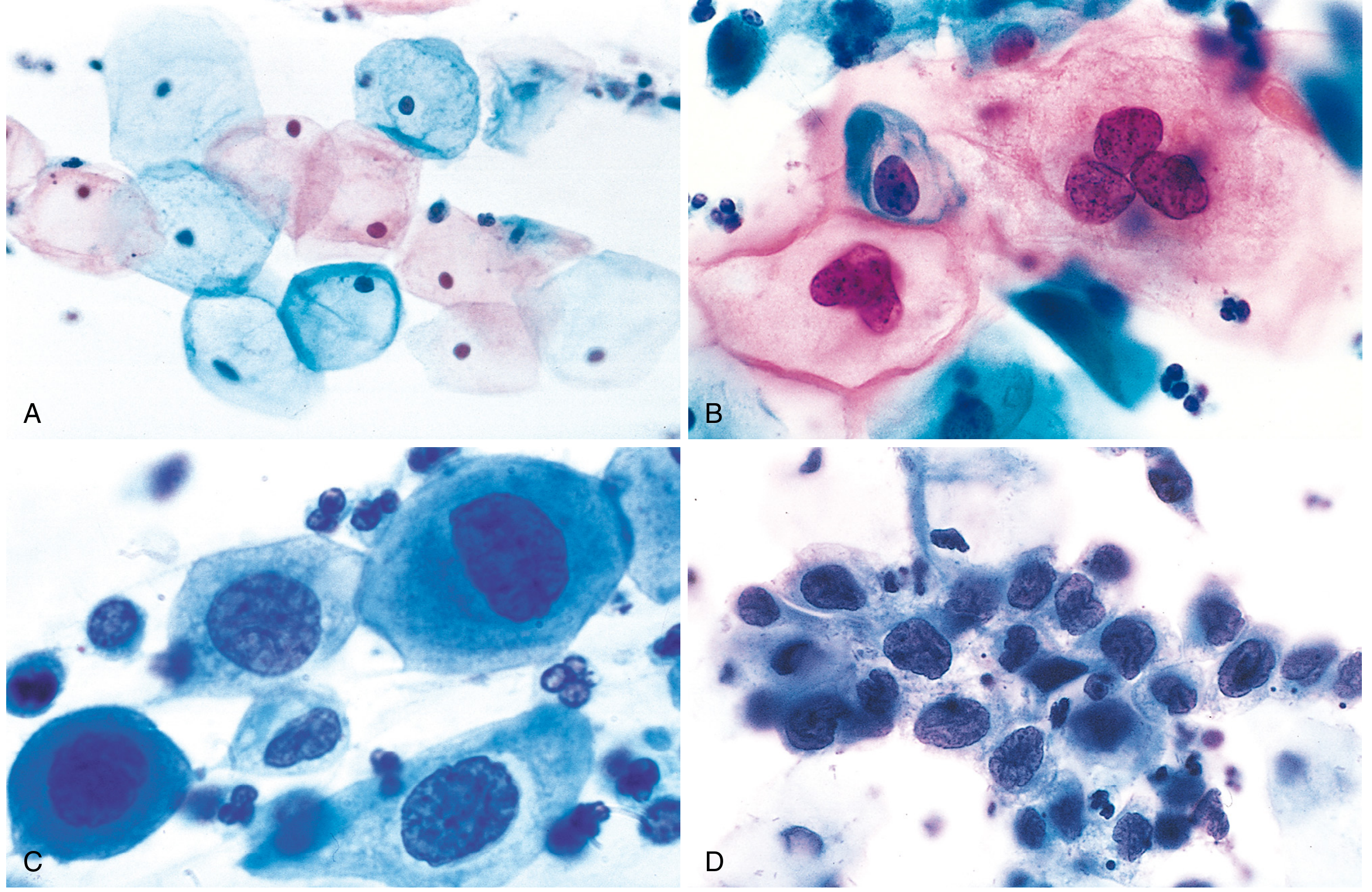
Fig: Cytology of cervical intraepithelial neoplasia on Papanicolaou smear. (A) Normal superficial squamous cells. (B) Low-grade SIL - koilocytes with perinuclear halos. (C) High-grade SIL - enlarged nucleus, reduced cytoplasm. (D) HSIL - clusters with marked nuclear enlargement and high N:C ratio. (From Robbins & Cotran Pathologic Basis of Disease)
14. Summary: Choosing the Right Screening Approach
| Context | Recommended Method |
|---|---|
| High-resource setting, any age 25-65 | Primary HPV testing every 5 years (preferred) |
| Unavailability of primary HPV testing | Co-testing every 5 years OR cytology every 3 years |
| Women 21-24 years | Cytology alone every 3 years (HPV testing not recommended due to high prevalence of transient infection) |
| Low-resource, no molecular lab | VIA ± same-visit cryotherapy |
| Low-resource, near-patient HPV capability | Xpert HPV / careHPV + screen-and-treat |
| Hard-to-reach populations | HPV self-sampling |
| HIV-positive women | Cytology (± HPV co-testing ≥30 years) |
Key Takeaway: Primary HPV testing every 5 years is now the global preferred standard for cervical screening in resource-adequate settings, driven by its superior sensitivity, very high negative predictive value, and the ability to extend screening intervals safely. In low-resource settings, the WHO promotes VIA-based screen-and-treat as a pragmatic, effective alternative, with point-of-care HPV testing increasingly bridging the gap.
Sources:
- Berek & Novak's Gynecology, 16th ed., pp. 845-846
- Harrison's Principles of Internal Medicine, 22nd ed. (2025), pp. 1573-1574
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 925-926
- ACS Cervical Cancer Screening Guidelines Update, December 2025
- Pillay J et al. (2025). Systematic review for Canadian Task Force on Preventive Health Care cervical screening update [PMID: 41152983]
- Wentzensen N et al. (2025). Self-collected vaginal specimens for HPV testing - ASCCP enduring guidelines [PMID: 39982254]
- Perkins RB et al. (2026). ACS cervical cancer screening guideline update: self-collection and screening exit [PMID: 41342729]
This is a shared conversation. Sign in to Orris to start your own chat.