Detailed information about blood indices in pregnancy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"blood indices" AND pregnancy
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer:
Blood Indices in Pregnancy
Pregnancy induces profound and well-characterized changes across every blood parameter. These are physiologic adaptations - not pathology - and understanding them is essential for interpreting lab results in pregnant patients.
1. Blood Volume
The single most important change underpinning nearly all hematologic shifts in pregnancy is the dramatic expansion of blood volume.
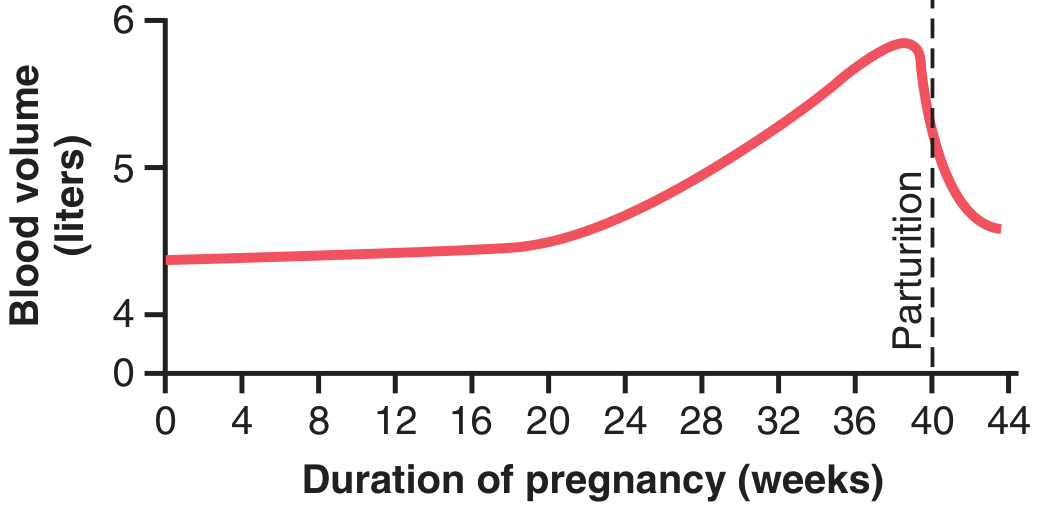
Figure: Effect of pregnancy on maternal blood volume (Guyton and Hall Textbook of Medical Physiology)
- Total blood volume increases by 40-50% above pre-pregnancy baseline by term in singleton pregnancies; up to 75-100% in twin or triplet pregnancies
- Plasma volume begins expanding in the first trimester, rises rapidly in the second, and plateaus in the late third trimester - ultimately increasing by ~50%
- Red cell mass also expands, but by only ~20-33%, and lags behind plasma expansion
- This disproportionate rise in plasma vs. red cells is the mechanism of physiologic (dilutional) anemia of pregnancy
- Aldosterone (stimulated by the renin-angiotensin system) and estrogen drive sodium and water retention; progesterone causes vasodilation and reduced peripheral resistance, stimulating the compensatory volume expansion
- After delivery of the placenta, progesterone and estrogen drop sharply, triggering vigorous diuresis
- Guyton and Hall Textbook of Medical Physiology; Medical Physiology (Boron & Boulpaep)
2. Red Blood Cell (RBC) Indices
Hemoglobin & Hematocrit
The most clinically referenced indices - the hemoglobin and hematocrit fall as a result of hemodilution. This dilutional anemia is physiologic, not pathologic, when it meets the following thresholds:
| Trimester | Hemoglobin (minimum normal) |
|---|---|
| First trimester (late) | ≥ 11 g/dL |
| Second & Third trimesters | ≥ 10 g/dL |
A hemoglobin above these thresholds in an otherwise uncomplicated pregnancy can be attributed to physiologic anemia without further workup. Values below these thresholds, or a microcytic/macrocytic picture, require evaluation for iron deficiency, folate deficiency, or other pathology.
The relative anemia peaks at 32-34 weeks of gestation, when plasma volume expansion is greatest relative to red cell mass expansion.
RBC Count (Reference Ranges by Trimester)
| Trimester | RBC Count |
|---|---|
| First | 3.42 - 4.55 × 10¹²/L |
| Second | 2.81 - 4.49 × 10¹²/L |
| Third | 2.72 - 4.43 × 10¹²/L |
MCV (Mean Corpuscular Volume)
| Trimester | MCV |
|---|---|
| First | 81 - 96 μm³ |
| Second | 82 - 97 μm³ |
| Third | 81 - 99 μm³ |
MCV is relatively stable across pregnancy. A rise suggests folate or B12 deficiency; a fall points to iron deficiency.
MCHC (Mean Corpuscular Hemoglobin Concentration)
- Normal throughout pregnancy: 32-35 g/dL
- Does not change significantly with hemodilution
Reticulocyte Count
- 48-152 × 10⁹/L (0.5%-1.5%)
- A modest reticulocytosis reflects the increased erythropoietic drive in response to expanding blood volume
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, Table 55.1; Goldman-Cecil Medicine
3. Iron Studies
Iron demand increases substantially in pregnancy (transfer of ~500 mg iron to the fetus - equivalent to about 2 units of blood). Iron deficiency is the most common cause of true (non-physiologic) anemia in pregnancy.
| Test | First Trimester | Second Trimester | Third Trimester |
|---|---|---|---|
| Serum Ferritin | > 20 μg/L (72-143 μg/dL) | - | - |
| Serum Iron | 44-178 μg/dL | 44-178 μg/dL | 30-193 μg/dL |
| TIBC (Total Iron-Binding Capacity) | 235-408 μg/dL | 302-519 μg/dL | 580-597 μg/dL |
| Transferrin Saturation | 16%-60% | 16%-60% | 16%-60% |
Key pattern in iron deficiency: serum iron decreases, TIBC increases, transferrin saturation decreases, ferritin decreases.
Note: TIBC rises progressively through pregnancy even in iron-replete women, reflecting increased transferrin synthesis driven by estrogen.
- Creasy & Resnik's Maternal-Fetal Medicine, Table 55.1
4. Folate and Vitamin B12
Folate demand increases during pregnancy (for fetal neural tube development and increased cell turnover). Deficiency causes macrocytic anemia.
| Test | First Trimester | Second Trimester | Third Trimester |
|---|---|---|---|
| Serum Folate | 26-150 μg/L | 8-240 μg/L | 14-207 μg/L |
| RBC Folate | 137-589 ng/mL | 94-828 ng/mL | 109-663 ng/mL |
| Serum B12 | 118-438 pg/mL | 130-656 pg/mL | 99-526 pg/mL |
- The 0.8 mg/day folate supplementation recommended for neural tube defect prophylaxis is generally sufficient to prevent folate deficiency anemia in countries with food fortification
- Anti-intrinsic factor antibody should be negative; a positive result suggests pernicious anemia
- Creasy & Resnik's Maternal-Fetal Medicine, Table 55.1
5. White Blood Cells (Leukocytes)
Leukocytosis is a normal, physiologic feature of pregnancy and should not be automatically attributed to infection.
| Period | WBC Range |
|---|---|
| First trimester | 3,000 - 15,000 cells/mm³ |
| Second & Third trimesters | 6,000 - 16,000 cells/mm³ |
| Labor | Further rise; degree proportional to duration of labor |
| Normal non-pregnant | 4,500 - 11,000 cells/mm³ |
- The upper limit of normal extends to 13,000-16,000/mm³ during pregnancy
- The WBC elevation is predominantly neutrophilia - immature neutrophil forms (bands, metamyelocytes) may appear on the peripheral smear
- WBC begins to decline in the first postpartum week but may take weeks to months to fully normalize
- This physiologic leukocytosis is an important caveat when diagnosing infection - a WBC of 12,000-14,000 alone does not confirm sepsis in a pregnant or laboring patient
- Miller's Anesthesia 10e; Sabiston Textbook of Surgery; Barash Clinical Anesthesia 9e
6. Platelets
Platelet count has a progressive, mild decline throughout pregnancy due to two mechanisms: hemodilution and increased platelet consumption/turnover (from low-grade activation in the uteroplacental circulation).
| Finding | Value |
|---|---|
| Normal platelet count | 150,000 - 450,000/mm³ |
| Expected decline by term | ~10% |
| Prevalence of platelets < 150,000/mm³ in healthy pregnant women | ~8-10% |
| Gestational thrombocytopenia floor | Usually > 70,000/mm³ |
| Mean platelet volume (MPV) | Tends to increase after 28 weeks |
- Gestational thrombocytopenia (GT) is the most common cause of low platelets in pregnancy, accounting for ~75% of cases. It is a diagnosis of exclusion, carries no bleeding risk, and resolves spontaneously postpartum
- A platelet count > 115,000/mm³ late in pregnancy generally does not require further evaluation in otherwise healthy women
- Platelet counts of 75,000-100,000/mm³ are not considered a significant surgical risk unless dysfunction is present
- GT must be distinguished from more serious causes: ITP, preeclampsia/HELLP syndrome, TTP, HUS
- Textbook of Family Medicine 9e; Miller's Anesthesia 10e; Sabiston Textbook of Surgery
7. Coagulation Indices - Hypercoagulable State
Pregnancy creates a physiologic hypercoagulable state - a protective adaptation against hemorrhage at delivery - by increasing procoagulants, decreasing anticoagulants, and reducing fibrinolysis.
Coagulation Factors
| Factor | Change in Pregnancy |
|---|---|
| Fibrinogen (Factor I) | Markedly increased: 400-500 mg/dL (vs. 200-400 mg/dL non-pregnant) |
| von Willebrand Factor | Increased |
| Factors II, V | Unchanged |
| Factors VII, VIII, IX, X, XII | Increased |
| Factor XI | Decreased |
| Factor XIII | Decreased |
Anticoagulants
| Parameter | Change |
|---|---|
| Protein S | Decreased |
| Protein C | Unchanged |
| Antithrombin III | Decreased |
| Resistance to activated Protein C | Decreased (acquired) |
Fibrinolysis
- Plasminogen activator inhibitor 1 (PAI-1) increases
- Placental PAI-2 also increases
- Net result: decreased fibrinolysis, contributing to the procoagulant state
Global Clotting Tests
| Test | Change |
|---|---|
| PT (Prothrombin Time) | ~20% decrease (shortened) |
| PTT (Partial Thromboplastin Time) | ~20% decrease (shortened) |
| APTT | Normal in absence of anticoagulants/coagulopathy |
| INR | Normal |
| Thrombin time (TT) | Normal |
| Bleeding time / clotting time | Unchanged |
Clinical Implications
This hypercoagulable state results in a 5-fold increase in VTE risk during pregnancy, rising to >20-fold in the puerperium. Women with inherited thrombophilias (e.g., Factor V Leiden, prothrombin gene mutation) are at substantially higher risk.
Fibrinogen is also an early predictor of postpartum hemorrhage severity - acute declines should trigger early intervention.
- Sabiston Textbook of Surgery; Miller's Anesthesia 10e; Barash Clinical Anesthesia 9e
8. Other Biochemical Indices Related to the Blood
LDH and Bilirubin
| Test | First Trimester | Second Trimester | Third Trimester |
|---|---|---|---|
| LDH | 78-433 U/L | 80-447 U/L | 82-524 U/L |
| Total Bilirubin | 0.1-0.4 mg/dL | 0.1-0.8 mg/dL | 0.1-1.1 mg/dL |
Elevated LDH and rising bilirubin beyond these ranges should raise concern for hemolysis (especially in the context of HELLP syndrome).
Serum Haptoglobin
- Normal: 30-200 mg/dL
- Decreased in hemolytic states
Hemoglobin Electrophoresis
- Normal: >98% HbA, <3.5% HbA2
- Screening for hemoglobinopathies (sickle cell, thalassemia) is part of routine antenatal care
- Creasy & Resnik's Maternal-Fetal Medicine, Table 55.1
Summary Table: Key Directional Changes
| Index | Direction in Pregnancy | Mechanism |
|---|---|---|
| Blood volume | ↑↑ (+40-50%) | Aldosterone, estrogen, progesterone |
| Plasma volume | ↑↑↑ (+50%) | RAAS activation |
| RBC mass | ↑ (+20-33%) | Increased EPO, bone marrow activity |
| Hemoglobin/Hematocrit | ↓ (dilutional) | Plasma >> RBC expansion |
| MCV | → unchanged | - |
| MCHC | → unchanged | - |
| Reticulocytes | ↑ modest | Erythropoietic drive |
| TIBC | ↑ | Increased transferrin |
| Serum ferritin | ↓ tendency | Increased demand |
| WBC | ↑ (leukocytosis) | Neutrophilia (mechanism unclear) |
| Platelets | ↓ mild | Hemodilution + increased turnover |
| Fibrinogen | ↑↑ | Hepatic synthesis |
| Factors VII, VIII, IX, X | ↑ | Hepatic synthesis, estrogen |
| Protein S, AT-III | ↓ | Consumption, reduced synthesis |
| PT/PTT | ↓ shortened | Procoagulant excess |
| Fibrinolysis | ↓ | PAI-1, PAI-2 increase |
Key clinical takeaways:
- A hemoglobin of 10-11 g/dL can be entirely normal in pregnancy - do not over-investigate without other abnormalities
- A WBC up to 15,000-16,000/mm³ can be normal; interpret infection markers in context
- Platelets commonly drop by ~10% - gestational thrombocytopenia to ~100,000/mm³ is typically benign
- Pregnancy is a prothrombotic state - all procoagulants (except XI and XIII) rise; anticoagulants fall
- Iron and folate stores are regularly consumed by the fetus - supplementation throughout pregnancy is standard practice
Detailed info about MCV,MCHC,MCH in pregnancy and anemia
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"MCV" AND "MCHC" AND pregnancy AND anemia
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive data from multiple authoritative sources. Let me compile the detailed answer.
MCV, MCHC, and MCH in Pregnancy and Anemia
1. Definitions and Calculations
Before applying them to pregnancy, it helps to be precise about what each index measures.
MCV - Mean Corpuscular Volume
- Definition: The average volume of a single red blood cell
- Formula: MCV = Hematocrit (Hct) ÷ RBC count (in millions/μL) × 10
- Units: femtoliters (fL) or cubic micrometers (μm³)
- One fL = 10⁻¹⁵ L = 1 μm³
- In automated counters, MCV is derived directly from the mean height of electrical voltage pulses generated during the red cell count
MCH - Mean Corpuscular Hemoglobin
- Definition: The average mass (weight) of hemoglobin per red cell
- Formula: MCH = Hemoglobin (g/L) ÷ RBC count (×10¹²/L)
- Units: picograms (pg)
- Example: Hb = 15 g/dL (150 g/L), RBC = 5 × 10¹²/L → MCH = 150 ÷ 5×10¹² = 30 pg
- MCH closely parallels MCV - microcytic cells contain less hemoglobin by mass
MCHC - Mean Corpuscular Hemoglobin Concentration
- Definition: The average concentration of hemoglobin per unit volume of packed red cells
- Formula: MCHC = Hemoglobin (g/dL) ÷ Hematocrit × 100
- Units: g/dL
- Example: Hb = 15 g/dL, Hct = 0.45 → MCHC = 15 ÷ 0.45 = 33.3 g/dL
- In automated counters: Hct = MCV × RBC; MCH = Hb/RBC; MCHC = (Hb/Hct) × 100
- Henry's Clinical Diagnosis and Management by Laboratory Methods
2. Normal Reference Values
Non-Pregnant Adults (Baseline)
| Index | Normal Range | Units |
|---|---|---|
| MCV | 80-96 fL | femtoliters |
| MCH | 27-33 pg | picograms |
| MCHC | 33-36 g/dL | g/dL |
| RDW | 11.8-16.1% | % |
(Robbins Basic Pathology; Henry's Clinical Diagnosis)
In Pregnancy - The Key Principle
MCV and MCHC do NOT change with the physiologic hemodilution of pregnancy.
This is the most clinically important fact about these indices in pregnancy:
- Blood volume increases 40-45% by 34 weeks, with plasma volume rising ~47% and RBC mass rising only ~17%
- This disparity causes hemoglobin, hematocrit, and RBC count to fall (dilutional anemia)
- However, because MCV and MCHC reflect the characteristics of individual red cells - not their total number - they remain unchanged by hemodilution
- MCH similarly stays within normal limits in pure physiologic anemia of pregnancy
This is why these indices are so useful in pregnancy: they serve as the key tool to distinguish physiologic (dilutional) anemia from pathologic anemia.
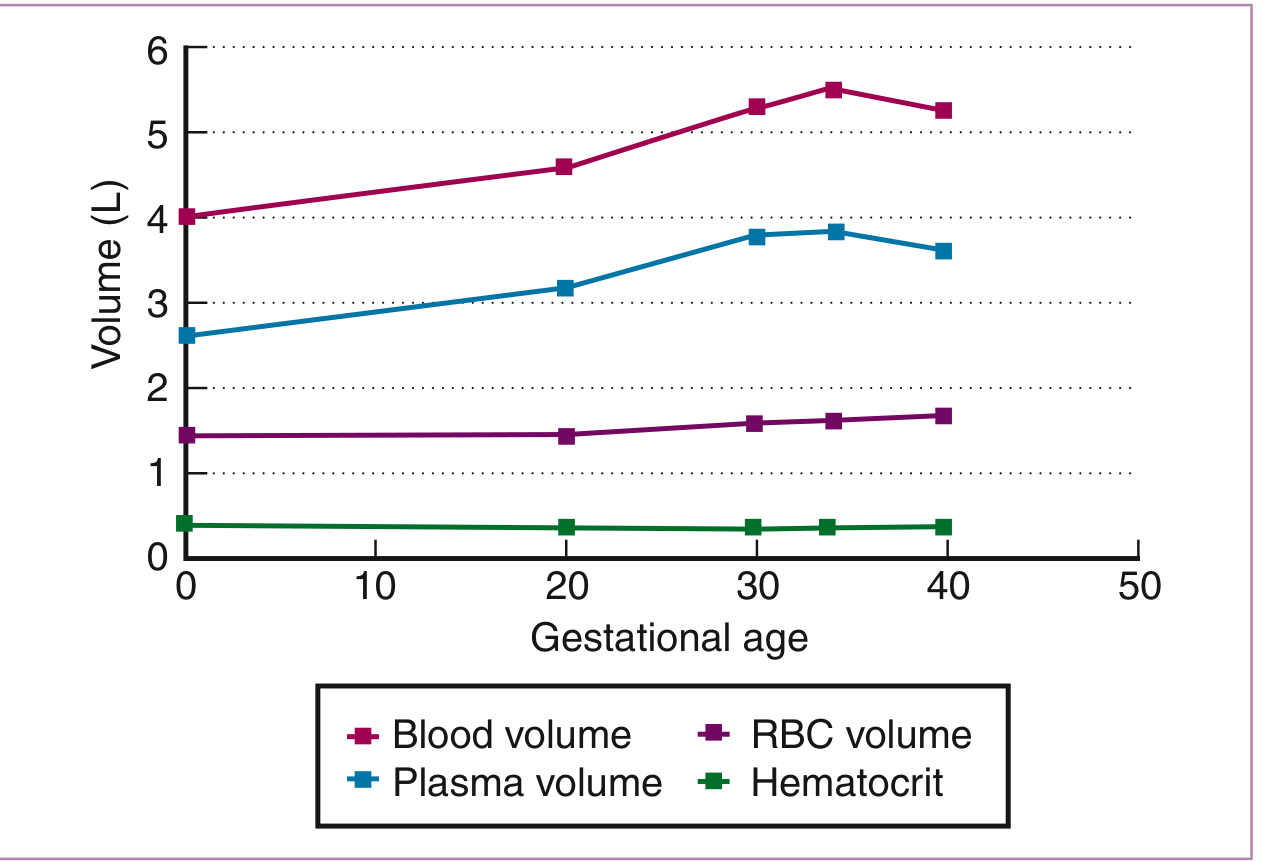
Figure: Hematologic changes during pregnancy. Note that while hematocrit falls progressively due to the greater rise in plasma volume versus RBC volume, the actual red cell indices (MCV, MCHC) remain stable throughout. (Creasy & Resnik's Maternal-Fetal Medicine)
From Creasy & Resnik's Maternal-Fetal Medicine reference table:
| Index | Pregnancy Reference Range |
|---|---|
| MCV (1st trimester) | 81-96 μm³ |
| MCV (2nd trimester) | 82-97 μm³ |
| MCV (3rd trimester) | 81-99 μm³ |
| MCHC | 32-35 g/dL (all trimesters) |
- Creasy & Resnik's Maternal-Fetal Medicine, Table 55.1; Textbook of Family Medicine 9e
3. The Diagnostic Power of Red Cell Indices in Pregnancy
Since MCV, MCH, and MCHC remain stable in physiologic anemia, any deviation from normal indicates pathological anemia requiring workup. Serial monitoring of these two indices is the principal tool for differentiating dilutional anemia from progressive iron deficiency anemia (IDA) during pregnancy.
"Serial evaluation of these two indices is useful in differentiating dilutional anemia from progressive IDA during pregnancy. In the former, indices do not change, and in the latter, they decrease progressively." - Creasy & Resnik's Maternal-Fetal Medicine
4. MCV, MCH, MCHC in Each Type of Anemia in Pregnancy
A. Iron Deficiency Anemia (IDA) - Microcytic, Hypochromic
The most common cause of pathologic anemia in pregnancy (75% of all anemias; prevalence up to 47%)
Iron demands during pregnancy are enormous - up to 500 mg is actively transferred to the fetus regardless of maternal stores. Many women enter pregnancy with borderline or depleted iron stores.
Red Cell Indices Pattern:
| Index | Finding | Severity Range |
|---|---|---|
| MCV | ↓ Low (microcytic) | Can fall to 50 fL in severe IDA |
| MCH | ↓ Low (hypochromic) | Can fall to 15 pg |
| MCHC | ↓ Low (hypochromic) | Can fall to 22 g/dL; rarely below |
| RDW | ↑ Elevated (anisocytosis) | RDW rises early - often before MCV falls |
Sequential progression of IDA indices (earliest to latest):
- Serum ferritin falls (depleted stores - first change)
- Transferrin saturation falls; TIBC rises
- RDW rises (anisocytosis - RBCs become heterogeneous in size)
- MCV falls (microcytosis develops)
- MCH falls (hypochromia develops)
- MCHC falls (frank hypochromia)
- Hemoglobin falls (anemia becomes manifest)
Note: In early IDA, MCV may be normal. The MCHC is more specific for true iron deficiency because it reflects the concentration of hemoglobin within the cell. Peripheral blood smear shows microcytic, hypochromic RBCs with pencil cells and target cells.
Supporting labs: ↓ serum ferritin, ↓ serum iron, ↑ TIBC, ↓ transferrin saturation (<16%), absent marrow iron staining.
- Creasy & Resnik's Maternal-Fetal Medicine; Henry's Clinical Diagnosis
B. Megaloblastic Anemia (Folate or B12 Deficiency) - Macrocytic
The second most common nutritional anemia in pregnancy
Folate requirements increase dramatically in pregnancy due to rapid cell division. B12 deficiency is less common but must always be considered.
Red Cell Indices Pattern:
| Index | Finding | Value Range |
|---|---|---|
| MCV | ↑↑ Elevated (macrocytic) | Can reach 110-150 fL |
| MCH | ↑ Elevated | Can reach 40-50 pg |
| MCHC | Normal or slightly low | Typically normal (32-36 g/dL) |
| RDW | ↑ Elevated (marked anisocytosis) | - |
Key distinguishing feature: MCHC remains normal (or slightly low) even as MCV rises dramatically. This is because macrocytic cells are large but not overfilled with hemoglobin - they are normochromic.
CBC findings in megaloblastic anemia:
- Macrocytic or normocytic, normochromic anemia
- Hypersegmented neutrophils (≥5 lobes; pathognomonic)
- Low reticulocyte count (aregenerative)
- Thrombocytopenia and leukopenia may be present (pancytopenia in severe cases)
Folate deficiency: Serum folate < 2 μg/L; RBC folate < 165 ng/mL; B12 normal
B12 deficiency: Serum B12 low; folate levels usually normal; anti-intrinsic factor antibody may be positive
Critical warning: Never treat B12 deficiency with folate alone - it corrects anemia but worsens (and may accelerate) the neurological damage to the posterior columns of the spinal cord.
- Creasy & Resnik's Maternal-Fetal Medicine; Barash Clinical Anesthesia 9e
C. Physiologic (Dilutional) Anemia of Pregnancy - Normocytic, Normochromic
| Index | Finding |
|---|---|
| MCV | Normal (81-99 μm³) |
| MCH | Normal |
| MCHC | Normal (32-35 g/dL) |
| Hb | ↓ (≥10 g/dL in 2nd/3rd trimester is acceptable) |
| RDW | Normal |
This is the reassuring pattern - hemodilution lowers Hb/Hct/RBC count, but red cell indices are completely normal. No further investigation is needed if Hb ≥ 11 g/dL (late first trimester) or ≥ 10 g/dL (second and third trimesters).
D. Thalassemia Trait (Minor) - Microcytic, Mildly Hypochromic
Women with beta-thalassemia minor often enter pregnancy with a mildly low MCV and hemoglobin. Pregnancy can magnify this apparent anemia further.
| Index | Finding |
|---|---|
| MCV | ↓ Low (often very low, sometimes < 70 fL) |
| MCH | ↓ Low |
| MCHC | Normal or slightly low |
| RBC count | Normal or elevated (key differentiating feature from IDA) |
| RDW | Normal or mildly elevated |
Mentzer Index (MCV ÷ RBC count): < 13 suggests thalassemia; > 13 suggests IDA. This is a quick bedside differentiator.
Confirming test: Hemoglobin electrophoresis shows elevated HbA2 > 3.5% in beta-thalassemia trait.
E. Anemia of Chronic Disease (ACD) / Anemia of Inflammation
Less common in pregnancy but possible in women with autoimmune conditions or chronic infections.
| Index | Finding |
|---|---|
| MCV | Normal or mildly ↓ (normocytic to mildly microcytic) |
| MCH | Normal or mildly low |
| MCHC | Normal |
Serum ferritin is normal or elevated (acute phase reactant); TIBC is low or normal; serum iron is low. This distinguishes ACD from IDA.
F. Hereditary Spherocytosis - Normocytic with Elevated MCHC
| Index | Finding |
|---|---|
| MCV | Normal or slightly low |
| MCH | Normal |
| MCHC | ↑ Elevated (often > 36 g/dL) |
Elevated MCHC is the classic signature of hereditary spherocytosis - the only common condition where MCHC rises significantly. Spherocytes have reduced surface area, making them appear densely hemoglobinized. MCHC rarely exceeds 38 g/dL in any condition.
5. Summary: MCV/MCH/MCHC Pattern Recognition in Pregnancy
| Anemia Type | MCV | MCH | MCHC | RDW | Key Clue |
|---|---|---|---|---|---|
| Physiologic (dilutional) | Normal | Normal | Normal | Normal | Hb mildly low; indices all normal |
| Iron deficiency (IDA) | ↓ Low | ↓ Low | ↓ Low | ↑ High | Ferritin low, TIBC high |
| Folate/B12 deficiency | ↑ High | ↑ High | Normal | ↑ High | Hypersegmented neutrophils |
| Thalassemia trait | ↓↓ Very low | ↓ Low | Normal/low | Normal | High RBC count, HbA2 elevated |
| Anemia of chronic disease | Normal/↓ | Normal | Normal | Normal | Ferritin normal/high |
| Hereditary spherocytosis | Normal/↓ | Normal | ↑ High | ↑ | MCHC >36 g/dL |
| Hemolytic anemia | Normal/↑ | Normal | Normal | ↑ | ↑ LDH, ↓ haptoglobin, + Coombs |
6. The Critical Diagnostic Rule
The single most practical clinical rule for interpreting these indices in pregnancy:
- MCV and MCHC do not change with physiologic anemia - if either falls, this signals pathological anemia (most likely IDA) requiring full iron studies
- A rising MCV in pregnancy is never physiologic - investigate for folate or B12 deficiency
- An elevated MCHC is never physiologic - consider spherocytosis or artifact
- RDW rises before MCV changes in IDA - it is a useful early marker
- The peripheral blood smear remains the most informative single test, directly showing cell morphology
- Creasy & Resnik's Maternal-Fetal Medicine; Textbook of Family Medicine 9e; Henry's Clinical Diagnosis and Management by Laboratory Methods; Robbins Basic Pathology
Explain about hematocrit
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have comprehensive textbook content to deliver a thorough answer. Let me compile it.
Hematocrit (Hct) - Comprehensive Explanation
1. Definition
The hematocrit (Hct) is the proportion (ratio) of the total blood volume that is occupied by red blood cells. It is expressed as either a percentage (%) or as a decimal fraction (L/L in SI units).
- The name comes from the graduated tube ("hematocrit tube") originally used to centrifuge blood for the measurement
- It is also called the Packed Cell Volume (PCV) - the two terms are interchangeable
"The percentage of the blood column represented by red cells compressed by centrifugation (also called packed cell volume) is the quantity physically represented by the hematocrit." - Goldman-Cecil Medicine
2. How It Is Measured
Method 1: Centrifugation (Microhematocrit / Macrohematocrit)
This is the direct, classical method.
Procedure (Microhematocrit):
- Blood is collected in EDTA (or heparinized) capillary tube (~7 cm long, ~1 mm bore)
- The tube is filled by capillary attraction to at least 5 cm; the empty end is sealed with clay
- Centrifuged at 10,000-12,000 g for 5 minutes (extra 5 min if Hct >50%)
- The packed red cell column height is read relative to total blood column height using a calibrated reading device
The result is read directly from the percentage scale:
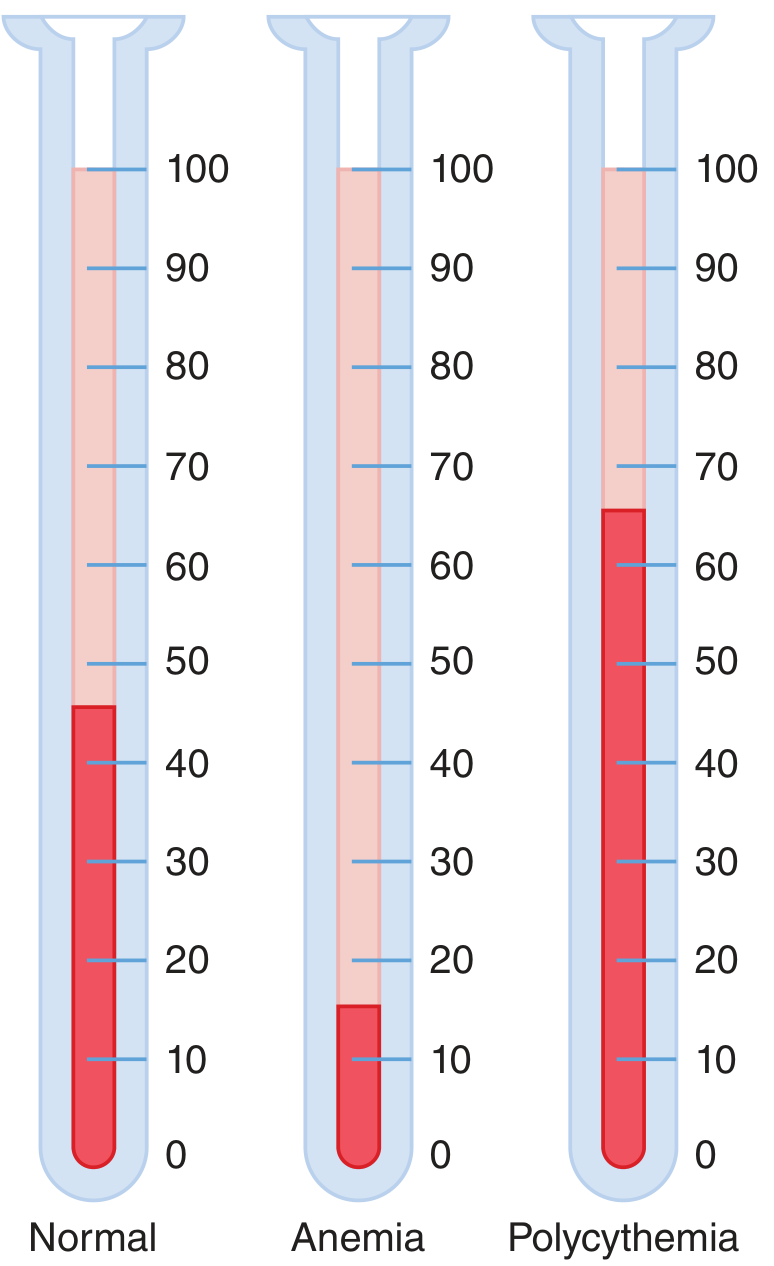
Figure: Hematocrit values in a normal person (left), anemia (center), and polycythemia (right). Numbers represent the percentage of blood composed of red blood cells. (Guyton and Hall Textbook of Medical Physiology)
Method 2: Calculated by Automated Cell Counters (most labs today)
In modern electronic hematology analyzers, Hct is not measured directly but calculated:
Hct = MCV × RBC count ÷ 10
- MCV (mean corpuscular volume, in fL) and RBC count (×10¹²/L) are measured directly
- Hematocrit is derived from their product
- Because hemoglobin is directly measured (not calculated), many clinicians prefer hemoglobin over hematocrit for defining anemia
The "Rule of Three" is a useful bedside check for internal consistency of the CBC when red cells are normal in size and shape:
- RBC × 3 ≈ Hemoglobin
- Hemoglobin × 3 ≈ Hematocrit (%)
- Tietz Textbook of Laboratory Medicine 7th Edition; Henry's Clinical Diagnosis
3. Normal Reference Values
| Population | Hematocrit (%) |
|---|---|
| Adult men | 41 - 51% (avg ~42%) |
| Adult women (non-pregnant) | 36 - 45% (avg ~38%) |
| Pregnant women | Lower (see below) |
| Newborns | ~44-64% (highest due to fetal erythropoiesis) |
- Men have a higher Hct than women due to testosterone-driven erythropoiesis
- Values also vary with altitude (higher altitude → higher Hct due to hypoxic stimulus)
- Level of physical activity influences Hct
4. What the Three Layers Look Like After Centrifugation
After centrifugation, blood separates into three visible layers:
| Layer | Contents | Appearance |
|---|---|---|
| Bottom (packed cell column) | Red blood cells | Dark red; this is the Hct |
| Middle (buffy coat) | Leukocytes + platelets | Thin white/gray layer |
| Top (plasma) | Plasma | Yellow/straw colored |
Abnormal plasma color clues:
- Orange or green plasma → elevated bilirubin
- Pink or red plasma → hemoglobinemia (hemolysis)
- Cloudy/lipemic plasma → hyperlipidemia (especially postprandial)
- Henry's Clinical Diagnosis and Management by Laboratory Methods
5. Physiological Significance: Hematocrit and Blood Viscosity
The hematocrit is one of the most important determinants of blood viscosity, which in turn governs vascular resistance and blood flow according to Poiseuille's law.
- At normal Hct (~40%), whole blood viscosity is approximately 3-4 times that of water
- As Hct rises, viscosity increases exponentially
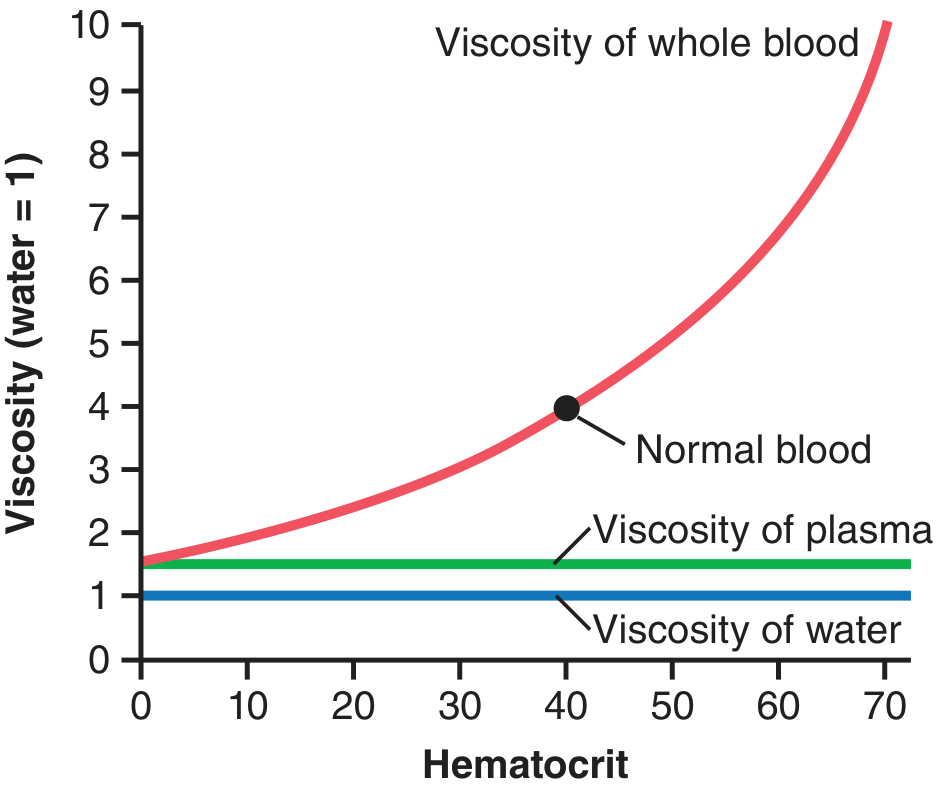
Figure: Effect of hematocrit on blood viscosity (water = 1). Normal blood at Hct ~40 has viscosity ~3-4. At Hct 60-70 (polycythemia), viscosity can reach 10×. (Guyton and Hall Textbook of Medical Physiology)
Clinical implication: In polycythemia (Hct 60-70%), blood viscosity can reach 10 times that of water, severely impeding flow through vessels and raising the risk of thrombosis, stroke, and hyperviscosity syndrome. Conversely, in severe anemia, blood viscosity drops, which reduces resistance but impairs oxygen delivery.
6. Hematocrit and Oxygen Delivery
Hematocrit is a major determinant of oxygen-carrying capacity of blood. Oxygen delivery (DO₂) is expressed by the Fick equation:
DO₂ = Cardiac Output × (Hb concentration × 1.34 × SaO₂ + 0.003 × PaO₂)
Since Hct directly reflects the hemoglobin mass per unit blood volume, it determines how much oxygen each milliliter of blood can carry. However, the relationship is not linear for flow - there is an optimal Hct (~30-35%) that balances oxygen-carrying capacity against viscosity-related flow resistance. This is why clinicians target Hb 7-9 g/dL (Hct ~21-27%) in many critical care transfusion protocols.
7. Clinical Interpretation: High and Low Hematocrit
Low Hematocrit (< normal for age/sex) = Anemia
| Cause | Mechanism |
|---|---|
| Iron deficiency | Insufficient Hb synthesis → small, fewer RBCs |
| Folate/B12 deficiency | Impaired DNA replication → fewer RBCs produced |
| Hemodilution (pregnancy) | Plasma expansion >> RBC expansion |
| Hemorrhage | Absolute red cell loss |
| Hemolysis | Premature red cell destruction |
| Chronic disease/inflammation | Suppressed erythropoiesis |
| Renal failure | Reduced erythropoietin |
| Bone marrow failure | Aplasia, leukemia, infiltration |
Important caveat - Hct is unreliable in two clinical situations:
- Immediately after acute blood loss - plasma and cells are lost proportionally; Hct may be falsely normal until hemodilution from extravascular fluid occurs (takes hours)
- Immediately after transfusion - Hct transiently reflects infused blood, not steady state
- Shock/hemoconcentration - Hct may be normal or high even though total red cell mass is reduced (plasma has been lost into tissues)
High Hematocrit (> normal) = Polycythemia or Hemoconcentration
| Cause | Type |
|---|---|
| Dehydration / fluid loss | Relative (spurious) - plasma depleted, RBC mass normal |
| High altitude residence | Physiologic - hypoxia drives EPO |
| Polycythemia vera | Pathologic - autonomous RBC overproduction |
| Secondary polycythemia | EPO-driven (COPD, sleep apnea, renal tumors) |
| Neonatal period | Physiologic - fetal erythropoiesis |
8. Hematocrit in Pregnancy
Pregnancy is the most common physiologic cause of a low Hct in women of reproductive age.
Mechanism: Plasma volume increases ~47%, but RBC mass increases only ~17%. This disproportionate expansion produces dilutional (physiologic) anemia, with the Hct falling progressively.
| Period | Hct Change |
|---|---|
| First trimester | Begins to fall |
| Peak dilution | 28-34 weeks gestation |
| Non-physiologic threshold | Hct < 33% is considered non-physiologic anemia |
The Hct in pregnancy is low, but the total red cell mass is not reduced - this is hemodilution, not true anemia. The critical point: while Hct and Hb fall, MCV and MCHC remain normal. Any fall in MCV or MCHC indicates superimposed iron deficiency or other pathology.
- Henry's Clinical Diagnosis; Textbook of Family Medicine 9e
9. Sources of Measurement Error
| Error Type | Effect |
|---|---|
| Inadequate centrifugation | Falsely high Hct (incomplete packing) |
| Trapped plasma | Falsely high Hct (+1-3% in normal blood; more in sickle cell, spherocytosis) |
| Excess EDTA anticoagulant | Falsely low Hct (cell shrinkage) - Hb and RBC counts not affected |
| Prolonged tourniquet stasis | Falsely high Hct (hemoconcentration at the venipuncture site) |
| Standing blood (room temp >6 hrs) | Falsely high Hct (erythrocyte swelling raises MCV and Hct) |
| Buffy coat inclusion | Falsely high Hct if white layer counted as red cells |
| K₃-EDTA vs K₂-EDTA | K₃-EDTA shrinks cells ~2%, lowering Hct slightly |
Precision: With good technique, CV (coefficient of variation) = ±1% for Hct.
- Henry's Clinical Diagnosis and Management by Laboratory Methods
10. Relationship Between Hct, Hb, and RBC - Summary
| Parameter | Formula | Normal Adult Male | Normal Adult Female |
|---|---|---|---|
| Hematocrit (Hct) | MCV × RBC ÷ 10 | 41-51% | 36-45% |
| Hemoglobin (Hb) | Directly measured | 13.2-16.6 g/dL | 11.6-15.0 g/dL |
| RBC count | Directly measured | 4.4-5.6 × 10⁶/μL | 3.9-5.1 × 10⁶/μL |
| Rule of Three check | Hb × 3 ≈ Hct | 15 × 3 = 45% ✓ | 12 × 3 = 36% ✓ |
Key relationships to remember:
- Hct reflects red cell concentration in blood, not total red cell mass
- Hb is preferred over Hct for defining and monitoring anemia because it is directly measured (not calculated)
- MCV and MCHC are independent of hemodilution - they reflect the quality of individual cells
- The triad of Hct + Hb + MCV together characterizes the nature and likely cause of anemia
- Goldman-Cecil Medicine; Guyton and Hall Textbook of Medical Physiology; Tietz Textbook of Laboratory Medicine 7th Edition; Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.