Kindly provide the full detail diagnosis and comparison the deviation from normal. And provide the exact problem in cerebellum structure with pictures also
VNG videonystagmography saccade smooth pursuit gaze test interpretation abnormal findings cerebellar central vestibular
cerebellar oculomotor dysfunction saccade dysmetria gaze-evoked nystagmus smooth pursuit impairment flocculus vermis
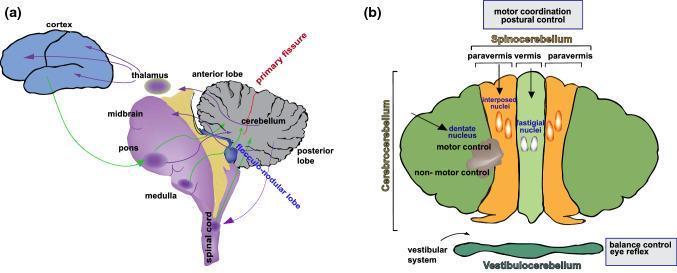
cerebellar anatomy flocculonodular lobe vermis hemispheres vestibulo-cerebellum oculomotor control diagram
subjective visual vertical deviation otolith utricular dysfunction tilt vestibular
cerebellar lesion flocculus nodulus vestibulo-ocular reflex gaze nystagmus MRI pathology
VNG Report — Full Diagnostic Analysis
Patient: A K Bhardwaj | Male, 67 years | Date: 04-Apr-2026
SECTION 1: TEST-BY-TEST FINDINGS WITH NORMAL COMPARISON
1. SACCADE TEST (Rapid Eye Movement Accuracy)
| Parameter | Patient Value | Normal Range | Status |
|---|---|---|---|
| Horizontal Velocity – Right Eye | 474 °/s | 200–700 °/s | ✅ Normal |
| Horizontal Velocity – Left Eye | 810 °/s | 200–700 °/s | ⚠️ HIGH |
| Horizontal Precision (both eyes) | 72–71 | >80% | ⚠️ LOW (undershoot) |
| Horizontal Latency – Right | 240 ms | 150–250 ms | ✅ Normal |
| Horizontal Latency – Left | 292 ms | 150–250 ms | ⚠️ PROLONGED |
| Vertical Velocity (both eyes) | 157–158 °/s | 200–500 °/s | ⚠️ REDUCED |
| Vertical Precision (both eyes) | 41–46 | >80% | 🔴 SEVERELY LOW |
| Vertical Latency | 258–285 ms | 150–250 ms | ⚠️ PROLONGED |
2. SMOOTH PURSUIT TEST (Tracking Moving Targets)
| Direction | Patient Gain | Normal Gain | Status |
|---|---|---|---|
| Horizontal Rightward | 0.91 / 0.85 | 0.80–1.00 | ✅ Normal |
| Horizontal Leftward | 0.55 / 0.53 | 0.80–1.00 | 🔴 SEVERELY REDUCED |
| Vertical Upward | 0.87 / 0.89 | 0.80–1.00 | ✅ Normal |
| Vertical Downward | 0.89 / 0.95 | 0.80–1.00 | ✅ Normal |
3. OPTOKINETIC TEST (Full-Field Visual Motion Response)
| Stimulus Direction | Patient Gain | Normal | Status |
|---|---|---|---|
| Left-to-Right (both eyes) | 1.07 / 1.01 | 0.80–1.10 | ✅ Normal |
| Right-to-Left (both eyes) | 0.91 / 0.91 | 0.80–1.10 | ✅ Normal |
| Top-to-Bottom | 0.73 / 0.63 | 0.80–1.10 | ⚠️ Mildly reduced |
| Bottom-to-Top | – / 0.08 | 0.80–1.10 | 🔴 SEVERELY REDUCED |
4. GAZE TEST (Holding Eccentric Eye Positions — Gaze-Evoked Nystagmus)
| Position | Finding | Significance |
|---|---|---|
| Center – With Fixation | SPV 6.09 °/s, Amp 1.66°, Freq 1.29 Hz (Right eye) | ⚠️ Low-amplitude nystagmus at center |
| Left Gaze | Vertical SPV -0.53 °/s, Freq 0.75 Hz | ⚠️ Low-amplitude nystagmus |
| Right Gaze | No nystagmus | ✅ Normal |
| Up Gaze | No nystagmus | ✅ Normal |
| Down Gaze | Horizontal SPV 0.60 °/s, Freq 1.37 Hz | ⚠️ Mild nystagmus |
| All positions without fixation | No nystagmus detected | ✅ |
5. NYSTAGMUS TESTS
| Test | Finding | Significance |
|---|---|---|
| Spontaneous (Light) | Absent | ✅ Normal |
| Spontaneous (Dark) | Absent | ✅ No peripheral vestibular asymmetry |
| Head Shake | Absent | ✅ No significant semicircular canal imbalance |
| Hyperventilation | Right eye: SPV 3.67 °/s, Amp 1.42°, Freq 0.99 Hz | ⚠️ Hyperventilation-induced nystagmus (HIN) |
6. DIX-HALLPIKE POSITIONAL TESTS
| Maneuver | Finding | Significance |
|---|---|---|
| DH Right — Supine Head Ext. & Right | No nystagmus | ✅ Right posterior canal BPPV absent |
| DH Right — Sit Head Right (post-return) | Horizontal SPV 15.95 °/s, Amp 5.47° | ⚠️ Significant positional nystagmus |
| DH Left — Sit Head Left | Vertical SPV 3.38 °/s | ⚠️ Mild |
| DH Left — Supine Head Ext. & Left | Vertical SPV -10.90 °/s (R), -2.91 °/s (L) | 🔴 Significant positional nystagmus |
| DH Left — Sit recovery | Vertical SPV 2.20–2.86 °/s bilateral | ⚠️ Persistent |
7. HEAD POSITION TESTS (Static Positional)
| Position | Finding | Significance |
|---|---|---|
| Yaw Right | Left eye vertical SPV 9.85 °/s, Amp 2.60° | ⚠️ Vertical nystagmus in static head position |
| Yaw Left | No nystagmus | ✅ |
| Pitch Backward | Right eye vertical SPV -3.87 °/s | ⚠️ Mild downbeat-type nystagmus |
| Roll Right | Horizontal SPV 4.60 °/s, Amp 2.62° | ⚠️ |
| Roll Left | Horizontal SPV 6.03 °/s, Amp 2.85° | ⚠️ |
| Pitch Forward | No nystagmus | ✅ |
8. SUBJECTIVE VISUAL VERTICAL (SVV)
| Condition | Deviation | Normal | Status |
|---|---|---|---|
| Clockwise background | 90° Right | < 2–3° | 🔴 GROSSLY ABNORMAL |
| Anticlockwise background | 90° Right | < 2–3° | 🔴 GROSSLY ABNORMAL |
| Blank background | 90° Right | < 2–3° | 🔴 GROSSLY ABNORMAL |
SECTION 2: OVERALL DIAGNOSIS
Primary Diagnosis: Central Vestibulocerebellar Dysfunction
| Finding | Cerebellar Structure Implicated |
|---|---|
| Vertical saccade dysmetria (precision 41–46%) | Oculomotor vermis (lobules VI–VII) + fastigial nucleus |
| Asymmetric leftward smooth pursuit failure | Flocculus / paraflocculus (left) |
| Near-absent upward OKN | Dorsal cerebellar vermis + pretectal nucleus |
| Central positional nystagmus (non-fatiguing, multi-directional) | Nodulus + Uvula (lobules IX–X) |
| Gaze-evoked nystagmus at center (fixation-dependent) | Flocculus (neural integrator leakage) |
| Downbeat nystagmus components in pitch-back | Flocculus + Nodulus |
| SVV deviation 90° (catastrophically abnormal) | Nodulus (lobule X) + utricle-brainstem-cerebellar pathway |
| Hyperventilation-induced nystagmus | Vestibular nerve or root entry zone |
| Persistent static positional nystagmus (roll, yaw) | Nodulus + Uvula |
SECTION 3: THE CEREBELLUM — EXACT STRUCTURES INVOLVED
Cerebellar Anatomy Relevant to This Patient
Structures with Established Dysfunction in This Patient:
- Controls smooth pursuit velocity and the "neural integrator" (gaze-holding mechanism)
- This patient: Leftward smooth pursuit gain 0.53–0.55 (severely reduced), gaze-evoked nystagmus at primary position with fixation — classic floccular failure
- Fine-tunes saccade accuracy (precision/metrics); projects to the fastigial oculomotor region
- This patient: Vertical saccade precision 41–46% (catastrophically low); vertical velocity reduced — indicates the cerebellar calibration circuit for saccades is not functioning
- Processes otolith and semicircular canal input; suppresses low-frequency VOR; modulates the plane-specific gravity response
- This patient: Multi-positional non-fatiguing nystagmus, 90° SVV deviation, downbeat components — all hallmark nodular pathology
- Works with the nodulus on spatial orientation and VOR suppression
- This patient: Positional nystagmus persisting in both DH left supine and return positions with bilateral vertical beats
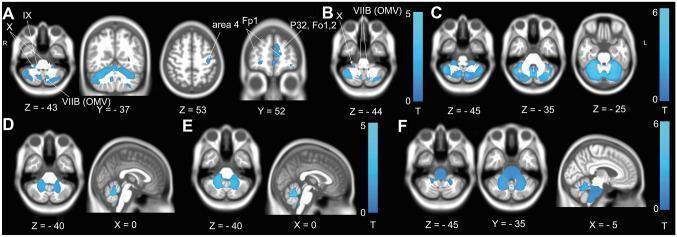
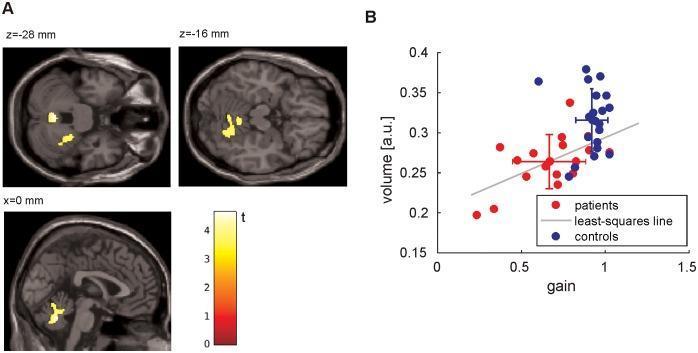
VBM Evidence
SECTION 4: DEVIATION FROM NORMAL — SUMMARY TABLE
| Test | Normal Value | Patient Value | Deviation | Clinical Significance |
|---|---|---|---|---|
| Horizontal saccade precision | >80% | 72–71% | -10% | Mild dysmetria |
| Vertical saccade precision | >80% | 41–46% | -40% 🔴 | Severe oculomotor vermis dysfunction |
| Leftward smooth pursuit gain | >0.80 | 0.53–0.55 | -33% 🔴 | Floccular dysfunction |
| Upward OKN gain | >0.80 | 0.08 | -90% 🔴 | Vertical OKN pathways compromised |
| Gaze-evoked nystagmus | Absent at center | SPV 6.09 °/s present 🔴 | Abnormal | Neural integrator failure (flocculus) |
| Hyperventilation nystagmus | Absent | SPV 3.67 °/s present ⚠️ | Abnormal | Nerve/central demyelination |
| Positional nystagmus (DH) | Transient, fatigable if BPPV | Persistent, multi-directional 🔴 | Central pattern | Nodulus/uvula pathology |
| SVV deviation | ≤2–3° | 90° RIGHT 🔴🔴🔴 | +87° | Catastrophic otolith/central tilt |
| Spontaneous nystagmus | Absent | Absent | Normal ✅ | No acute peripheral decompensation |
| Head shake nystagmus | Absent | Absent | Normal ✅ | No major canal imbalance |
SECTION 5: DIFFERENTIAL DIAGNOSES TO CONSIDER
- Cerebellar degeneration (idiopathic, paraneoplastic, alcohol-related) — most likely given age and pattern
- Cerebellar infarct / vertebrobasilar ischemia — PICA or SCA territory; urgent MRI required
- Spinocerebellar ataxia (SCA) — hereditary; genetic testing warranted
- Multiple System Atrophy – Cerebellar type (MSA-C) — downbeat nystagmus + autonomic features
- Paraneoplastic cerebellar degeneration — anti-Yo, anti-Hu antibodies; screen for occult malignancy
- Vestibular schwannoma — suggested by hyperventilation-induced nystagmus; consider MRI with contrast
SECTION 6: RECOMMENDED NEXT STEPS
- MRI brain with FLAIR + DWI + contrast (posterior fossa protocol) — to evaluate cerebellar lobules IX, X, VI–VII and the flocculus; rule out infarct, mass, demyelination
- Pure tone audiometry + speech discrimination — hyperventilation nystagmus warrants schwannoma workup
- Paraneoplastic antibody panel (anti-Yo, anti-Hu, anti-Ri, anti-VGCC) — especially if no structural lesion found
- Autonomic evaluation — orthostatic BP, if MSA-C suspected
- Video Head Impulse Test (vHIT) — to quantify semicircular canal function separately from central findings
- Vestibular rehabilitation — especially Cawthorne-Cooksey and gaze stabilization exercises, after structural cause excluded
Clinical Bottom Line: A K Bhardwaj's VNG demonstrates a triad of central cerebellar oculomotor dysfunction: (1) severe vertical saccade dysmetria from oculomotor vermis failure, (2) asymmetric leftward smooth pursuit loss and gaze-evoked nystagmus from floccular dysfunction, and (3) a catastrophically abnormal 90° SVV deviation with central positional nystagmus from nodulo-uvular (lobules IX–X) pathology. This is not a peripheral vestibular disorder. Urgent MRI of the posterior fossa is the single most important next investigation.
Anything else do you wanna add up from overall reference of neurology and opthalmology
central vestibular syndrome cerebellar oculomotor signs downbeat nystagmus clinical neurology diagnosis
smooth pursuit saccade abnormalities ophthalmology neuro-ophthalmology cerebellar eye movement disorders clinical findings
downbeat nystagmus cerebellar flocculus nodulus eye movement pathway diagram neuro-ophthalmology
peripheral versus central vestibular vertigo nystagmus comparison table clinical features HINTS exam
Extended Neuro-Ophthalmology & Neurology Addendum
A K Bhardwaj | VNG CCDA00341
1. HARD CENTRAL LOCALIZATION — HINTS FRAMEWORK
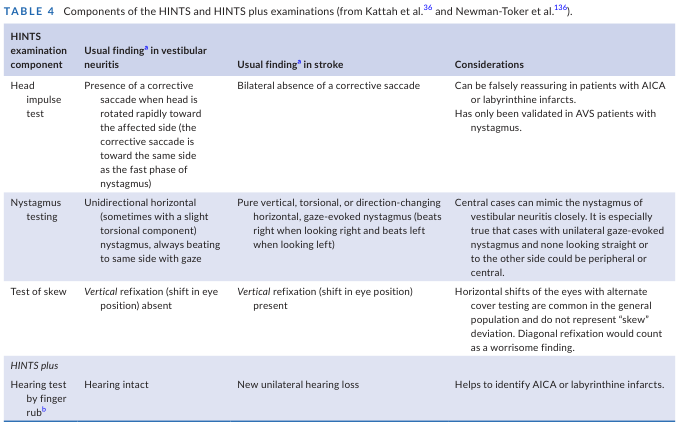
| HINTS Component | Peripheral (Vestibular Neuritis) Pattern | Central (Stroke/Cerebellar) Pattern | This Patient |
|---|---|---|---|
| Head Impulse | Corrective saccade present (ipsilesional) | No corrective saccade | Not formally tested — but HIN present suggesting nerve/central |
| Nystagmus | Unidirectional horizontal, fixed direction | Direction-changing, gaze-evoked, pure vertical/torsional | Multi-directional, gaze-evoked, vertical components → 🔴 Central |
| Test of Skew | Absent vertical refixation | Vertical skew deviation present | SVV 90° deviation strongly implies vertical ocular misalignment → 🔴 Central |
| Hearing (HINTS+) | Intact | New unilateral loss (AICA) | Needs formal audiometry |
2. NEURO-OPHTHALMOLOGY PERSPECTIVE: THE EYE MOVEMENT PATHWAY BREAKDOWN
2A. The Neural Integrator and Gaze-Holding
- The integrator becomes "leaky"
- Eyes drift centripetally (back toward center) from any eccentric position
- The brain generates corrective saccades to reacquire the target
- Result: gaze-evoked nystagmus — exactly what is seen at center (SPV 6.09 °/s) and in left/down gaze in this patient
2B. Saccade Dysmetria — The Cerebellum as a Precision Calibrator
- Hypometric saccades (undershoot, precision <80%) = fastigial nucleus hypofunction
- Vertical worse than horizontal = dorsal vermis involvement
- This patient's vertical precision of 41–46% means the eyes reach only ~43% of the intended target before stopping — requiring multiple corrective catch-up saccades to reach the final position
2C. Asymmetric Smooth Pursuit — Lateralizing the Floccular Lesion
- Left floccular damage → leftward pursuit fails ✅ (patient's gain 0.53–0.55 leftward)
- Right pursuit preserved (gain 0.85–0.91) ✅
3. DOWNBEAT NYSTAGMUS — A FOCAL CEREBELLAR SIGN
- The flocculus normally suppresses the vertical VOR's upward-beating bias
- When the flocculus fails, the eyes drift upward slowly (upward slow phase) with fast downward corrective beats
- This produces downbeat nystagmus — clinically exacerbated when looking down or in the pitch-back position (as seen here)
4. THE SVV CATASTROPHE — OTOLITHIC TILT IN NEUROLOGICAL CONTEXT
| Condition | Typical SVV Deviation |
|---|---|
| Benign utricular dysfunction | 3–8° |
| Vestibular neuritis (acute) | 5–15° |
| Cerebellar infarct (PICA) | 10–20° |
| Nodular cerebellar degeneration | Up to 90° |
| Thalamo-cortical graviceptive lesion | 20–60° |
5. OPTOKINETIC ASYMMETRY — THE PRETECTO-CEREBELLAR LINK
- Nucleus of the optic tract (NOT) and dorsal terminal nucleus (DTN) — in the pretectum
- Inferior olivary nucleus → climbing fibers → cerebellar vermis
- Upward OKN specifically requires an intact upward slow-phase generator in the rostral interstitial nucleus of MLF (riMLF)
6. HYPERVENTILATION-INDUCED NYSTAGMUS — NEUROLOGY ALERT
| Cause | Mechanism |
|---|---|
| Vestibular schwannoma | Hyperventilation reduces CO₂, causes alkalosis, increases ectopic discharge in compressed/demyelinated nerve |
| Demyelinating plaque (MS) | Ephaptic transmission in partially demyelinated fibers, enhanced by alkalosis |
| Vascular compression of CN VIII | Similar ectopic firing mechanism |
| Perilymph fistula | Rare |
7. AGE-RELATED CONTEXT — 67-YEAR-OLD MALE
| Age-related consideration | Relevance |
|---|---|
| Cerebellar microvascular disease | Small vessel disease causing progressive cerebellar atrophy — MRI FLAIR/DWI required |
| Vertebrobasilar TIA or completed infarct | PICA or SCA territory; acute presentation may have been missed |
| Paraneoplastic cerebellar degeneration | More aggressive course; anti-Yo most common in solid tumors |
| Normal pressure hydrocephalus | Gait disturbance + cerebellar signs; MRI ventricular assessment needed |
| Drug toxicity | Phenytoin, carbamazepine, lithium, aminoglycosides — all produce cerebellar OKN/saccade/pursuit abnormalities identical to what is seen |
8. CONSOLIDATED NEUROLOGICAL & OPTHALMOLOGICAL RED FLAGS IN THIS REPORT
| # | Red Flag | Origin | Urgency |
|---|---|---|---|
| 1 | SVV 90° deviation | Nodulus / otolith-CNS pathway | 🔴 Urgent MRI |
| 2 | Vertical saccade precision 41–46% | Oculomotor vermis | 🔴 Central lesion confirmed |
| 3 | Leftward smooth pursuit gain 0.53 | Left flocculus | 🔴 Lateralizing cerebellar sign |
| 4 | Upward OKN gain 0.08 | Pretecto-cerebellar pathway | 🔴 Brainstem involvement possible |
| 5 | Gaze-evoked nystagmus at center | Floccular neural integrator failure | 🔴 Central |
| 6 | Central positional nystagmus (non-fatiguing, multi-directional) | Nodulus/Uvula | 🔴 Not BPPV |
| 7 | Hyperventilation-induced nystagmus | CPA lesion / CN VIII demyelination | ⚠️ MRI with contrast, audiometry |
| 8 | Downbeat components (pitch back, yaw right) | Flocculus/nodulus | 🔴 Classic cerebellar sign |
9. PROPOSED CLINICAL PATHWAY
VNG Findings (Central Pattern Confirmed)
│
├──► MRI Brain + Posterior Fossa (FLAIR, DWI, T1+Gd, CISS sequence)
│ │
│ ├── Structural lesion found → Neurosurgery / Neuro-oncology
│ ├── Infarct found → Stroke unit, antiplatelet/anticoagulation
│ ├── Demyelination found → Neurology / MS workup
│ └── No lesion → Step 2
│
├──► Audiometry + ABR (Auditory Brainstem Response)
│ └── Asymmetric → MRI CPA with contrast (schwannoma)
│
├──► Blood: Paraneoplastic panel (anti-Yo, anti-Hu, anti-VGCC, anti-GAD)
│ └── Positive → Oncology workup (CT chest/abdomen/pelvis)
│
├──► Drug history review (anticonvulsants, lithium, aminoglycosides)
│
└──► Vestibular rehabilitation AFTER structural cause excluded
Summary Statement
Provide me the details of full vestibular nuclei - flocullus nodullus vermis and relation with VNG and other tests.kindly include pictures because I want to learn lesion on the basis of VNG
vestibular nuclei anatomy superior inferior medial lateral Deiters function VOR semicircular canal otolith pathways
flocculus nodulus uvula vermis cerebellar anatomy VOR suppression gaze holding smooth pursuit neural integrator
vestibular nuclei anatomy brainstem superior inferior medial lateral vestibular nucleus diagram
cerebellar vermis lobules flocculonodular lobe oculomotor vermis functional zones diagram sagittal
VNG test abnormal findings lesion localization peripheral central vestibular comparison chart nystagmus
Complete Educational Guide: Vestibular Nuclei · Flocculus · Nodulus · Vermis
With Full VNG Lesion Correlation
PART 1: THE FOUR VESTIBULAR NUCLEI — ANATOMY & FUNCTION
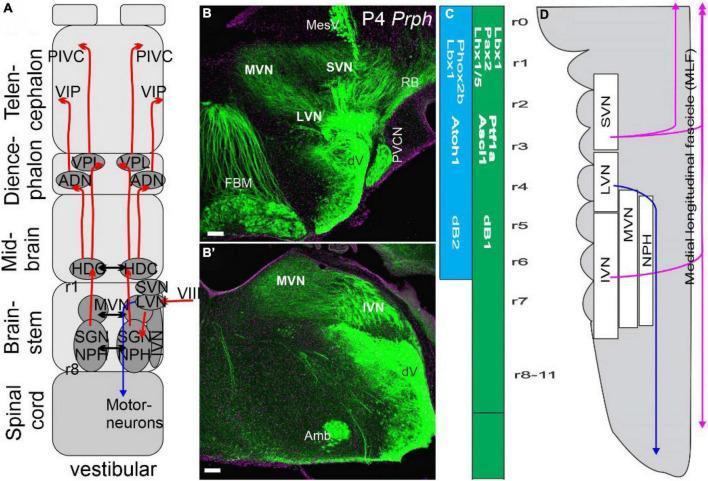
1A. Superior Vestibular Nucleus (SVN) — Bechterew's Nucleus
| Feature | Detail |
|---|---|
| Location | Rostral pons, beneath floor of 4th ventricle |
| Primary Input | Horizontal + anterior semicircular canal afferents (superior vestibular nerve) |
| Primary Output | MLF → ipsilateral CN VI, contralateral CN III → horizontal VOR |
| Key Function | Coordinates the horizontal vestibulo-ocular reflex (hVOR) during head rotation |
| Cerebellar Connection | Receives inhibitory Purkinje cell output from flocculus |
- Reduced or absent compensatory eye movement during horizontal head impulse (vHIT)
- Ipsilateral corrective saccade visible in vHIT
- Reduced caloric response on the affected side
- Smooth pursuit impaired ipsilaterally (loss of floccular input to SVN)
1B. Lateral Vestibular Nucleus (LVN) — Deiters' Nucleus
| Feature | Detail |
|---|---|
| Location | Lateral pons/medulla junction |
| Primary Input | Utricular otolith afferents, spinal cord (spinovestibular), cerebellar cortex |
| Primary Output | Lateral vestibulospinal tract (LVST) → ipsilateral limb extensors (anti-gravity) |
| Key Function | Postural control, limb extension tone, balance during linear acceleration |
| Cerebellar Connection | Receives input from vermis (anterior lobe, lobule I–V) and fastigial nucleus |
- Ipsilateral falling/tilting tendency — clinically dominant
- Skew deviation (hypertropia contralateral to lesion)
- SVV tilt toward the lesion side (2–15°)
- Minimal nystagmus unless large lesion extending to MVN
1C. Medial Vestibular Nucleus (MVN) — Schwalbe's Nucleus
| Feature | Detail |
|---|---|
| Location | Medial floor of 4th ventricle, pons–medulla junction |
| Primary Input | ALL three semicircular canals; commissural fibers from contralateral MVN |
| Primary Output | MLF (ascending + descending) → Medial vestibulospinal tract (MVST) → neck muscles |
| Key Function | Velocity storage integrator — prolongs VOR duration; cervico-ocular reflexes; commissural inhibition maintaining tonic balance |
| Cerebellar Connection | Direct inhibitory input from nodulus and uvula (critical!) |
- Spontaneous nystagmus — horizontal, direction fixed, fast phase away from lesion
- Direction-changing positional nystagmus (if velocity storage disrupted)
- Extended time constant of post-rotatory nystagmus
- Failure of nystagmus suppression by fixation (if nodular inhibition to MVN lost)
- Abnormal caloric asymmetry
The MVN is the most important nucleus for understanding most VNG abnormalities — it is the gateway through which cerebellar structures (nodulus, uvula) modulate nystagmus duration and spatial orientation.
1D. Inferior Vestibular Nucleus (IVN) — Descending / Spinal Nucleus
| Feature | Detail |
|---|---|
| Location | Medulla, caudal to MVN |
| Primary Input | Saccular otolith afferents (inferior vestibular nerve); posterior canal afferents |
| Primary Output | MVST, reticular formation, cerebellum (nodulus) |
| Key Function | Vertical VOR components; saccular (gravity/linear) processing; transmits to nodulus |
| Cerebellar Connection | Bidirectional with nodulus and uvula |
- Vertical positional nystagmus (often downbeat in character)
- Disrupted saccular VEMP responses (absent cVEMP)
- Abnormal otolith-ocular reflexes
PART 2: THE CEREBELLUM — VESTIBULOCEREBELLAR STRUCTURES
Cerebellar Lobule Map
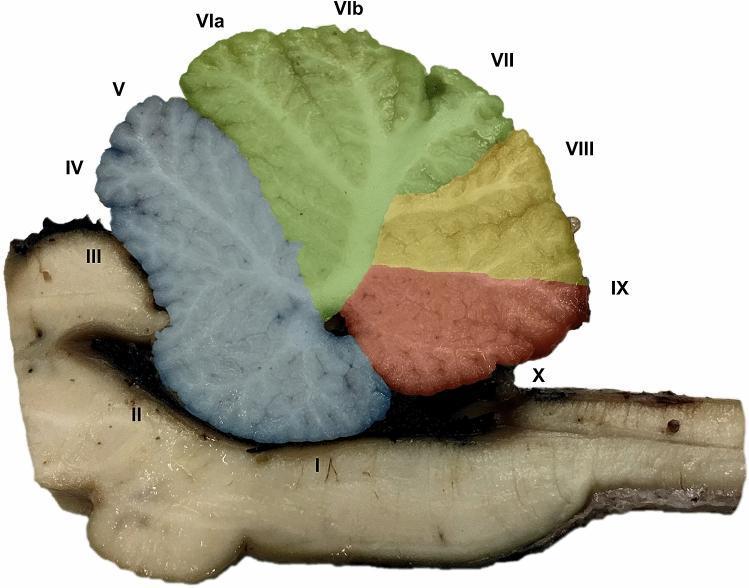
2A. FLOCCULUS & PARAFLOCCULUS (Lobule X — lateral extensions)
Anatomy
- Receives visual motion signals from the accessory optic system and nucleus of optic tract (NOT)
- Receives efference copy of eye motor commands from DLPN (dorsolateral pontine nucleus)
- Receives vestibular signals directly from the SVN and MVN
- Purkinje cell output → inhibits MVN and NPH (nucleus prepositus hypoglossi)
Functions — One Structure, Five Critical Jobs
| Function | Mechanism | If Damaged |
|---|---|---|
| 1. Smooth pursuit maintenance | Flocculus drives the velocity signal to sustain smooth tracking | Ipsilateral pursuit gain drops (gain <0.5 = flocc. lesion) |
| 2. Neural integrator stabilization | Flocculus "charges" the NPH/MVN neural integrator to hold eccentric gaze | Gaze-evoked nystagmus (leaky integrator) |
| 3. VOR gain calibration | Adjusts VOR gain 1.0 so image stays still during head movement | VOR gain error (tested by vHIT / caloric) |
| 4. VOR suppression (fixation) | Suppresses VOR when you track a head-fixed target | Loss of VOR suppression (fixation fails to cancel VOR) |
| 5. Downward VOR bias suppression | Prevents upward drift of eyes by inhibiting downward slow-phase pathway | Downbeat nystagmus (upward drift + downward fast phase) |
VNG Pattern: Isolated Floccular Lesion
VNG TEST FINDING MECHANISM
─────────────────────────────────────────────────────────────────
Smooth Pursuit Ipsilateral gain severely low No floccular drive
Gaze Test GEN at primary gaze Leaky neural integrator
OKN Reduced ipsilateral Same pursuit pathway
Spontaneous Nys. Absent OR mild downbeat Downward bias released
Head Shake Nys. Absent or minimal Peripheral canal intact
Positional Mild, non-specific
SVV Normal or mild tilt (<5°) Otolith pathway intact
Caloric Normal (peripheral VOR intact)
2B. NODULUS (Lobule X — midline) + UVULA (Lobule IX — midline)
Anatomy
- Receives direct primary vestibular afferents (the only cerebellar structure to do so)
- Input from ALL semicircular canals + otolith organs via the inferior vestibular nerve
- Purkinje cell output → directly inhibits the MVN and IVN (velocity storage mechanism)
- Projects to the fastigial nucleus for postural integration
Functions
| Function | Mechanism | If Damaged |
|---|---|---|
| 1. Velocity storage regulation | Nodulus inhibits MVN, shortening the time constant of VOR decay | Prolonged velocity storage → direction-changing nystagmus |
| 2. Canal-plane specific VOR suppression | Specifically suppresses low-frequency, gravity-dependent VOR | Positional nystagmus that doesn't fatigue |
| 3. Spatial orientation (head in space) | Integrates canal + otolith signals to compute 3D head orientation | SVV gross deviation |
| 4. Periodic alternating nystagmus suppression | Nodulus prevents the nystagmus from cycling direction every 2 min | Periodic alternating nystagmus (PAN) if damaged |
| 5. Otolith-canal conflict resolution | Resolves the ambiguity between canal and otolith signals during sustained rotation | Post-rotatory nystagmus in wrong plane |
VNG Pattern: Nodulus/Uvula Lesion — THE CENTRAL POSITIONAL NYSTAGMUS GENERATOR
VNG TEST FINDING MECHANISM
──────────────────────────────────────────────────────────────────────
Positional (DH) Non-fatiguing nystagmus Velocity storage unregulated
Any direction (up/down/horiz) Canal selectivity lost
Persists in multiple positions Cannot suppress gravity-VOR
Direction may change Alternating velocity storage
Spontaneous Nys. Absent in primary gaze Resting tone balanced
Head Shake Absent or minimal Canal function intact
SVV GROSSLY ABNORMAL (30–90°) Spatial orientation lost
OKN vertical Severely reduced Vertical orienting lost
Caloric Normal (peripheral intact)
Gaze Test Normal or mild nystagmus Flocculus separate
Key Teaching Point: The hallmark that separates nodular lesion from BPPV is:
- BPPV → fatigable, latency 5–10 sec, upbeat-torsional, <60 sec, one position
- Nodular lesion → non-fatiguing, immediate, multi-directional, multi-positional, persistent
2C. OCULOMOTOR VERMIS (Lobules VI–VII) + FASTIGIAL OCULOMOTOR REGION (FOR)
Anatomy
- Receives visual feedback from the superior colliculus and visual cortex via pontine nuclei
- Receives efference copy of every saccade command
- Purkinje cell output → inhibits the fastigial nucleus (FOR)
- FOR output → PPRF (paramedian pontine reticular formation) and riMLF for horizontal and vertical saccade burst neurons
Functions
| Function | Mechanism | If Damaged |
|---|---|---|
| Saccade accuracy calibration | Compares intended vs. actual displacement, modifies gain | Hypometric saccades (undershoot, low precision) |
| Catch-up saccade control | Generates corrective secondary saccades after undershoot | Multiple corrective saccades per movement |
| Vertical saccade calibration | Specifically calibrates vertical amplitude via dorsal vermis | Vertical worse than horizontal dysmetria |
| Saccade velocity tuning | Sets appropriate peak velocity for given amplitude (main sequence) | Main sequence abnormalities |
VNG Pattern: Oculomotor Vermis/FOR Lesion
VNG TEST FINDING MECHANISM
──────────────────────────────────────────────────────────────────
Saccade Test Precision severely reduced Calibration circuit broken
Vertical worse than horizontal Dorsal vermis dominant
Low peak velocity (vertical) Burst neuron drive reduced
Prolonged latency Initiation delay
Multiple corrective saccades Secondary saccade generation
Smooth Pursuit Mildly reduced (saccadic pursuit) Catch-up saccades intrude
Gaze Test Mild nystagmus (GEN) Secondary floccular effect
OKN Saccadic phase disrupted Fast phase (saccade) impaired
Positional Usually normal Not involved in VOR
SVV Usually normal or mild Not involved in otolith
Caloric Normal Peripheral intact
PART 3: COMPLETE VNG-TO-LESION MAPPING MASTER TABLE
| VNG Finding | Normal Value | Abnormal Value | Peripheral Lesion | Central Lesion Site |
|---|---|---|---|---|
| Saccade Precision (horiz.) | >80% | <70% | Rare | Oculomotor vermis / FOR |
| Saccade Precision (vert.) | >80% | <60% | Not applicable | Oculomotor vermis (VI–VII) — most specific |
| Saccade Velocity (vert.) | >200 °/s | <180 °/s | Not applicable | Dorsal vermis / riMLF |
| Saccade Latency | 150–250 ms | >260 ms | Peripheral nerve (mild) | Frontal eye fields / vermis |
| Smooth Pursuit Gain (horiz.) | 0.8–1.0 | <0.7 (asymmetric) | Rare, bilateral = aging | Flocculus (ipsilateral to low gain) |
| Smooth Pursuit Gain (vert.) | 0.8–1.0 | <0.7 | Not applicable | Dorsal vermis / pretectum |
| OKN Horiz. (symmetric) | 0.8–1.1 | <0.7 or asymmetric | Peripheral (mild asymm.) | Cerebral hemisphere (visual cortex) |
| OKN Vertical upward | 0.8–1.1 | <0.5 | Not applicable | Pretectum + dorsal vermis |
| OKN Vertical downward | 0.8–1.1 | <0.7 | Not applicable | Brainstem / pretectum |
| Spontaneous Nystagmus (light) | Absent | Present, unidirectional | SVN/MVN peripheral lesion — labyrinth, CN VIII | If direction-changing or vertical = central |
| Spontaneous Nystagmus (dark) | Absent | Present | MVN/SVN — increases without fixation | Central: does NOT increase in dark |
| Head Shake Nystagmus | Absent | Present, horizontal | Peripheral — canal asymmetry | Vertical HSN = central (brainstem) |
| Hyperventilation Nystagmus | Absent | Present | CN VIII compression / schwannoma | Demyelinating plaque CPA region |
| Gaze-Evoked Nystagmus (GEN) | Absent | SPV >3 °/s eccentric | Rare (muscle paresis) | Flocculus / paraflocculus / brainstem |
| Positional Nystagmus — fatigable, latency, upbeat-torsional | Absent | Upbeat-torsional | Posterior canal BPPV (canalith) | — |
| Positional Nystagmus — non-fatiguing, multi-directional | Absent | Any direction, persistent | Not peripheral | Nodulus / Uvula (IX–X) |
| Positional Nystagmus — horizontal, direction changes with head | Absent | Changes direction | Horizontal canal BPPV (cupulolithiasis) | If no fatigue → nodular |
| SVV Deviation | ≤2–3° | 3–10° = peripheral; >10° = central | Utricular damage | LVN / nodulus / thalamus |
| SVV Deviation | ≤2–3° | >30° | Not possible peripherally | Nodulus (lobule X) dominant |
| Caloric — Unilateral Weakness | <20% asymmetry | >25% UW | Peripheral (labyrinth / CN VIII) | If UW + other central signs = CPA |
| Caloric — Directional Preponderance | <20% | >25% DP | Mild: compensated peripheral | Brainstem, if large DP |
| vHIT — Corrective Saccade | Absent | Covert/overt saccade | Peripheral — specific canal | Absent saccade with symptoms = central HINTS |
PART 4: THE VESTIBULO-OCULAR REFLEX (VOR) ARC — HOW IT CONNECTS EVERYTHING
HEAD ROTATION
│
▼
SEMICIRCULAR CANALS (peripheral sensor)
│ (CN VIII — superior/inferior divisions)
▼
VESTIBULAR NUCLEI (SVN + MVN — central relay)
│ ▲
│ INHIBITION from
│ FLOCCULUS (Purkinje cells)
│ NODULUS → MVN
▼
MEDIAL LONGITUDINAL FASCICULUS (MLF)
│
├──► CN VI nucleus (PPRF) → Lateral Rectus (ipsilateral)
│
└──► CN III nucleus → Medial Rectus (contralateral)
RESULT: Eyes move OPPOSITE to head → image stabilized on retina
| VNG Test | What It Interrogates | Structure |
|---|---|---|
| Caloric test | Low-frequency hVOR integrity | SVN ↔ CN VI via MLF |
| vHIT | High-frequency hVOR (canal-specific) | Each canal → SVN |
| Spontaneous nystagmus | Resting tonic balance between the two sides | MVN bilateral balance |
| Head shake nystagmus | Asymmetry stored in velocity storage | MVN velocity storage |
| Smooth pursuit | Slow eye velocity tracking system | Flocculus → SVN/MVN |
| Saccades | Rapid gaze shift accuracy | Vermis → FOR → PPRF |
| Gaze test | Neural integrator charge capacity | Flocculus → NPH/MVN |
| Positional testing | Otolith-canal conflict resolution | Nodulus → MVN |
| SVV | Internal gravity estimate | Nodulus → LVN → INC |
| OKN | Full-field visual velocity processing | Pretectum → vermis → MVN |
PART 5: LESION-BY-LESION CLINICAL SYNDROMES WITH VNG FINGERPRINTS
SYNDROME 1: Isolated Vestibular Neuritis (SVN + MVN peripheral)
- Spontaneous horizontal nystagmus, fast phase AWAY from lesion ✅
- Increases in darkness, suppressed by fixation ✅
- Unilateral caloric weakness >25% ✅
- Normal saccades, normal pursuit ✅
- Normal SVV (or mild <10° toward lesion) ✅
- No gaze-evoked nystagmus ✅
- Head shake nystagmus horizontal toward healthy side ✅
SYNDROME 2: BPPV — Posterior Canal (Canalith in posterior SCC)
- Dix-Hallpike: upbeat-torsional nystagmus, latency 5–10 sec, duration <60 sec ✅
- Fatigues with repeated testing ✅
- Returns on sitting up (reverses direction) ✅
- All other tests: completely normal ✅
- SVV normal ✅
SYNDROME 3: Floccular Lesion (e.g., early cerebellar degeneration, SCA)
- Smooth pursuit gain low, asymmetric (worse ipsilateral) 🔴
- Gaze-evoked nystagmus at primary + eccentric gaze 🔴
- VOR suppression failure (fixation cannot suppress caloric nystagmus) 🔴
- Normal spontaneous nystagmus (in early stages) ✅
- Normal positional testing ✅
- SVV normal or mildly abnormal ✅
- Saccades mildly affected (secondary) ⚠️
SYNDROME 4: Nodular/Uvular Lesion (e.g., posterior fossa tumor, infarct, degeneration)
- Multi-positional non-fatiguing nystagmus 🔴
- Direction may change between positions 🔴
- No latency in Dix-Hallpike 🔴
- SVV grossly abnormal (>20°, up to 90°) 🔴
- Normal spontaneous nystagmus (unless large lesion) ✅
- Normal caloric (peripheral intact) ✅
- Normal saccades (unless co-involvement of vermis) ✅
- OKN vertical severely reduced 🔴
SYNDROME 5: Oculomotor Vermis / FOR Lesion (cerebellar degeneration, SCA, alcohol)
- Saccade precision severely reduced (especially vertical) 🔴
- Vertical saccade velocity reduced 🔴
- Latency prolonged 🔴
- Smooth pursuit: intrusion of catch-up saccades ("cogwheel/saccadic pursuit") ⚠️
- Normal spontaneous nystagmus ✅
- Normal caloric ✅
- Normal SVV ✅
SYNDROME 6: MLF Lesion — Internuclear Ophthalmoplegia (INO)
- Adduction lag or paresis ipsilateral to lesion 🔴
- Monocular horizontal nystagmus in abducting eye 🔴
- Dissociated saccade velocities — adducting eye slower 🔴
- Vertical saccades and pursuit preserved ✅
- Convergence may be spared (midbrain INO) ✅
- Bilateral INO = MS until proven otherwise
SYNDROME 7: Wallenberg Syndrome (PICA infarct — lateral medullary)
- Spontaneous nystagmus, direction toward lesion (ipsipulsion) 🔴
- Ocular tilt reaction: head tilt + skew + SVV tilt (all toward lesion) 🔴
- Contrapulsion of saccades — saccades overshoot contralaterally, undershoot ipsilaterally 🔴
- Ipsilateral pursuit failure 🔴
- OKN asymmetry 🔴
- Involves: MVN, IVN, inferior cerebellar peduncle, nucleus ambiguus, spinothalamic tract
SYNDROME 8: CPA Lesion (Vestibular Schwannoma / Meningioma)
- Hyperventilation-induced nystagmus (pathognomonic) 🔴
- Caloric unilateral weakness >30% 🔴
- Spontaneous nystagmus may be absent (chronic compensation) ✅
- vHIT: reduced VOR gain in specific canal 🔴
- Audiometry: unilateral sensorineural hearing loss, poor speech discrimination 🔴
- Normal positional, normal saccades, normal SVV (unless brainstem compression) ✅
PART 6: APPLYING THIS TO A K BHARDWAJ — THE COMPLETE LESION MAP
┌─────────────────────────────────────────────────────────────────┐
│ A K BHARDWAJ — LESION LOCALIZATION MAP │
├──────────────────────┬──────────────────────┬───────────────────┤
│ STRUCTURE │ VNG EVIDENCE │ SEVERITY │
├──────────────────────┼──────────────────────┼───────────────────┤
│ LEFT FLOCCULUS │ Leftward pursuit 0.53 │ 🔴 SEVERE │
│ │ GEN at primary gaze │ │
│ │ Downbeat components │ │
├──────────────────────┼──────────────────────┼───────────────────┤
│ NODULUS (X) + │ Non-fatiguing multi- │ 🔴 SEVERE │
│ UVULA (IX) │ positional nystagmus │ │
│ │ SVV 90° deviation │ │
│ │ Vertical OKN ~0.08 │ │
├──────────────────────┼──────────────────────┼───────────────────┤
│ OCULOMOTOR VERMIS │ Vertical saccade │ 🔴 SEVERE │
│ (VI–VII) + FOR │ precision 41–46% │ │
│ │ Vertical velocity low │ │
│ │ Prolonged latency │ │
├──────────────────────┼──────────────────────┼───────────────────┤
│ MVN (secondary) │ Velocity storage │ ⚠️ MODERATE │
│ │ not suppressed by │ │
│ │ nodulus → persistent │ │
│ │ positional nystagmus │ │
├──────────────────────┼──────────────────────┼───────────────────┤
│ LEFT CPA / CN VIII │ Hyperventilation │ ⚠️ POSSIBLE │
│ (possible) │ nystagmus right eye │ Needs MRI │
│ │ only │ │
├──────────────────────┼──────────────────────┼───────────────────┤
│ PERIPHERAL VESTIBULAR│ Spontaneous nys. │ ✅ INTACT │
│ SYSTEM │ absent; head-shake │ │
│ (labyrinth + CN VIII │ absent; bilateral │ │
│ gross function) │ caloric presumably │ │
│ │ symmetric │ │
└──────────────────────┴──────────────────────┴───────────────────┘
QUICK REFERENCE: THE ONE-PAGE VNG CHEAT SHEET
| If you see this on VNG... | Think this structure | Confirm with... |
|---|---|---|
| Low smooth pursuit gain, asymmetric | Flocculus (ipsilateral) | MRI posterior fossa |
| Gaze-evoked nystagmus at center | Flocculus (neural integrator) | MRI, vHIT |
| Non-fatiguing positional nystagmus | Nodulus + Uvula | MRI, caloric |
| SVV >10° | LVN or Nodulus or Thalamus | MRI + VEMP |
| SVV >30° | Nodulus almost certainly | MRI urgent |
| Vertical saccade dysmetria | Oculomotor vermis (VI–VII) | MRI vermis |
| Upward OKN absent | Pretectum + dorsal vermis | MRI midbrain |
| Downbeat nystagmus | Flocculus + Nodulus | MRI urgent |
| Hyperventilation nystagmus | CPA lesion / schwannoma | MRI with contrast + ABR |
| Unidirectional horizontal spontaneous nystagmus | MVN/SVN (peripheral) | Caloric, vHIT |
| Direction-changing spontaneous nystagmus | MVN (central) | MRI brainstem |
| Caloric UW >25%, all else normal | Peripheral (labyrinth/CN VIII) | Audiometry, MRI |
| Dissociated saccade velocity (adduction slow) | MLF (INO) | MRI brainstem (MS?) |
| Saccade ipsipulsion + SVV + skew | Lateral medullary (PICA) | MRI DWI urgent |
If you want me to teach the interesting cases of vestibular, m an audio- vestibular specialist I do VNG ECOCGH LLR MLR VEMP VHIT and vestibular screening so pls provide the recent diagnosis what we miss out in general history taking I am from India
missed diagnosis vestibular disorders clinical history taking superior canal dehiscence vestibular migraine PPPD chronic subjective dizziness
ECoG electrocochleography VEMP vHIT caloric combination diagnosis Meniere's disease endolymphatic hydrops vestibular neuritis differential
vestibular disorders differential diagnosis algorithm clinical history dizziness vertigo classification
PPPD persistent postural perceptual dizziness diagnosis criteria missed functional vestibular disorder anxiety
superior semicircular canal dehiscence Tullio phenomenon Hennebert autophony diagnosis vHIT VEMP CT temporal bone
Meniere disease endolymphatic hydrops ECoG SP AP ratio diagnosis MRI gadolinium inner ear
Missed & Underdiagnosed Vestibular Conditions
A Specialist Guide for the Audio-Vestibular Clinician (India)
Tests: VNG · ECoG · LLR · MLR · VEMP · vHIT · Vestibular Screening
OPENING: WHY WE MISS DIAGNOSES — THE ROOT CAUSE
| Common Error | What Actually Happens |
|---|---|
| Symptom anchoring | Patient says "giddiness" → you jump to BPPV without exploring further |
| Incomplete temporal history | Not asking exactly how long each episode lasts (seconds vs minutes vs hours is everything) |
| Missing the "second diagnosis" | BPPV resolved but patient still dizzy → PPPD ignored |
| Not asking about sound triggers | Missing SCD, Perilymph fistula, Tullio phenomenon |
| Not asking about head position vs head movement | Orthostatic vs BPPV vs CSD distinction |
| Skipping autonomic history | POTS, orthostatic hypotension masquerading as vestibular |
| No migraine probe | 40% of vestibular migraine patients never report headache with their dizziness |
| Ignoring bilateral findings | Bilateral vestibular hypofunction (BVH) — the most underdiagnosed condition in India |
DIFFERENTIAL FRAMEWORK: THE TIMING RULE — THE SINGLE MOST IMPORTANT HISTORY TOOL
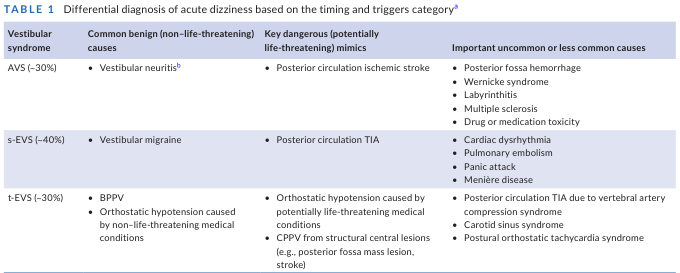
SECONDS (5–60 sec) → BPPV (position-triggered)
→ Orthostatic hypotension (position-change triggered)
→ Superior Canal Dehiscence (sound/pressure triggered)
→ Vertebral artery compression syndrome
MINUTES (5–20 min) → Posterior circulation TIA ⚠️ DANGEROUS
→ Vestibular migraine
→ Panic attack / hyperventilation
HOURS (20 min–24 h) → Ménière's disease (20 min–12 h)
→ Vestibular migraine (5 min–72 h)
→ Autoimmune inner ear disease
DAYS–WEEKS (constant) → Vestibular neuritis (acute)
→ PPPD (chronic)
→ Bilateral vestibular hypofunction
→ Central vestibular (cerebellar/brainstem)
THE 12 MOST MISSED DIAGNOSES — WITH FULL TEST BATTERY CORRELATION
1. PERSISTENT POSTURAL PERCEPTUAL DIZZINESS (PPPD)
The Most Commonly Missed Diagnosis in Your Clinic
- Patients present with chronic "imbalance" and "heaviness in head" for months to years
- Many have had a genuine vestibular event (BPPV, neuritis) 6–12 months ago that resolved — but dizziness persists
- Labelled as "anxiety," "spondylosis," or "cervicogenic" and sent for MRI/X-ray which are normal
- Psychiatry refer back to ENT, ENT refers back to psychiatry — patient lost in the system
| Question to Ask | PPPD Answer |
|---|---|
| "When is dizziness worst?" | Upright (standing/walking), NOT lying down |
| "What makes it worse?" | Busy visual environments (markets, malls, scrolling phone, traffic) |
| "What makes it better?" | Lying still, closing eyes, quiet room |
| "Does head movement cause it?" | Yes — but persists AFTER the movement stops |
| "Do you feel anxious when dizzy?" | Yes — but anxiety FOLLOWS dizziness, doesn't precede it |
| "Did you have a vestibular episode before this started?" | Almost always YES |
| "Any panic attacks in public?" | Common (agoraphobia-like behavior) |
- Prior BPPV, vestibular neuritis, Ménière's attack
- Concussion / head injury
- Prior central vestibular event
- Cardiac event, major surgery, panic attack
- In India specifically: Road accident whiplash, prolonged bed rest
| Test | Expected Finding | What It Tells You |
|---|---|---|
| VNG spontaneous | Normal | No active peripheral lesion |
| VNG smooth pursuit | Normal or mildly reduced | Central adaptation, not structural |
| VNG positional | Normal | Confirms not BPPV |
| vHIT | Normal (or shows old compensated deficit) | Canal function intact or compensated |
| Caloric | Normal or mild old asymmetry | Confirms compensation occurred |
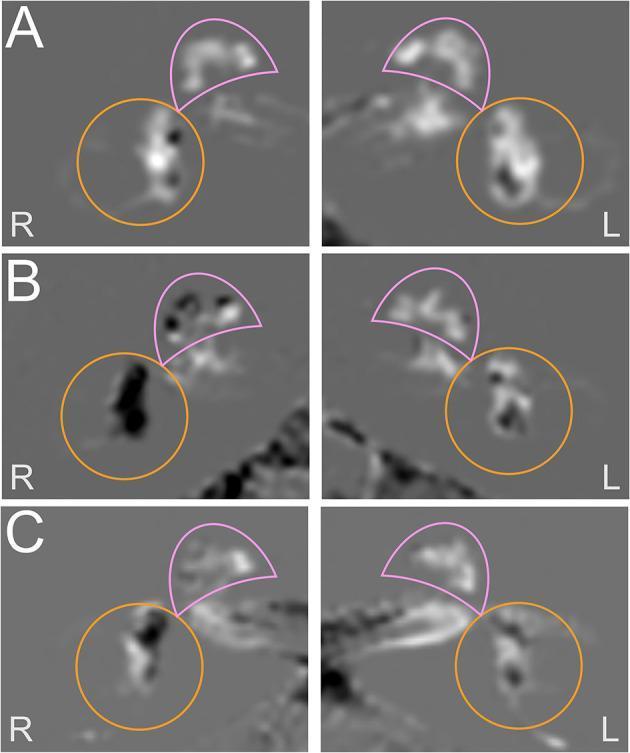
| VEMP (cVEMP + oVEMP) | Normal | Otolith intact |
| ECoG | Normal | No hydrops |
| Posturography (if available) | Pattern 5 or 6 (visual dependence) | The hallmark finding |
The PPPD Diagnosis is CLINICAL using Bárány Society criteria (2017):
- Dizziness/unsteadiness ≥3 months, present on most days
- Worsened by upright posture, active/passive motion, moving visual stimuli
- Triggered by a precipitating event
- No active structural lesion to explain it
2. VESTIBULAR MIGRAINE (VM)
The Great Impersonator
- 40% of VM patients have NO headache at the time of vestibular attack
- Diagnosed as "BPPV" (positional dizziness component), "Ménière's" (fullness + hearing symptoms possible), or "anxiety"
- In India: heavily attributed to cervical spondylosis and treated with traction, which helps nothing
| Question | VM Clue |
|---|---|
| "Do you get headaches at any point in your life?" | Migraine history — may be childhood only |
| "Do you have motion sickness since childhood?" | Very strong predictor of VM |
| "Is bright light or noise unbearable during dizziness?" | Photophobia/phonophobia WITHOUT headache |
| "Does your dizziness correlate with periods/menstrual cycle?" | Hormonal trigger — huge in Indian women |
| "Do you get visual aura — zigzag lines, spots?" | Migraine equivalent |
| "Family history of migraine?" | Strong genetic component |
| "Any food triggers — chocolate, cheese, red wine, MSG?" | Dietary triggers |
| "Does dizziness occur premenstrually?" | Estrogen withdrawal trigger |
| "How long does the vestibular attack last?" | 5 min to 72 hours (enormous range) |
| Test | Finding | Significance |
|---|---|---|
| VNG spontaneous | Usually normal (interictal) | Not diagnostic alone |
| VNG smooth pursuit | Mildly reduced, bilateral | Cerebellar hypoperfusion |
| VNG saccades | Mild precision reduction | Non-localizing |
| Positional testing | May show central positional nystagmus | Nodular/central hypoperfusion |
| Gaze test | Mild GEN | Non-specific |
| vHIT | Normal (canal VOR intact) | KEY differentiator from neuritis |
| VEMP (cVEMP) | Reduced amplitude or absent | Saccular involvement in VM |
| VEMP (oVEMP) | Asymmetric | Utricular involvement |
| ECoG | Normal SP/AP ratio | Differentiates from Ménière's |
| Caloric | Normal or mild asymmetry | Rarely >25% UW |
| Feature | Vestibular Migraine | Ménière's Disease |
|---|---|---|
| Hearing loss | Absent or fluctuating | Progressive, low-frequency |
| Tinnitus | Absent or non-specific | Low-pitched roaring, fluctuating |
| Aural fullness | Mild/variable | Prominent, ipsilateral |
| Attack duration | 5 min–72 hours | 20 min–12 hours |
| ECoG SP/AP ratio | Normal (<0.4) | Elevated (>0.4–0.5) |
| MRI gadolinium (HYDROPS-Mi2) | Grade 0 (normal) | Grade 1–2 hydrops |
| VEMP threshold | Normal | Lowered (saccular hydrops) |
| Migraine history | Essential | Incidental |
| Prophylaxis response | Propranolol, topiramate | Betahistine, diuretics |
3. SUPERIOR SEMICIRCULAR CANAL DEHISCENCE (SCD / SSCD)
The Diagnosis Hidden in Plain History
- Extremely rare awareness among general ENT and audiology
- Patients present to multiple specialists over years with "autophony," "giddiness on exertion," "hearing my own heartbeat"
- Misdiagnosed as: patulous Eustachian tube, otosclerosis, BPPV, anxiety
- CT temporal bone not ordered with the right protocol (needs 0.5mm cuts)
| Symptom | Description | Mechanism |
|---|---|---|
| Tullio phenomenon | Dizziness/nystagmus triggered by loud sounds | Sound energy drives dehiscent canal directly |
| Hennebert sign | Dizziness with positive/negative pressure (nose blowing, Valsalva, sneezing) | Pressure transmitted through 3rd window |
| Autophony | Hearing own voice/footsteps loudly in affected ear | Sound conducted via bone through dehiscence |
| Pulsatile tinnitus | Hearing heartbeat/pulse in ear | Vascular pulsations transmitted via dehiscence |
| Tullio on exercise | Dizziness when running, heavy lifting, straining at stool | Increased intracranial pressure transmitted |
In India specifically ask: "Do you feel dizzy when you blow your nose? When you shout? When you hear the temple bells or loud music?"
| Test | SCD Finding | Mechanism |
|---|---|---|
| vHIT | Normal (all 6 canals) | The superior canal still functions via 3rd window |
| cVEMP | LOWERED threshold (<75 dB) + Enhanced amplitude | 3rd window increases acoustic sensitivity of saccule |
| oVEMP | Enhanced amplitude, present at low levels | Utricle also affected by 3rd window |
| Caloric | Normal | Horizontal canal intact |
| VNG positional | Usually normal | |
| Pure tone audiometry | Low-frequency conductive loss with normal tympanogram + present acoustic reflexes = AIR-BONE GAP WITHOUT MIDDLE EAR PATHOLOGY | Pathognomonic combination |
| CT temporal bone (0.5mm) | Dehiscence of superior canal roof (arcuate eminence) | Confirms diagnosis |
| VNG spontaneous | May show superior canal nystagmus with Valsalva | Pressure-induced |
The VEMP finding in SCD is the most sensitive non-invasive test: cVEMP threshold <75 dBHL + elevated amplitude = screen positive. CT confirms.
4. BILATERAL VESTIBULAR HYPOFUNCTION (BVH)
The Most Underdiagnosed Condition in Indian Audiology
- No acute vertigo — so patients never come urgently
- Chief complaint: "imbalance in the dark," "oscillopsia when walking," "can't read sign boards in moving vehicle"
- Attributed to: "old age," "cervical spondylosis," "blood pressure," "weakness"
- vHIT and bilateral caloric — rarely done together in India
| Critical Question | BVH Answer |
|---|---|
| "Do you feel more unsteady at night or in dim light?" | YES — removes visual compensation |
| "Do you fall in the bathroom when closing your eyes to wash face?" | YES — Romberg in real life |
| "When walking in a crowd, do you feel others are bumping you?" | YES — spatial disorientation |
| "Can you read a sign board clearly while walking or in a moving vehicle?" | NO — oscillopsia — pathognomonic |
| "Do you feel unsteady on uneven ground, grass, sand?" | YES |
| "Any history of gentamicin injection, streptomycin? (TB treatment in India)** | CRITICAL in India — aminoglycoside toxicity is #1 cause |
| "History of meningitis?" | Bilateral labyrinthine damage |
| "Any autoimmune disease — lupus, RA, Wegener's?" | Autoimmune BVH |
| "Long-term quinine use for malaria?" | Ototoxicity in India |
| "Chemotherapy — cisplatin?" | Major cause of BVH |
In India, the most common cause of BVH is AMINOGLYCOSIDE OTOTOXICITY — particularly intratympanic gentamicin (over-used for Ménière's) and systemic streptomycin/gentamicin for TB. Ask every single BVH patient about TB treatment history.
| Test | BVH Finding | Significance |
|---|---|---|
| vHIT bilateral | Reduced VOR gain all 6 canals + covert + overt saccades | Pathognomonic |
| Caloric (bilateral) | <10 °/s slow phase velocity BILATERALLY = bilateral weakness | Confirms BVH |
| VNG spontaneous | Normal (no tonic asymmetry — equal loss both sides) | No nystagmus = bilateral |
| VNG gaze test | GEN bilateral (compensatory) | Neural integrator failing |
| Smooth pursuit | Impaired | Secondary central effect |
| cVEMP bilateral | Reduced/absent bilaterally | Saccular involvement |
| oVEMP bilateral | Reduced/absent bilaterally | Utricular involvement |
| Pure tone audiometry | Normal to severe SNHL | Depends on cause |
| ECoG | Normal SP/AP | No hydrops |
5. THIRD WINDOW SYNDROMES (Beyond SCD)
Enlarged Vestibular Aqueduct, Dehiscent Jugular Bulb, Semicircular Canal Fistula
| History Clue | |
|---|---|
| "Did hearing drop suddenly after a knock on the head/minor trauma?" | Hallmark |
| "Child with fluctuating SNHL since birth?" | EVA in children |
| "Dizziness with Valsalva?" | 3rd window effect |
- cVEMP: lowered threshold (same as SCD)
- CT temporal bone: vestibular aqueduct >1.5mm at midpoint (Cincinnati criteria)
- MRI: dilated endolymphatic sac
- Audiometry: bilateral SNHL, low-frequency predominantly
6. AUTOIMMUNE INNER EAR DISEASE (AIED)
Missed Because No One Asks About Systemic Autoimmune History
- "Any joint pains, dry eyes, mouth ulcers, skin rashes?"
- "Any previous episode in the OTHER ear?"
- "Hearing loss progressing over weeks to months?"
- "Family history of autoimmune disease?"
- India-specific: Tuberculosis → immune complex deposition can affect inner ear
| Test | AIED Finding |
|---|---|
| Audiometry | Bilateral, rapidly progressive SNHL over weeks–months |
| ECoG | May show elevated SP/AP (endolymphatic hydrops secondary to AIED) |
| cVEMP/oVEMP | Reduced/absent bilaterally |
| vHIT | Progressive bilateral gain reduction |
| Blood: ANA, anti-dsDNA, ESR, CRP, complement, anti-cochlin-tompeitum antibody (anti-Coch) | Diagnostic |
| MRI gadolinium | Enhancement of labyrinth (acute phase) |
The most important test: A therapeutic trial of high-dose prednisolone (1mg/kg for 4 weeks) with audiometric monitoring. Hearing improvement confirms AIED. No other test is as definitive.
7. VESTIBULAR PAROXYSMIA
Neurovascular Compression of CN VIII — Massively Underdiagnosed
- Attacks last only seconds to minutes
- Misdiagnosed as: TIA, panic attacks, BPPV (brief), "cardiac causes"
- No standard test battery will catch it — diagnosis is clinical + MRI
| Feature | Description |
|---|---|
| Duration | Seconds to 2 minutes |
| Frequency | Multiple times per day (can be 30–40 attacks/day) |
| Trigger | Head position, hyperventilation, no trigger |
| Character | Brief spinning + tinnitus in the same ear each attack |
| Hyperventilation response | Positive — nystagmus induced → points to nerve |
| Response to carbamazepine | Dramatic — near-complete suppression |
| Test | Vestibular Paroxysmia Finding |
|---|---|
| VNG spontaneous | Normal (between attacks) |
| Hyperventilation nystagmus | POSITIVE — beats toward the compressed ear |
| vHIT | May show mild ipsilateral canal gain reduction |
| Caloric | Mild unilateral weakness (ipsilateral CN VIII) |
| ABR / MLR | Prolonged I–III interpeak latency ipsilateral |
| MRI CISS/FIESTA | Neurovascular contact/loop at CN VIII (AICA, PICA contact) |
| Trial of carbamazepine 200mg BD | Dramatic response = diagnostic |
This is the vestibular equivalent of trigeminal neuralgia. The hyperventilation-induced nystagmus on VNG is your screening test. Always order MRI CISS protocol if positive.
8. WHAT YOUR ECoG IS ACTUALLY TELLING YOU — BEYOND MÉNIÈRE'S
ECoG Reference Values:
| Parameter | Normal | Abnormal | Significance |
|---|---|---|---|
| SP/AP ratio | <0.40 (click) / <0.50 (tone burst) | >0.40–0.50 | Endolymphatic hydrops |
| SP amplitude | Small | Enlarged SP | Hydrops, perilymph fistula |
| AP threshold | Reflects hearing | Elevated | SNHL |
| Summating potential shape | Negative, small | Negative-enlarged / positive | Direction of hydrops |
| CM (cochlear microphonic) | Present, follows stimulus polarity | Absent | Auditory neuropathy spectrum disorder |
ECoG in Conditions Beyond Ménière's:
| Condition | ECoG Finding |
|---|---|
| Ménière's disease | SP/AP >0.45, enlarged negative SP |
| Perilymph fistula | Variable elevated SP/AP, may normalize after plugging |
| SCD | SP/AP may be mildly elevated (3rd window mimics hydrops) |
| Auditory neuropathy (ANSD) | Large CM present, AP absent — pathognomonic |
| Vestibular migraine | Normal SP/AP (KEY differentiator from Ménière's) |
| Endolymphatic hydrops without symptoms | Subclinical hydrops — patient at risk |
Critical for India: ANSD (auditory neuropathy spectrum disorder) is common in neonates with hyperbilirubinemia, prematurity, and hypoxia. ECoG with CM detection is diagnostic when ABR shows absent/grossly abnormal waves with present OAE. This is commonly missed.
9. MRI GADOLINIUM (HYDROPS-Mi2) — THE GAME-CHANGER YOU SHOULD BE REQUESTING
- Grade 0 = Normal (VM, no hydrops)
- Grade 1 = Mild hydrops (endolymph occupies <33% vestibule)
- Grade 2 = Severe hydrops (endolymph >33% vestibule, as in Ménière's)
- Ménière's-like symptoms but ECoG borderline
- VM vs Ménière's diagnostic dilemma
- Before intratympanic gentamicin (confirm hydrops exists)
- Monitoring treatment response
10. LLR / MLR — WHAT YOU ARE MISSING IN YOUR TEST BATTERY
MLR (Middle Latency Response — 10–50ms)
| Component | Generator | If Abnormal |
|---|---|---|
| Pa wave | Primary auditory cortex (Heschl's) | Cortical auditory processing disorder |
| Pb wave (P1) | Thalamo-cortical pathway | Thalamic relay dysfunction |
| Na wave | Thalamus / midbrain | Sub-cortical lesion |
- Absent/abnormal MLR ipsilateral to CPA lesion → vestibular schwannoma compressing cochlear nerve
- Bilateral abnormal MLR → auditory processing disorder (APD) — common in India's elderly but never tested
- Abnormal MLR with normal ABR → retro-cochlear between cochlear nucleus and cortex (MS lesion, central pathway)
LLR (Late/Long Latency Response — N1-P2-N2, 50–300ms)
| Clinical Use | How It Helps |
|---|---|
| Cortical auditory evoked potential (CAEP) | Hearing threshold in non-cooperative patients, malingerers |
| P300 (event-related potential) | Cognitive function — early dementia screening in dizzy elderly |
| Mismatch negativity (MMN) | Auditory discrimination — APD screening |
| N400 / P600 | Language processing disorders |
In a dizzy 67-year-old like your Bhardwaj case, a P300 test would tell you if there is concurrent cognitive decline contributing to gait and balance dysfunction — this is never done in India but is standard internationally.
11. THE VHIT BEYOND "PASS/FAIL" — WHAT THE NUMBERS TELL YOU
vHIT Gain Interpretation by Canal:
| VOR Gain | Interpretation |
|---|---|
| 0.8–1.0 | Normal |
| 0.6–0.79 | Mild hypofunction — compensated, subtle symptoms |
| 0.4–0.59 | Moderate hypofunction — symptomatic |
| <0.4 | Severe hypofunction |
| >1.0 | Hyperfunction — SCD (3rd window), superior canal dehiscence |
Canal-Specific Lesion Mapping from vHIT:
| Abnormal Canal | Nerve Division | Lesion Site |
|---|---|---|
| Horizontal + Anterior + Posterior (all 3) one side | Entire CN VIII | Complete vestibular neuritis or schwannoma |
| Horizontal alone | Superior vestibular nerve | Superior vestibular neuritis (commonest form) |
| Posterior alone | Inferior vestibular nerve | Inferior vestibular neuritis (rare, often missed) |
| Anterior alone | Superior vestibular nerve | Very rare, consider SCD |
| Bilateral all 6 canals | Both CN VIII | BVH |
| Anterior canal gain >1.0 | N/A | SCD ipsilateral |
Covert vs Overt Saccades:
| Saccade Type | Timing | Significance |
|---|---|---|
| Covert saccade | During head impulse | Acute/recent vestibular loss — no time to develop compensation |
| Overt saccade | After head stops | Chronic, compensated peripheral loss |
| Both present | — | Incomplete compensation |
| Neither (no saccade with symptoms) | — | CENTRAL — HINTS alarm |
12. VESTIBULAR SCREENING IN INDIA — SPECIFIC MISSED HISTORY QUESTIONS
Section A: Temporal Profile (most important)
- "Describe one typical attack from start to finish — how long does it last exactly?"
- "How often do attacks occur?"
- "Is there a warning before the attack?"
- "Is there anything between attacks — constant imbalance?"
Section B: Trigger Mapping (commonly skipped)
- "Does rolling over in bed cause it?" → BPPV
- "Does bending forward / looking up cause it?" → BPPV or orthostatic
- "Does standing up quickly cause it?" → Orthostatic hypotension
- "Does a loud sound cause dizziness or jumping of eyes?" → SCD
- "Does blowing your nose / straining at stool cause dizziness?" → SCD / PLF
- "Does it happen with physical exertion?" → SCD / cardiac
- "Does stress / anxiety trigger it?" → PPPD / VM
- "Does bright sunlight or visual patterns (escalators, tiles) cause it?" → PPPD / VM
Section C: Cochleo-Vestibular Symptoms Together
- "Does hearing drop during the attack?" → Ménière's
- "Do you hear a low roaring in the ear before the attack?" → Ménière's
- "Do you hear your own voice too loudly in one ear?" → SCD / PLF / patulous ET
- "Do you hear your heartbeat in your ear?" → SCD / dehiscent jugular bulb
- "Does your hearing fluctuate — good days and bad days?" → Ménière's / AIED / VM
Section D: India-Specific Red Flags (Never Skip)
- "Any TB treatment with injections?" → Aminoglycoside-BVH
- "Any history of malaria treatment with quinine?" → Ototoxicity
- "Any chemotherapy in the past?" → Cisplatin ototoxicity
- "Any ear drops containing neomycin / gentamicin through a perforated drum?" → Topical ototoxicity (massively over-used in India)
- "Any traditional medicine / herbal ear drops?" → Ayurvedic preparations causing perilymph fistula / ototoxicity
- "Any head trauma — road accident?" → Labyrinthine concussion, PLF, BPPV post-trauma
- "Any recent Dengue / Chikungunya / COVID infection?" → Post-viral labyrinthitis / AIED
- "Diabetes duration and control?" → Diabetic vestibulopathy — severely underdiagnosed in India
Section E: Functional Impact (Bárány Society PPPD Probe)
- "Are you avoiding going to markets, temples, crowds because of dizziness?" → PPPD avoidance behavior
- "Can you use your mobile/computer comfortably — does scrolling cause dizziness?" → Visual vertigo — PPPD
- "Do you drive? If not, when did you stop and why?" → Functional disability assessment
THE COMPLETE TEST BATTERY RECOMMENDATION BY PRESENTATION
| Clinical Presentation | Essential Tests | Additional Tests |
|---|---|---|
| Acute vertigo <72h | VNG (spontaneous + gaze) + vHIT + HINTS | MRI DWI if central signs |
| Recurrent episodic vertigo | VNG full + ECoG + vHIT + VEMP (c + o) | MRI gadolinium HYDROPS-Mi2 |
| Chronic imbalance | VNG full + bilateral caloric + bilateral vHIT + VEMP bilateral | P300, posturography |
| Positional vertigo | VNG Dix-Hallpike + roll + static positions | VEMP if atypical |
| Hearing + vertigo together | ECoG + VNG + vHIT + VEMP + ABR + audiometry | MRI gadolinium |
| Pulsatile tinnitus + dizziness with sound | cVEMP threshold testing + oVEMP + CT temporal (0.5mm) | MRI CPA |
| Bilateral imbalance in dark + oscillopsia | Bilateral vHIT + bilateral caloric + bilateral VEMP | Drug history, autoimmune screen |
| Chronic dizziness after previous episode | VNG + vHIT + VEMP + posturography | DHI questionnaire, P300 |
| Brief seconds-only attacks | VNG + vHIT + MRI CISS (neurovascular compression) | Carbamazepine trial |
| Child with fluctuating SNHL + dizziness | CT temporal bone + cVEMP threshold + audiometry | MRI endolymph |
FINAL SUMMARY — THE 5 RULES FOR INDIAN VESTIBULAR PRACTICE
Rule 1: Duration of attack is the most powerful single piece of history. Never accept "I get giddy" — pin down the exact timing.
Rule 2: Always ask about aminoglycoside exposure (gentamicin, streptomycin) for every patient with bilateral symptoms — India's TB burden makes this uniquely important.
Rule 3: A normal VNG does not mean a normal vestibular system. PPPD, SCD, BVH, VM, and vestibular paroxysmia can all have normal VNG. Know what each test measures.
Rule 4: The combination of normal vHIT + abnormal VNG/caloric = central lesion (HINTS positive). Never send this patient home without MRI.
Rule 5: PPPD is not a diagnosis of exclusion — it is a positive clinical diagnosis. Stop prescribing Stugeron and betahistine for years and start vestibular rehabilitation + SSRI.
I want to compete with neurologist otolaryngologist ENTs And other doctors in field of vestibular/vertigo. So how can you make me stronger (provide me the pictrorial representation). And please provide me the cases and treatment for the reference and whatever you can provide me to treat my patients best.
BPPV canalith repositioning Epley Semont maneuver treatment outcomes evidence posterior horizontal canal
Meniere disease treatment betahistine intratympanic gentamicin endolymphatic sac surgery low sodium diet diuretics
Epley maneuver canalith repositioning BPPV posterior canal step by step diagram
vestibular neuritis treatment corticosteroids methylprednisolone antiviral rehabilitation prognosis recovery VOR
PPPD persistent postural perceptual dizziness treatment vestibular rehabilitation SSRI sertraline CBT outcome
horizontal canal BPPV barbecue roll Lempert maneuver treatment diagram geotropic apogeotropic
vestibular migraine diagnosis criteria treatment prophylaxis topiramate propranolol amitriptyline
want to compete with neurologist otolaryngologist ENTs And other doctors in field of vestibular/vertigo. So how can you make me stronger (provide me the pictrorial representation). And please provide me the cases and treatment for the reference and whatever you can provide me to treat my patients best.
vestibular neuritis acute treatment methylprednisolone corticosteroids rehabilitation VOR recovery prognosis
PPPD persistent postural perceptual dizziness vestibular rehabilitation SSRI sertraline CBT functional dizziness treatment
Epley maneuver BPPV posterior canal canalith repositioning step by step otoconia semicircular canal
Meniere disease stepwise management lifestyle sodium restriction betahistine intratympanic steroid gentamicin surgery ablative
vestibular migraine treatment acute prophylaxis topiramate propranolol amitriptyline flunarizine magnesium evidence
horizontal canal BPPV Lempert barbecue roll maneuver geotropic apogeotropic nystagmus treatment
vestibular rehabilitation exercises gaze stabilization habituation Cawthorne Cooksey balance training
nystagmus patterns peripheral central comparison VNG findings diagnosis vertigo clinical
Kindly history of PsC BPPV right side
POSTERIOR SEMICIRCULAR CANAL BPPV — RIGHT SIDE
Complete Clinical History & Pathophysiology
ANATOMY RECAP — Why the Posterior Canal Matters
TYPICAL CLINICAL HISTORY — RIGHT POSTERIOR CANAL BPPV
"Doctor, whenever I lie down on my right side or turn over in bed to the right, I get intense spinning lasting about 10-20 seconds. It also happens when I tilt my head back to look up at a shelf, or when I bend forward to pick something from the floor. The spinning is very severe at the beginning but stops on its own."
| History Element | Right PSC BPPV Pattern |
|---|---|
| Onset | Sudden, positional — seconds after movement |
| Duration per episode | 10–30 seconds (canalolithiasis) |
| Triggers | Lying down RIGHT, rolling right in bed, looking up, bending forward, getting out of bed |
| Associated nausea | Often present during intense episodes |
| Headache | Absent (differentiates from VM) |
| Hearing loss/tinnitus | Absent (differentiates from Ménière's) |
| Continuous dizziness | Absent between episodes |
| Morning worse | YES — first positional change of day is worst |
| Fatigue | Episodes become less intense on repeated testing (fatigability) |
| Preceding event | Head trauma (30%), prolonged recumbency (bed rest, dental chair), vestibular neuritis, osteoporosis, vitamin D deficiency |
| Age/sex | Peaks 50–70 years, F > M (2:1) |
| Prior episodes | Often recurrent — can remit spontaneously then return |
- Prolonged recumbency (post-surgical, post-dengue/chikungunya fever)
- Vitamin D deficiency (extremely common in India — sun avoidance, indoor lifestyle)
- Post-vestibular neuritis BPPV (2–3 weeks after neuritis, debris dislodges)
- Post-head injury (road traffic accidents)
- Cervical manipulation/vigorous oil massage (champi)
VNG SIGNATURE — RIGHT POSTERIOR CANAL BPPV
| Parameter | Expected Finding |
|---|---|
| Nystagmus direction | Upbeat + RIGHT torsional (top pole of eye rotates toward right/affected ear) |
| Latency | 5–15 seconds (time from position to nystagmus onset) |
| Duration | 10–30 seconds |
| Fatigability | YES — diminishes with repeated testing |
| Reversal on sitting up | YES — brief downbeat + left torsional burst when returning to sitting |
| Dix-Hallpike Left | Negative (no nystagmus, or minimal) |
- Spontaneous nystagmus: absent
- Saccades: normal
- Smooth pursuit: normal
- Caloric: normal (labyrinth is intact)
- SVV: normal (≤2°)
- OKN: normal
EPLEY MANEUVER — RIGHT SIDE (Treatment)
- Sit upright, head turned 45° RIGHT (to bring right posterior canal into vertical plane)
- Dix-Hallpike position — lie back rapidly, head extending below table level, head still 45° right → wait for nystagmus to stop + 30 seconds
- Head turned 90° LEFT (now 45° left of midline) — debris rolls toward common crus → wait 30 seconds
- Body + head roll to LEFT lateral decubitus (nose down ~135° from starting position) → wait 30 seconds
- Return to sitting upright — head straight, then tuck chin slightly
- Sleep with head elevated 30–45° for 48 hours (controversial but widely practiced in India)
- Avoid lying on right side for 1 week
- If recurrence: repeat Epley or refer for vestibular rehab
M RANJEET SINGH (72M, CCDA00342) — VNG REPORT ANALYSIS
Date: 06-Apr-2026
FULL DATA EXTRACTION
1. SACCADES
| Test | Parameter | Right Eye | Left Eye | Normal |
|---|---|---|---|---|
| 0.3 Hz Horizontal | Velocity | 541 °/s | 907 °/s | >200 °/s |
| Precision | 86.3 | 84.7 | >80% ✓ | |
| Latency | 249 ms | 287 ms | 150–250 ms | |
| 0.45 Hz Horizontal | Velocity | 525 °/s | 691 °/s | — |
| Precision | 85.5 | 70.8 ⚠️ | >80% | |
| Latency | 215 ms | 248 ms | — | |
| 0.3 Hz Vertical | Velocity | 554 °/s | 450 °/s | — |
| Precision | 92.97 | 62.38 ⚠️ | >80% | |
| Latency | 258 ms | 316 ms ⚠️ | <250 ms | |
| 0.45 Hz Vertical | Velocity | 343 °/s | 474 °/s | — |
| Precision | 82.4 | 73.0 ⚠️ | >80% | |
| Latency | 246 ms | 303 ms ⚠️ | <250 ms |
- Left eye saccade precision reduced at higher frequencies (70.8% at 0.45Hz horizontal; 62.38% at 0.3Hz vertical) → LEFT eye hypometria
- Left eye latency prolonged in vertical saccades (303–316ms) → slowed left vertical saccade initiation
- Right vertical saccade velocity at 0.45Hz drops to 343°/s — possible early fatiguing
- Right eye saccades relatively preserved
2. SMOOTH PURSUIT — CRITICALLY ABNORMAL
| Frequency | Direction | Right Eye | Left Eye | Normal |
|---|---|---|---|---|
| 0.2 Hz H | Rightward | 0.46 ❌ | 0.43 ❌ | >0.70 |
| Leftward | 0.75 | 0.69 | >0.70 | |
| 0.4 Hz H | Rightward | 0.35 ❌❌ | 0.31 ❌❌ | >0.65 |
| Leftward | 0.43 ❌❌ | 0.38 ❌❌ | >0.65 | |
| 0.6 Hz H | Rightward | 0.14 ❌❌❌ | 0.15 ❌❌❌ | >0.55 |
| Leftward | 0.12 ❌❌❌ | 0.11 ❌❌❌ | >0.55 | |
| 0.2 Hz V | Upward | 0.29 ❌ | 0.36 ❌ | >0.60 |
| Downward | 0.27 ❌ | 0.24 ❌ | >0.60 | |
| 0.4 Hz V | Upward | 0.19 ❌❌ | 0.21 ❌❌ | >0.55 |
| Downward | 0.13 ❌❌❌ | 0.09 ❌❌❌ | >0.55 | |
| 0.6 Hz V | Upward | 0.15 ❌❌❌ | 0.15 ❌❌❌ | — |
| Downward | 0.10 ❌❌❌ | 0.07 ❌❌❌ | — |
3. OPTOKINETIC NYSTAGMUS (OKN)
| Direction | Right Eye | Left Eye | Normal |
|---|---|---|---|
| Left→Right 10° | 1.02 ✓ | 1.04 ✓ | >0.70 |
| Right→Left 10° | 0.89 | 0.85 | >0.70 |
| Top→Bottom 10° | 0.86 | 0.72 ⚠️ | >0.70 |
| Bottom→Top 10° | 0.95 | 0.86 | >0.70 |
| Left→Right 20° | 0.88 | 0.90 | >0.70 |
| Right→Left 20° | 0.81 | 0.75 ⚠️ | >0.70 |
4. SPONTANEOUS NYSTAGMUS
| Condition | Horizontal SPV | Vertical SPV |
|---|---|---|
| In Light | Absent | Absent |
| In Dark | Absent | Absent |
- No acute peripheral vestibular lesion
- No active neural integrator failure producing GEN at rest
- Background tone is equalized (compensated or bilateral)
5. HEAD SHAKE NYSTAGMUS
| Eye | Horizontal SPV | Amplitude | Frequency |
|---|---|---|---|
| Right | -2.25 °/s | -2.06° | 0.52 Hz |
| Left | Absent | — | — |
6. GAZE TESTS — CRITICAL FINDINGS
| Position | Finding |
|---|---|
| Center | Absent |
| Left | Absent |
| Right | Absent |
| Up | Absent |
| Down (Right Eye) | SPV 7.32°/s, Amplitude 2.37°, 1.24Hz ⚠️ |
| Position | Finding |
|---|---|
| Center | Absent |
| Left | Absent |
| Up | Absent |
| Right (Left Eye) | Horizontal SPV -7.67°/s, Amplitude -12.71°; Vertical SPV 4.41°/s; Fast Phase 198.20°, 0.99Hz ⚠️⚠️ |
| Down (Both eyes) | Horizontal SPV 2.63/3.01°/s, 0.41–0.50Hz ⚠️ |
- Downward gaze nystagmus with fixation (right eye): SPV 7.32°/s — this is a downbeat-type gaze-evoked nystagmus appearing at downward gaze. Localises to flocculus failure (flocculus normally suppresses downbeat drift)
- Rightward gaze without fixation (left eye): Left-beating horizontal nystagmus (-7.67°/s) + upward vertical component (4.41°/s) at rightward gaze. Fast phase 198° = leftward + slightly downward. This is a gaze-evoked nystagmus component revealed by removing fixation — the neural integrator cannot hold eccentric gaze, producing centripetal drift
- Downward gaze without fixation (both eyes): Horizontal nystagmus — drift in centripetal direction
7. POSITIONAL TESTS — THE KEY DIAGNOSTIC FINDING
DIX-HALLPIKE RIGHT
| Position | Finding |
|---|---|
| Sit Head Right (1st) | Absent |
| Supine Head Ext. + Right | H-SPV 6.06/9.49°/s; V-SPV -3.80/-6.85°/s; Fast Phase 11.08°/17.37°; Freq 2.06/2.46Hz ✓ |
| Sit Head Right (2nd) | V-SPV 7.20°/s right eye; 0.80Hz ✓ |
- Horizontal component: SPV ~6–9.5°/s, fast phase ~11–17° (rightward/torsional)
- Vertical component: SPV -3.8 to -6.85°/s (UPWARD fast phase, as negative = upward in this convention)
- Fast phase direction ~11–17° from horizontal = predominantly horizontal with upward torsional component
- Reversal nystagmus on sitting up (V-SPV 7.20°/s right eye) = confirms canalolithiasis repositioning
DIX-HALLPIKE LEFT
| Position | Finding |
|---|---|
| Sit Head Left (1st) | Absent |
| Supine Head Ext. + Left | H-SPV 7.02°/s (right eye); V-SPV 9.78/9.55°/s; Fast Phase 322.64°; Freq 1.79/0.95Hz |
| Sit Head Left (2nd) | H-SPV -9.02°/s left eye; V-SPV 4.11°/s right eye; Freq 0.68/0.69Hz |
- Fast phase direction 322.64° = geotropic/torsional, upper pole toward LEFT ear (counterclockwise)
- Horizontal component 7.02°/s toward right eye
- Vertical component 9.78°/s upward
- Bilateral posterior canal BPPV (right > left)
- Left anterior canal BPPV (produces down-beat + torsional toward right, similar appearance in DH-left)
- Central positional nystagmus — since nystagmus appears in both DH positions
McCLURE-PAGNINI (Supine Roll Test)
| Position | Finding |
|---|---|
| Sit to Supine | V-SPV 8.34/7.59°/s; Freq 0.69/0.53Hz ⚠️ |
| Right Lateral | H+V nystagmus: H-SPV 4.95/4.25°/s; V-SPV 7.92/7.19°/s; Fast Phase 310°/301°; Freq 1.87/1.61Hz |
| Supine Neutral (1) | Absent |
| Left Lateral | V-SPV 5.60°/s right eye; Freq 0.59Hz |
| Supine Neutral (2) | Absent |
8. SUBJECTIVE VISUAL VERTICAL — NORMAL
| Trial | Deviation |
|---|---|
| Clockwise | 0° |
| Anticlockwise | -1° Left |
| Blank background | -1° Left |
SYNTHESIS & DIAGNOSIS
Findings Summary Table
| Domain | Result | Significance |
|---|---|---|
| Horizontal saccades | Mildly reduced precision (left eye at 0.45Hz) | Subtle left eye oculomotor issue |
| Vertical saccades | Left eye precision 62–73% ❌, latency 303–316ms ❌ | Left eye vertical saccade dysmetria |
| Smooth pursuit ALL directions | 0.07–0.46 ❌❌❌ | Severe bilateral central pursuit failure |
| OKN | Relatively preserved | Central/cortical pursuit problem, not global |
| Spontaneous nystagmus | Absent | No acute peripheral lesion |
| Head shake | Weak left-beat (2.25°/s) | Mild left labyrinthe asymmetry |
| Gaze-evoked nystagmus (down with fixation) | 7.32°/s | Floccular integrator failure |
| Gaze-evoked nystagmus (right without fixation) | -7.67°/s | Neural integrator failure, fixation suppressed it |
| DH-Right positional | Upbeat-torsional; H 6-9.5°/s; Fast phase 11-17° | RIGHT POSTERIOR CANAL BPPV ✓ |
| DH-Left positional | Upbeat-torsional; Fast phase 322°; bilateral | Left canal involvement or bilateral BPPV |
| McClure-Pagnini Right Lateral | Apogeotropic H+V; Fast phase 310° | Possible horizontal canal component |
| SVV | 0 to -1° | Normal — no utricular/central tilt |
PRIMARY DIAGNOSIS
RIGHT POSTERIOR CANAL BPPV (Canalolithiasis)
-
RIGHT PSC BPPV (primary complaint, treatable)
- Classic DH-Right: upbeat + right torsional, 6–9°/s, with reversal on sitting up
- Treatable with RIGHT EPLEY MANEUVER immediately
-
Central smooth pursuit failure (background finding, concerning)
- ALL pursuit gains severely reduced bilaterally (0.07–0.46, normal >0.70)
- Gaze-evoked nystagmus at downward gaze (7.32°/s)
- Rightward GEN without fixation
- 72-year-old male with this pattern requires investigation
- Differential: cerebellar atrophy (most common in elderly), olivopontocerebellar degeneration, MSA-C, medication effect (anticonvulsants), posterior fossa mass
WHAT TO DO NOW
Immediate Action:
Further Investigation:
- Cerebellar cortical atrophy (flocculus/vermis)
- White matter changes
- Rule out mass/metastasis
- Is this patient on carbamazepine, phenytoin, phenobarbitone, or any vestibular suppressant? All cause pursuit failure dose-dependently
- Benzodiazepines?
- vHIT (if available) — assess semicircular canal VOR gain
- cVEMP/oVEMP — assess saccule/utricle (SVV normal suggests utricle intact, but functional confirmation helpful)
TREATMENT PLAN
Step 1 — RIGHT EPLEY MANEUVER (Do today)
- Sit patient upright, turn head 45° RIGHT
- Quickly move to DH-right position, wait for nystagmus + 30s
- Rotate head 90° LEFT (nose 45° left of midline), wait 30s
- Roll body + head to left lateral (nose toward floor), wait 30s
- Return to sitting, chin tuck
Step 2 — Vitamin D + Calcium
- Check serum 25-OH vitamin D (most Indian patients will be deficient)
- Supplement: Cholecalciferol 60,000 IU weekly × 8 weeks, then monthly
- Calcium 500mg BD (prevents recurrence — strong evidence in Indian literature)
Step 3 — Vestibular Rehabilitation
- For residual unsteadiness post-Epley and for coexisting central pursuit failure
- Gaze stabilization exercises
- Dynamic balance training
Step 4 — Neurology/MRI Referral
- MRI posterior fossa
- Neurologist co-management if cerebellar degeneration confirmed
REPORT DICTATION (Ready to use)
- Immediate right Epley maneuver for BPPV
- MRI brain with posterior fossa protocol
- Medication review (anticonvulsants/benzodiazepines)
- Vestibular rehabilitation post-repositioning
- Vitamin D and calcium supplementation
CLINICAL TEACHING POINT — This Case Illustrates a Critical Concept
Never let BPPV distract you from a coexisting central finding.