Malformations of the genitourinary system: Hypospadias. Epispadias-D
Reading File
search_medical_text
hypospadias epispadias genitourinary malformations anatomy classification surgery
search_medical_image
hypospadias epispadias anatomy diagram classification
GradeResponse
GradeResponse
search_medical_text
hypospadias embryology incidence chordee surgical repair urethroplasty
search_medical_image
epispadias bladder exstrophy complex penis dorsal defect
GradeResponse
GradeResponse
I now have sufficient material to compose a comprehensive answer. Let me synthesize it all.
Malformations of the Genitourinary System: Hypospadias & Epispadias
I. HYPOSPADIAS
Definition
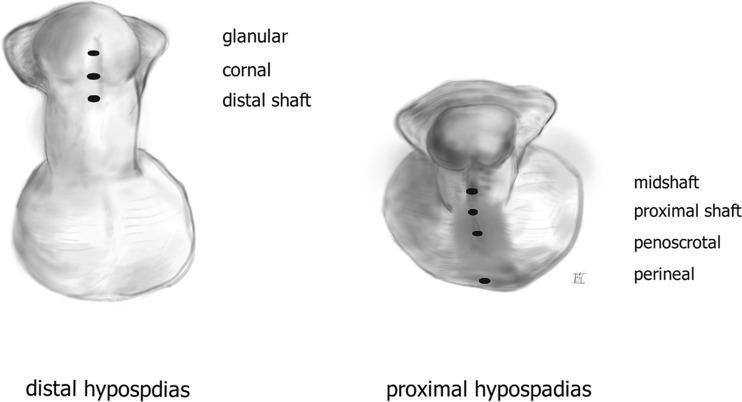
Hypospadias is a congenital malformation in which the urethral meatus opens on the ventral (inferior) surface of the penis — anywhere from the glans to the perineum — rather than at the tip of the glans. It is often accompanied by chordee (ventral penile curvature) and a dorsally hooded prepuce.
Embryology
Normal urethral development depends on androgen-driven fusion of the urethral folds along the ventral midline (weeks 8–14 of gestation). Failure of complete fusion leads to hypospadias. The more proximal the arrest, the more severe the defect.
Incidence
- Approximately 1 in 200–300 male births (one of the most common congenital penile anomalies)
- Higher incidence in first-degree relatives
Classification
Classified by the location of the ectopic meatus:
| Type | Meatal Position |
|---|---|
| Distal (anterior) | Glanular, coronal, distal shaft (~70%) |
| Middle | Midshaft |
| Proximal (posterior) | Proximal shaft, penoscrotal, scrotal, perineal (~30%) |
Clinical Features
- Abnormal urinary stream (deflected downward/ventral)
- Chordee — ventral curvature of the penis (more common in proximal types)
- Dorsal hooded prepuce (incomplete foreskin ventrally)
- Difficulty with micturition in proximal types
- Psychosocial / sexual dysfunction if untreated
Associations
- Cryptorchidism (~10%)
- Inguinal hernia
- In severe cases: disorders of sex development (DSD) should be excluded
Management
(Bailey & Love's, p. 1561)
Surgical correction is the mainstay:
- Timing: Ideally before 18 months of age
- Distal hypospadias:
- Often repaired for cosmetic and functional reasons
- Technique of choice: Tubularised Incised Plate (TIP) urethroplasty (Snodgrass procedure)
- Proximal hypospadias with chordee: Two-stage repair
- Stage 1: Correct penile curvature (chordee release ± skin grafting)
- Stage 2: Urethral reconstruction (urethroplasty using preputial or buccal mucosa)
- Circumcision should be avoided prior to repair — preputial skin is valuable tissue for reconstruction
Complications of Surgery
- Urethrocutaneous fistula (most common)
- Meatal stenosis
- Urethral stricture
- Wound dehiscence
- Persistent/recurrent chordee
II. EPISPADIAS
Definition
Epispadias is a rare congenital dorsal penile defect in which the urethral meatus opens on the dorsal (superior) surface of the penis. The opening may lie anywhere from the glans to the penopubic junction (Bailey & Love's, p. 300).
A useful conceptual mnemonic: if hypospadias results from a ventral opening (scissors blade into the urethra, cutting ventrally), epispadias is the dorsal counterpart — cutting dorsally through the penis and pubis into the bladder.
Incidence
- Much rarer than hypospadias: ~1 in 117,000 males, ~1 in 484,000 females
Embryology
Results from failure of the cloacal membrane to be replaced by mesenchymal tissue during embryogenesis, leading to premature rupture of the cloacal/urogenital membrane.
Classification (Males)
| Type | Description |
|---|---|
| Glanular | Meatus on dorsal glans (mildest) |
| Penile | Meatus on dorsal shaft |
| Penopubic (complete) | Meatus at penopubic junction; sphincter usually incompetent → incontinence |
Epispadias–Exstrophy Complex
Epispadias exists on a spectrum with bladder exstrophy:
| Condition | Features |
|---|---|
| Isolated epispadias | Dorsal penile opening only; bladder intact |
| Bladder exstrophy | Bladder and bladder neck open on lower abdominal wall; epispadias always present |
| Cloacal (ileocaecal) exstrophy | Most severe variant: exomphalos + everted caecum/ileum separating two bladder halves + split penis |

Clinical Features
- Dorsal urethral opening on the penis
- Dorsal chordee (upward penile curvature)
- Urinary incontinence — common, especially in penopubic type (incompetent bladder neck)
- Widened pubic symphysis (diastasis) in exstrophy
- Fertility issues — retrograde ejaculation, epididymo-orchitis risk
In Females
- Short, wide urethra with cleft clitoris
- Incontinence is the predominant symptom
- Bifid clitoris
Management
Complex multistep surgical reconstruction, often in a staged approach:
- Penile/bladder neck reconstruction — restore continence
- Urethral reconstruction — tubularize the dorsal urethral plate
- Pelvic osteotomy — for bladder exstrophy (to close the pubic diastasis)
- Bladder augmentation / urinary diversion — in severe exstrophy
- Boys with epispadias and a functioning bladder neck may achieve continence with reconstructive surgery alone (Bailey & Love's, p. 300)
III. COMPARISON: Hypospadias vs. Epispadias
| Feature | Hypospadias | Epispadias |
|---|---|---|
| Meatal location | Ventral surface | Dorsal surface |
| Chordee direction | Ventral (downward) | Dorsal (upward) |
| Incidence | ~1:200–300 | ~1:117,000 |
| Incontinence | Rare | Common (penopubic type) |
| Associated anomaly | Cryptorchidism, hernia | Bladder exstrophy, diastasis pubis |
| Prepuce | Dorsal hood | Often absent/abnormal |
| Surgical timing | Before 18 months | Staged from neonatal period |
| Key repair | TIP urethroplasty | Bladder/urethra reconstruction ± osteotomy |
Sources: Bailey and Love's Short Practice of Surgery, 28th Edition (pp. 300, 1561)
Treatment differenc3 between men and female
search_medical_text
hypospadias epispadias treatment female women surgical repair
search_medical_text
epispadias male female management incontinence reconstruction bladder neck
GradeResponse
GradeResponse
Here is a focused comparison of treatment differences between males and females for both conditions:
Treatment Differences: Male vs. Female
HYPOSPADIAS
Males
Hypospadias is almost exclusively a male condition (the urethra must travel the length of the penis). Treatment is well-established and surgical:
- Distal types: Tubularised Incised Plate (TIP) urethroplasty — the urethral plate is incised and tubularised to bring the meatus to the glans tip
- Proximal types with chordee: Two-stage repair
- Stage 1 — chordee release ± skin/buccal mucosa graft
- Stage 2 — urethroplasty (urethral tube construction)
- Circumcision avoided pre-operatively (preputial skin needed for repair)
- Goal: functional meatus at glans tip, straight penis, normal voiding stream
Females
True hypospadias in females is extremely rare (female urethra is short and rarely malformed in the same way). When a female urethral anomaly occurs, it is usually:
- A urethral diverticulum (causing recurrent UTIs, post-void dribbling) — treated by surgical excision
- A urethral caruncle (minor mucosal prolapse) — usually requires no treatment (Bailey & Love's, p. 1471)
- Rarely, a low-opening urethra as part of a disorder of sex development (DSD) — managed by a multidisciplinary team
EPISPADIAS
Males
The male presentation is more anatomically complex, so treatment is more extensive:
| Goal | Procedure |
|---|---|
| Urethral reconstruction | Tubularisation of the dorsal urethral plate |
| Correct dorsal chordee | Penile straightening / corporoplasty |
| Restore continence | Bladder neck reconstruction (Young-Dees-Leadbetter procedure) |
| Pelvic stability (exstrophy) | Pelvic osteotomy to close pubic diastasis |
| Bladder capacity | Bladder augmentation if needed |
| Cosmesis | Penile/glans reconstruction |
- Boys with a functioning bladder neck may achieve continence with urethral repair alone (Bailey & Love's, p. 300)
- Boys with bladder exstrophy require staged neonatal closure of the bladder plate as the first priority
Females
Female epispadias is rarer and anatomically different — there is no long urethra or penis involved. The key features and treatment goals differ:
| Feature | Female |
|---|---|
| Anatomy | Bifid/cleft clitoris, patulous short urethra, open dorsal urethral roof |
| Dominant symptom | Urinary incontinence (nearly universal — bladder neck is always incompetent in females) |
| Main surgical goal | Continence restoration |
Female-specific procedures:
- Bladder neck reconstruction is the primary surgical priority (since virtually all females with epispadias are incontinent)
- Urethral lengthening — the female urethra is reconstructed/lengthened to restore resistance
- Clitoroplasty — repair of the bifid clitoris for cosmesis
- Vaginal/pelvic floor repair if associated exstrophy is present
- Pelvic osteotomy — when pubic diastasis is present (bladder exstrophy cases)
Summary Table
| Aspect | Male | Female |
|---|---|---|
| Hypospadias | Common; TIP urethroplasty or 2-stage repair | Extremely rare; usually a diverticulum or caruncle — minimal/no surgery |
| Epispadias anatomy | Dorsal urethral opening on penis ± split penis | Bifid clitoris, patulous short urethra |
| Dominant problem | Voiding abnormality + chordee + incontinence | Almost always incontinence |
| Urethral repair | Tubularisation + penile reconstruction | Urethral lengthening |
| Continence procedure | Bladder neck repair (if incompetent) | Always required — bladder neck reconstruction is the primary goal |
| Cosmetic repair | Glans/penile reconstruction | Clitoroplasty |
| Osteotomy | Required in exstrophy | Required in exstrophy |
| Staged approach | Yes — often 2–3 stages | Yes — continence first, then cosmesis |
Key principle: In males, the treatment priority balances urethral reconstruction + penile cosmesis + continence. In females, continence is the dominant and most urgent surgical goal, as bladder neck incompetence is almost universal in female epispadias.
Sources: Bailey and Love's Short Practice of Surgery, 28th Edition (pp. 300, 1471)
Antimicrobial, antibacterial, antifungal,antiviral drugs of pharma in short for notes
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I have rich content from Lippincott's Pharmacology covering all the drug classes. I have enough to build comprehensive notes. Let me compile the full answer now.
Antimicrobial Drugs — Short Notes for Pharmacology
I. ANTIBACTERIAL DRUGS
A. β-LACTAMS
1. Penicillins
- MOA: Inhibit bacterial cell wall synthesis by binding Penicillin-Binding Proteins (PBPs) → block transpeptidation (cross-linking of peptidoglycan) → cell lysis. Bactericidal, time-dependent.
- Resistance: β-lactamase production (most S. aureus); reduced PBP affinity (MRSA)
| Group | Drugs | Spectrum |
|---|---|---|
| Natural | Penicillin G (IV), Penicillin V (oral) | G+, spirochetes (syphilis, gas gangrene) |
| Penicillinase-resistant | Cloxacillin, Nafcillin, Oxacillin | MSSA (not MRSA) |
| Aminopenicillins | Ampicillin, Amoxicillin | G+, some G− (H. influenzae, E. coli) |
| Extended-spectrum | Piperacillin, Ticarcillin | Pseudomonas + G− |
| + β-lactamase inhibitor | Amoxicillin-clavulanate, Piperacillin-tazobactam | Broad including β-lactamase producers |
2. Cephalosporins
- MOA: Same as penicillins (PBP binding)
- Generations:
| Generation | Drugs | Coverage |
|---|---|---|
| 1st | Cephalexin, Cefazolin | G+ (MSSA, Strep) |
| 2nd | Cefuroxime, Cefoxitin | G+ + some G− (H. influenzae) |
| 3rd | Ceftriaxone, Cefotaxime, Ceftazidime | Broad G−, CSF penetration, meningitis |
| 4th | Cefepime | G+ + G− including Pseudomonas |
| 5th | Ceftaroline | MRSA + broad G− |
3. Carbapenems
- Drugs: Imipenem, Meropenem, Ertapenem
- MOA: Broadest β-lactam spectrum — G+, G−, anaerobes
- Use: Serious/polymicrobial infections, ESBL-producing organisms
- Note: Imipenem given with cilastatin (prevents renal degradation); can cause seizures
4. Monobactams
- Drug: Aztreonam
- Spectrum: G− only (including Pseudomonas); safe in penicillin allergy
B. GLYCOPEPTIDES
- Drugs: Vancomycin, Teicoplanin
- MOA: Bind D-Ala-D-Ala terminus of peptidoglycan precursors → inhibit cell wall synthesis. Bactericidal.
- Use: MRSA, C. difficile (oral vancomycin), serious G+ infections
- ADRs: "Red man syndrome" (rapid infusion), nephrotoxicity, ototoxicity
C. PROTEIN SYNTHESIS INHIBITORS
| Drug Class | Drugs | Ribosomal Target | Effect |
|---|---|---|---|
| Aminoglycosides | Gentamicin, Amikacin, Tobramycin, Streptomycin | 30S | Bactericidal |
| Tetracyclines | Tetracycline, Doxycycline, Minocycline | 30S | Bacteriostatic |
| Chloramphenicol | Chloramphenicol | 50S (23S rRNA) | Bacteriostatic |
| Macrolides | Erythromycin, Azithromycin, Clarithromycin | 50S (23S rRNA) | Bacteriostatic |
| Clindamycin | Clindamycin | 50S | Bacteriostatic |
| Oxazolidinones | Linezolid | 50S (30S+50S initiation) | Bacteriostatic |
| Streptogramins | Quinupristin/Dalfopristin | 50S | Bactericidal |
Key mnemonics:
- 30S inhibitors: "Aminoglycosides Tetracyclines" → AT 30
- 50S inhibitors: "CELL" → Chloramphenicol, Erythromycin (macrolides), Linezolid, cLindamycin
D. FLUOROQUINOLONES
- Drugs: Ciprofloxacin, Levofloxacin, Moxifloxacin, Norfloxacin
- MOA: Inhibit DNA gyrase (topoisomerase II) and topoisomerase IV → prevent DNA supercoiling/separation → bactericidal
- Spectrum: Broad G+, G−, atypicals (Mycoplasma, Chlamydia), mycobacteria
- ADRs: Tendon rupture (Achilles), QT prolongation, cartilage damage (avoid in children/pregnancy), photosensitivity
E. SULFONAMIDES & TRIMETHOPRIM
- MOA:
- Sulfonamides (Sulfamethoxazole): inhibit dihydropteroate synthase → block folate synthesis
- Trimethoprim: inhibits dihydrofolate reductase → block THF production
- Together (Co-trimoxazole/TMP-SMX): sequential blockade of folate pathway → bactericidal synergy
- Use: UTIs, Pneumocystis jirovecii pneumonia (PCP), Nocardia, Toxoplasma
F. OTHER ANTIBACTERIALS
| Drug | MOA | Key Use |
|---|---|---|
| Metronidazole | Forms free radicals → DNA strand breakage | Anaerobes, C. difficile, H. pylori, protozoal (Giardia, Trichomonas) |
| Rifampicin | Inhibits bacterial RNA polymerase (β-subunit) | TB, leprosy, meningococcal prophylaxis |
| Isoniazid (INH) | Inhibits mycolic acid synthesis (InhA) | TB (first-line) |
| Linezolid | 50S — inhibits initiation complex formation | MRSA, VRE |
| Daptomycin | Disrupts cell membrane (Ca²⁺-dependent) | MRSA, VRE (skin + bacteremia) |
| Polymyxins (Colistin) | Detergent-like disruption of outer membrane | MDR G− (last resort) |
| Mupirocin | Inhibits isoleucyl-tRNA synthetase | Topical — impetigo, MRSA nasal decolonization |
II. ANTIFUNGAL DRUGS
A. POLYENES
- Drugs: Amphotericin B, Nystatin
- MOA: Bind ergosterol in fungal cell membrane → form pores → ion leakage → cell death. Fungicidal.
- Amphotericin B: IV; broad spectrum (Candida, Aspergillus, Cryptococcus, endemic fungi)
- ADRs: Nephrotoxicity (dose-limiting), infusion reactions (fever, rigors), hypokalemia, hypomagnesemia; use liposomal form to reduce toxicity
- Nystatin: Topical/oral only (too toxic for systemic use); oral/vaginal Candida
B. AZOLES
- MOA: Inhibit 14α-demethylase (CYP450 enzyme) → block lanosterol → ergosterol conversion → membrane dysfunction. Fungistatic (mostly).
| Drug | Route | Use |
|---|---|---|
| Fluconazole | Oral/IV | Candida (UTI, thrush, systemic), Cryptococcal meningitis |
| Itraconazole | Oral | Histoplasma, Aspergillus, dermatophytes, Blastomyces |
| Voriconazole | Oral/IV | Aspergillus (drug of choice), invasive mold infections |
| Ketoconazole | Topical | Dermatophytes, seborrheic dermatitis |
| Clotrimazole | Topical | Vaginal Candida, oral thrush, tinea |
| Posaconazole | Oral/IV | Prophylaxis in immunocompromised; mucormycosis |
- ADRs: Hepatotoxicity, CYP450 inhibition (drug interactions), teratogenic
C. ECHINOCANDINS
- Drugs: Caspofungin, Micafungin, Anidulafungin
- MOA: Inhibit β-(1,3)-D-glucan synthase → disrupt fungal cell wall synthesis. Fungicidal against Candida.
- Use: Invasive Candida (including azole-resistant), Aspergillus (2nd line)
- ADRs: Generally well tolerated; mild hepatotoxicity, histamine release
D. ALLYLAMINES
- Drugs: Terbinafine, Naftifine
- MOA: Inhibit squalene epoxidase → block ergosterol synthesis → squalene accumulates (toxic to fungi)
- Use: Dermatophytes (tinea unguium/nail fungus, tinea pedis) — oral/topical
E. OTHER ANTIFUNGALS
| Drug | MOA | Use |
|---|---|---|
| Flucytosine (5-FC) | Converted to 5-FU → inhibits fungal DNA/RNA synthesis | Combined with Amphotericin B for Cryptococcal meningitis |
| Griseofulvin | Inhibits fungal mitosis (microtubule disruption) | Dermatophytes (tinea capitis, onychomycosis) — oral |
III. ANTIVIRAL DRUGS
A. ANTI-HERPESVIRUS AGENTS
- MOA: Nucleoside analogues → phosphorylated by viral thymidine kinase → incorporated into viral DNA → chain termination
| Drug | Use |
|---|---|
| Acyclovir | HSV-1, HSV-2, VZV (chickenpox, shingles) |
| Valacyclovir | Prodrug of acyclovir; better oral bioavailability |
| Ganciclovir | CMV (retinitis, colitis in immunocompromised) |
| Valganciclovir | Oral prodrug of ganciclovir |
| Famciclovir | HSV, VZV |
| Foscarnet | CMV, acyclovir-resistant HSV; inhibits viral DNA polymerase directly (no kinase needed) |
| Cidofovir | CMV retinitis; broad antiviral (poxviruses, adenovirus) |
B. ANTI-INFLUENZA AGENTS
| Drug | MOA | Use |
|---|---|---|
| Oseltamivir (Tamiflu) | Neuraminidase inhibitor → prevents viral release | Influenza A & B |
| Zanamivir (Relenza) | Neuraminidase inhibitor (inhaled) | Influenza A & B |
| Amantadine / Rimantadine | Block M2 ion channel → prevent uncoating | Influenza A only (high resistance now) |
| Baloxavir | Inhibits cap-dependent endonuclease | Influenza A & B |
C. ANTIRETROVIRALS (HIV)
| Class | Drugs | MOA |
|---|---|---|
| NRTIs (Nucleoside RTIs) | Zidovudine (AZT), Lamivudine, Tenofovir, Emtricitabine | Inhibit reverse transcriptase (chain termination) |
| NNRTIs (Non-nucleoside RTIs) | Efavirenz, Nevirapine, Rilpivirine | Non-competitively inhibit reverse transcriptase |
| PIs (Protease inhibitors) | Ritonavir, Lopinavir, Atazanavir, Darunavir | Inhibit HIV protease → immature virions |
| INSTIs (Integrase inhibitors) | Raltegravir, Dolutegravir, Bictegravir | Inhibit integrase → prevent viral DNA integration |
| Fusion inhibitor | Enfuvirtide (T-20) | Blocks gp41-mediated fusion |
| CCR5 antagonist | Maraviroc | Blocks CCR5 co-receptor entry |
- HAART/ART: Combination therapy — typically 2 NRTIs + 1 NNRTI or INSTI
D. ANTI-HEPATITIS AGENTS
| Drug | Target | Use |
|---|---|---|
| Interferon-α | Immunomodulator | Hep B & C (older regimen) |
| Entecavir, Tenofovir | HBV DNA polymerase | Chronic Hepatitis B (first-line) |
| Lamivudine, Adefovir | HBV DNA polymerase | Chronic Hepatitis B |
| Sofosbuvir | NS5B (HCV RNA polymerase) | Hepatitis C |
| Ledipasvir, Daclatasvir | NS5A inhibitor | Hepatitis C |
| Simeprevir | NS3/4A protease | Hepatitis C |
| Combination (e.g. Sofosbuvir/Ledipasvir) | Multi-target | Hepatitis C — >95% cure rates |
E. MISCELLANEOUS ANTIVIRALS
| Drug | Use |
|---|---|
| Ribavirin | RSV (inhaled), Hep C (with interferon), Lassa fever |
| Remdesivir | COVID-19, Ebola (RNA polymerase inhibitor) |
QUICK SUMMARY TABLE
| Category | MOA Key Target | Bactericidal/Static |
|---|---|---|
| β-lactams | PBPs / cell wall | Cidal |
| Glycopeptides | D-Ala-D-Ala / cell wall | Cidal |
| Aminoglycosides | 30S ribosome | Cidal |
| Tetracyclines | 30S ribosome | Static |
| Macrolides / Clindamycin | 50S ribosome | Static |
| Chloramphenicol | 50S ribosome | Static |
| Fluoroquinolones | DNA gyrase / Topo IV | Cidal |
| Sulfonamides/TMP | Folate synthesis | Cidal (combination) |
| Rifampicin | RNA polymerase | Cidal |
| Polyenes | Ergosterol (membrane pores) | Fungicidal |
| Azoles | 14α-demethylase (ergosterol) | Fungistatic |
| Echinocandins | β-glucan synthase (cell wall) | Fungicidal |
| Nucleoside antivirals | Viral DNA/RNA polymerase | — |
| NRTIs/NNRTIs | Reverse transcriptase | — |
| Protease inhibitors | HIV protease | — |
Sources: Katzung's Basic & Clinical Pharmacology, 16th Ed. — Lippincott Illustrated Reviews: Pharmacology — Goodman & Gilman's Pharmacological Basis of Therapeutics
Antiallergic drugs
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Excellent content from both Lippincott and Katzung. I have more than enough to write comprehensive notes. Let me compile now.
Antiallergic Drugs — Short Notes for Pharmacology
BACKGROUND: HISTAMINE & ALLERGY
- Histamine is synthesized by decarboxylation of L-histidine (enzyme: histidine decarboxylase)
- Stored in mast cell & basophil granules, ECL cells of stomach, neurons
- Released by: IgE-mediated degranulation (allergy/anaphylaxis), cold, trauma, venoms, drugs
- Mediates: immediate allergic reactions (urticaria, rhinitis, anaphylaxis), gastric acid secretion, neurotransmission
| Receptor | Location | Effect when activated |
|---|---|---|
| H1 | Smooth muscle, endothelium, CNS | Bronchoconstriction, ↑ vascular permeability, itch, pain |
| H2 | Gastric parietal cells, heart | ↑ Gastric acid, ↑ HR |
| H3 | CNS (presynaptic) | Modulate neurotransmitter release |
| H4 | Immune cells | Chemotaxis, inflammation |
I. H1 ANTIHISTAMINES (Main Antiallergic Drugs)
MOA
- Inverse agonists at H1 receptors (not simple competitive antagonists)
- Stabilize the inactive form of H1 receptor → reduce histamine-driven allergic response
- Block: bronchoconstriction, itch, urticaria, vascular permeability, rhinorrhea
Generation 1 (Sedating / Classical)
Key feature: Lipid-soluble → cross BBB → CNS sedation; also have anticholinergic effects
| Drug | Brand | Notes |
|---|---|---|
| Diphenhydramine | Benadryl | Most sedating; also used for motion sickness, insomnia |
| Chlorpheniramine | — | Most commonly used 1st-gen; moderate sedation |
| Promethazine | Phenergan | Strong sedation; antiemetic; antipsychotic-like |
| Cyproheptadine | — | Also a serotonin antagonist; used for appetite stimulation, migraine |
| Hydroxyzine | Vistaril | Anxiolytic + antipruritic |
| Dimenhydrinate | Dramamine | Motion sickness |
| Meclizine | Antivert | Motion sickness, vertigo |
| Clemastine | — | Urticaria, allergic rhinitis |
| Doxylamine | Unisom | Sedative; pregnancy nausea (with B6) |
ADRs of 1st Gen:
- Sedation, drowsiness (major)
- Anticholinergic: dry mouth, blurred vision, urinary retention, constipation, tachycardia
- Paradoxical CNS stimulation in children
Generation 2 (Non-Sedating / Modern)
Key feature: Poorly lipid-soluble → minimal BBB penetration → no/minimal sedation; no anticholinergic effects; longer duration
| Drug | Brand | Notes |
|---|---|---|
| Loratadine | Claritin | Prototype 2nd-gen; once daily; safe in pregnancy |
| Desloratadine | Clarinex | Active metabolite of loratadine; more potent |
| Cetirizine | Zyrtec | Metabolite of hydroxyzine; mild sedation possible |
| Levocetirizine | Xyzal | Active enantiomer of cetirizine; less sedating |
| Fexofenadine | Allegra | Metabolite of terfenadine; most non-sedating |
Topical/ophthalmic:
| Drug | Use |
|---|---|
| Azelastine | Nasal spray (allergic rhinitis); ophthalmic |
| Olopatadine | Ophthalmic (allergic conjunctivitis) |
| Alcaftadine | Ophthalmic |
| Bepotastine | Ophthalmic |
| Ketotifen | Ophthalmic |
Clinical Uses of H1 Antihistamines
- Allergic rhinitis
- Urticaria / angioedema
- Allergic conjunctivitis
- Motion sickness (1st gen)
- Insomnia / sedation (1st gen)
- Pruritus (itching)
- Anaphylaxis (adjunct — NOT first-line; epinephrine is first-line)
II. H2 ANTIHISTAMINES
- MOA: Block H2 receptors on gastric parietal cells → ↓ gastric acid secretion
- Primary use: Peptic ulcer, GERD, Zollinger-Ellison (largely replaced by PPIs)
- Also used as adjunct in anaphylaxis (with H1 blockers + epinephrine)
| Drug | Notes |
|---|---|
| Ranitidine | Withdrawn (NDMA contamination) |
| Famotidine | Most potent H2 blocker; no CYP450 interaction |
| Cimetidine | First H2 blocker; significant CYP450 inhibitor (drug interactions); anti-androgenic |
| Nizatidine | Similar to ranitidine |
III. MAST CELL STABILIZERS
- MOA: Prevent degranulation of mast cells → block release of histamine, leukotrienes, and other mediators
- Act prophylactically — must be used before allergen exposure; not effective once reaction has started
| Drug | Route | Use |
|---|---|---|
| Cromolyn sodium (Sodium cromoglicate) | Inhaled, nasal, ophthalmic, oral | Asthma prophylaxis, allergic rhinitis, conjunctivitis, mastocytosis |
| Nedocromil | Inhaled | Mild-moderate asthma prophylaxis |
| Ketotifen | Oral / ophthalmic | Asthma, allergic conjunctivitis (also H1 blocker) |
| Lodoxamide | Ophthalmic | Allergic conjunctivitis |
IV. LEUKOTRIENE RECEPTOR ANTAGONISTS (LTRAs)
- MOA: Block cysteinyl leukotriene (CysLT1) receptors → prevent bronchoconstriction, mucus secretion, and eosinophil recruitment triggered by leukotrienes (LTC4, LTD4, LTE4)
- Leukotrienes are major mediators in asthma and allergic rhinitis
| Drug | Notes |
|---|---|
| Montelukast (Singulair) | Most used; once daily oral; used in asthma + allergic rhinitis |
| Zafirlukast | Twice daily; CYP450 inhibitor |
| Zileuton | Inhibits 5-lipoxygenase (blocks leukotriene synthesis); hepatotoxicity risk |
V. CORTICOSTEROIDS
- MOA: Broad anti-inflammatory effect — suppress release of histamine, leukotrienes, prostaglandins, cytokines; reduce mast cell and eosinophil numbers
| Route | Drugs | Use |
|---|---|---|
| Inhaled | Budesonide, Fluticasone, Beclomethasone | Asthma, allergic rhinitis (nasal spray) |
| Topical | Hydrocortisone, Betamethasone | Allergic skin reactions (eczema, contact dermatitis) |
| Systemic (oral/IV) | Prednisolone, Dexamethasone, Methylprednisolone | Severe anaphylaxis, status asthmaticus, angioedema |
VI. EPINEPHRINE (ADRENALINE) — First-Line in Anaphylaxis
- MOA: α1 → vasoconstriction (reverses hypotension); β1 → ↑HR/cardiac output; β2 → bronchodilation; also inhibits further mast cell degranulation
- Route: IM (anterolateral thigh) — preferred; IV in cardiac arrest
- Device: EpiPen (auto-injector 0.3 mg for adults, 0.15 mg for children)
- Indications: Anaphylaxis, severe angioedema, laryngeal edema
VII. IMMUNOTHERAPY (Desensitization)
- MOA: Repeated allergen exposure → shift from Th2 → Th1 response; induces IgG4 "blocking" antibodies; reduces IgE production and mast cell sensitivity
- Routes: Subcutaneous (SCIT) or sublingual (SLIT)
- Use: Allergic rhinitis, bee venom allergy, food allergy (peanut — Palforzia)
- Only treatment that modifies the underlying allergic disease
VIII. BIOLOGICS (Newer Antiallergic Agents)
| Drug | Target | Use |
|---|---|---|
| Omalizumab (Xolair) | Anti-IgE (binds free IgE) | Moderate-severe allergic asthma, chronic urticaria |
| Dupilumab (Dupixent) | IL-4Rα (blocks IL-4 + IL-13 signaling) | Atopic dermatitis, asthma, eosinophilic esophagitis |
| Mepolizumab | Anti-IL-5 | Eosinophilic asthma |
| Benralizumab | Anti-IL-5Rα | Eosinophilic asthma |
| Tralokinumab | Anti-IL-13 | Atopic dermatitis |
QUICK SUMMARY TABLE
| Drug Class | MOA | Key Use |
|---|---|---|
| H1 blockers (1st gen) | H1 inverse agonist + anticholinergic | Allergy + sedation + motion sickness |
| H1 blockers (2nd gen) | H1 inverse agonist (no CNS) | Allergic rhinitis, urticaria |
| H2 blockers | H2 antagonist → ↓ acid | Adjunct anaphylaxis, GERD/ulcer |
| Mast cell stabilizers | Prevent mast cell degranulation | Prophylaxis — asthma, rhinitis |
| LTRAs | Block CysLT1 receptors | Asthma, allergic rhinitis |
| Corticosteroids | Broad anti-inflammatory | Anaphylaxis, asthma, dermatitis |
| Epinephrine | α1, β1, β2 agonist | First-line anaphylaxis |
| Biologics | Anti-IgE / anti-IL | Severe/refractory allergic disease |
MNEMONIC: 1st vs. 2nd Gen H1 Blockers
| 1st Gen | 2nd Gen | |
|---|---|---|
| BBB penetration | ✅ Yes | ❌ No |
| Sedation | ✅ Yes | ❌ No (or minimal) |
| Anticholinergic | ✅ Yes | ❌ No |
| Duration | Short (4–6 h) | Long (12–24 h) |
| Example | Diphenhydramine | Fexofenadine |
Sources: Lippincott Illustrated Reviews: Pharmacology — Katzung's Basic & Clinical Pharmacology, 16th Ed. — Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.