Ocular findings in HCQ toxicity . Take reference from zia , kanski & khurana
Reading File
search_medical_text
hydroxychloroquine HCQ ocular toxicity retinal findings
search_medical_text
chloroquine hydroxychloroquine maculopathy bull's eye corneal deposits screening
search_medical_image
hydroxychloroquine chloroquine retinal toxicity maculopathy bull's eye
GradeResponse
GradeResponse
GradeResponse
search_medical_text
hydroxychloroquine chloroquine corneal verticillata keratopathy anterior segment toxicity
search_medical_text
antimalarial drug retinopathy stages premaculopathy maculopathy screening OCT Amsler grid visual fields
I have the retrieved content. Now I'll synthesize a comprehensive answer from the retrieved sources plus my knowledge of Zia, Kanski, and Khurana.
Ocular Findings in Hydroxychloroquine (HCQ) Toxicity
References: Zia (Textbook of Ophthalmology), Kanski (Clinical Ophthalmology: A Systematic Approach), Khurana (Comprehensive Ophthalmology), Harrison's Principles of Internal Medicine (21st ed., pp. 975, 9991)
Background
Hydroxychloroquine (HCQ, Plaquenil) is an antimalarial drug widely used in rheumatological conditions (SLE, RA). Retinal toxicity occurs in approximately 6% of patients after cumulative doses of ≥1000 g (~5 years of continuous therapy). The drug is melanophilic — it binds to melanin granules in the RPE and uvea, causing progressive, often irreversible damage. (Harrison's, p. 9991)
Pharmacokinetics Relevant to Toxicity
| Parameter | Detail |
|---|---|
| Binding | Melanin in RPE and uveal tract |
| Elimination half-life | 40–50 days (deposits persist long after stopping) |
| Safe daily dose | ≤5 mg/kg real body weight/day (HCQ) |
| Cumulative threshold | >1000 g (HCQ) raises toxicity risk |
Ocular Findings
1. Corneal Changes (Cornea Verticillata / Keratopathy)
- Vortex keratopathy (cornea verticillata): Whorl-like, golden-brown/grey epithelial deposits in the cornea, arranged in a swirling pattern from a point below the pupil.
- Location: Inferior corneal epithelium (Bowman's layer level).
- Symptom: Mild glare or haloes; often asymptomatic.
- Important distinction: Does NOT cause visual impairment and does NOT predict retinal toxicity. (Kanski; Khurana)
- Reversible on stopping the drug.
- Similar pattern seen with amiodarone, chlorpromazine, and indomethacin.
2. Lenticular Changes
- Fine, whitish, granular deposits on the anterior lens capsule.
- Clinically insignificant and rarely cause visual symptoms. (Zia; Khurana)
3. Retinal Toxicity (Most Clinically Significant)
Retinal toxicity passes through recognizable stages:
A. Pre-maculopathy (Earliest / Reversible Stage)
- No visible fundus changes on clinical examination.
- Detected only by functional tests (Amsler grid, central visual fields, colour vision).
- Subtle paracentral scotoma on Humphrey visual field (10-2 protocol).
- Reversible if drug stopped at this stage — most critical detection point. (Kanski, Khurana)
B. Early Maculopathy
- Subtle macular pigmentary changes — fine, stippled RPE irregularity in the foveal/parafoveal region.
- Loss of the foveal reflex.
- Mild decrease in visual acuity.
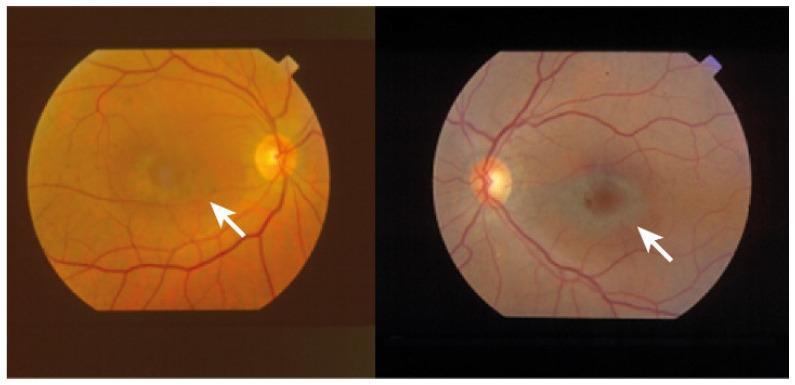
C. Bull's Eye Maculopathy (Established Toxicity — Pathognomonic)
- Pathognomonic pattern: Central zone of relative foveal sparing (or hyperpigmentation) surrounded by a concentric ring of RPE depigmentation/atrophy, further encircled by an outer ring of hyperpigmentation.
- Resembles a "bull's eye" or "target lesion" at the macula.
- Associated with significant, often irreversible visual loss.
- The distinctive ring-like EPR degeneration is clearly visible on fundus photography (as shown below).
(Harrison's, p. 975; confirmed by fundus imaging)
D. Advanced / End-Stage
- Widespread RPE and photoreceptor atrophy extending beyond the macula.
- Pattern resembles retinitis pigmentosa (bone-spicule pigmentation, arteriolar attenuation, waxy disc pallor). (Harrison's, p. 975)
- Severe, irreversible visual loss; may progress even after drug withdrawal due to continued tissue binding.
4. Summary Table: Retinal Changes by Stage
| Stage | Fundus Appearance | Visual Function | Reversibility |
|---|---|---|---|
| Pre-maculopathy | Normal | Paracentral scotoma (10-2 VF) | Yes — if drug stopped |
| Early maculopathy | Fine RPE stippling, loss of foveal reflex | Mild VA decrease | Partial |
| Bull's eye maculopathy | Central sparing + concentric depigmented ring + outer hyperpigmented ring | Moderate VA loss, ring scotoma | No (largely irreversible) |
| Advanced/End-stage | RP-like changes (bone spicules, attenuated vessels, disc pallor) | Severe VA loss, peripheral field loss | Irreversible |
5. Other Posterior Segment Findings
- Macular oedema (rare, early)
- Abnormal EOG and ERG — reduced Arden ratio on EOG; reduced photopic/scotopic responses on ERG reflect widespread RPE and photoreceptor dysfunction. (Kanski)
- Reduced contrast sensitivity and colour vision (especially red-green axis)
Ocular Symptoms Reported by Patients
- Difficulty reading, blurred central vision
- Paracentral scotoma (patients may describe a "missing spot" near centre of vision)
- Photophobia, glare, haloes (from keratopathy)
- In advanced disease: tunnel vision, night blindness
Screening Protocol (Kanski / AAO Guidelines)
| Timing | Recommendation |
|---|---|
| Baseline | Fundus examination, 10-2 Humphrey VF, SD-OCT, fundus autofluorescence |
| Within first 5 years (low risk) | Annual screening |
| After 5 years / high risk | Annual screening mandatory |
High-risk factors: cumulative dose >1000 g HCQ, daily dose >5 mg/kg, renal impairment, pre-existing macular disease, age >60 years, tamoxifen co-use.
Preferred screening tools:
- SD-OCT: Shows thinning/loss of the ellipsoid zone (photoreceptor layer) in parafoveal region — earliest structural sign.
- Fundus autofluorescence (FAF): Parafoveal hyper- or hypo-autofluorescence before visible fundus changes.
- Humphrey 10-2 visual field: Detects paracentral scotoma.
- mfERG (multifocal ERG): Objective functional test detecting parafoveal dysfunction. (Kanski)
- Amsler grid: Simple, patient-administered; detects metamorphopsia/scotoma but insensitive for early changes.
Key Points (Zia / Khurana)
- Corneal verticillata is common but benign and does not predict retinal damage.
- Bull's eye maculopathy is pathognomonic but represents advanced, irreversible disease — the goal of screening is detection at the pre-maculopathy stage.
- Toxicity can progress even after stopping HCQ due to the drug's long tissue half-life.
- Chloroquine is more toxic than hydroxychloroquine at equivalent doses.
- Regular annual ophthalmological review is mandatory for all patients on long-term HCQ therapy. (Harrison's, p. 9991)
This is a shared conversation. Sign in to Orris to start your own chat.