
IMG20260625201350.jpg
Black spot on forhead. Itching after sun exposure
analyse_media
Reading File
Finding Sources
Searching the Web
dark grey brown patch forehead itching after sun exposure melasma vs solar lentigo differential diagnosis
Reading File
Reading File
Loading Image
Reading File
I now have enough information to give a thorough answer. Here is a full assessment:
Assessment: Dark Patch on Forehead with Sun-Induced Itching
Important disclaimer: This is an educational overview only. A dermatologist should examine this in person - they may use a Wood's lamp or dermoscopy for a definitive diagnosis.
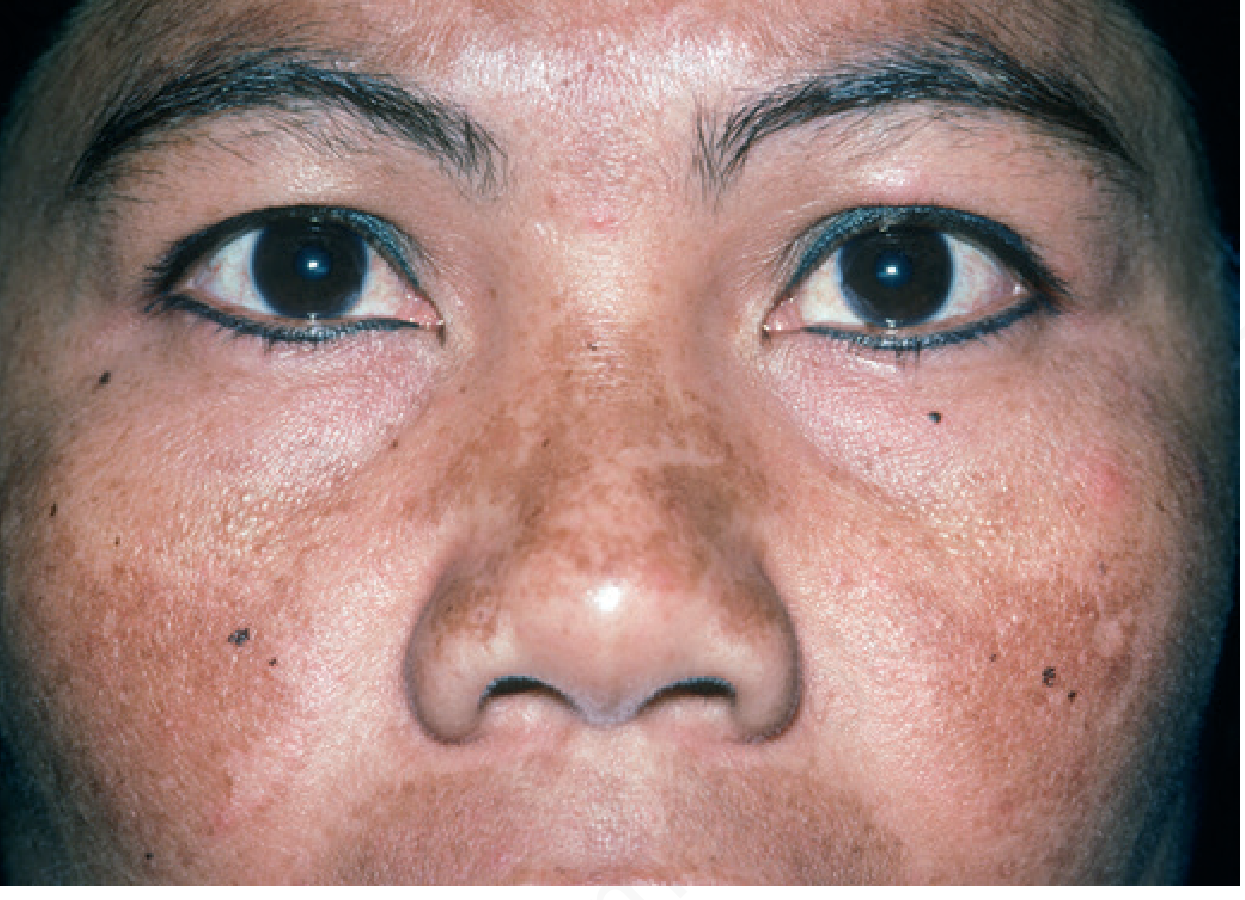
What the image shows
The patch on the right forehead (above the medial eyebrow) is:
- ~1.5 cm wide, oval/horizontally oriented
- Flat (macular) - no raised edges, no scaling, no ulceration
- Dusky grey-brown color with ill-defined, fading borders
- Uneven pigmentation, slightly darker in the center
There are also mild periorbital dark circles and a few small spots on the cheek consistent with minor post-inflammatory hyperpigmentation or acne marks.
Most Likely Diagnosis: Melasma
This presentation is highly characteristic of melasma (also called chloasma). Compare with the textbook photograph from Andrews' Diseases of the Skin:
Key features matching melasma in this case:
| Feature | This patient | Melasma |
|---|---|---|
| Location | Forehead | Forehead is classic (centrofacial pattern) |
| Color | Dusky grey-brown | Tan to dark brown, sometimes grey |
| Border | Ill-defined, fading | Usually somewhat ill-defined |
| Texture | Flat macule | Flat patch |
| Trigger | Worse after sun | Sun exposure is the primary trigger |
| Itching | Present | Occasionally reported, especially post-sun |
| Skin type | Darker complexion | Strongly associated with Fitzpatrick IV-V |
From Andrews' Diseases of the Skin: "Melasma is a common disorder, with two predisposing factors: sun exposure and sex hormones. It tends to affect darker-complexioned individuals, especially East, West, and Southeast Asians... Melasma is characterized by brown patches, typically on the malar prominences and forehead."
Why the Itching After Sun Exposure?
Melasma-affected skin has a lower minimal erythema dose (MED) - it reacts to UV more readily than surrounding skin. After sun exposure, the UV-triggered melanogenesis and local inflammatory response can cause itching/irritation, especially in dermal melasma where melanophages accumulate.
Other Possibilities to Rule Out
| Condition | Why less likely here |
|---|---|
| Solar lentigo | Usually smaller, well-defined, discrete; does NOT cause itching |
| Ephelides (freckles) | Smaller, multiple; fade in winter |
| Lichen planus pigmentosus | More violaceous, often periorbital |
| Nevus of Ota | Usually unilateral scleral involvement; congenital |
| Post-inflammatory hyperpigmentation | Follows prior skin injury/acne |
What to Do
See a dermatologist - they will confirm with Wood's lamp examination (epidermal melasma brightens under UV; dermal does not) and may do dermoscopy.
In the meantime:
- Broad-spectrum sunscreen (SPF 30+, UVA+UVB) every day - this is the single most important step; it both reduces worsening and makes any treatment more effective
- Avoid peak sun hours (10 AM - 4 PM) and use hats/physical protection
- Do not scratch - itching after sun exposure is the skin reacting to UV; scratching can worsen pigmentation via post-inflammatory hyperpigmentation
Treatments a dermatologist may offer:
- Topical hydroquinone (2-4%) - gold standard bleaching agent
- Tretinoin (topical retinoid) - enhances hydroquinone efficacy
- Kligman's formula (hydroquinone + tretinoin + mild corticosteroid) - most effective topical regimen
- Tranexamic acid - newer option with good evidence
- Chemical peels or laser - used cautiously, as they can sometimes worsen pigmentation in darker skin types
Bottom line: This is very likely melasma triggered and worsened by sun exposure. It is benign and not dangerous, but does require consistent sun protection and dermatologist-guided treatment for improvement. The itching after sun exposure is a recognized feature reflecting UV sensitivity of affected skin.
This is from last two years
The 2-year duration actually strengthens the melasma diagnosis. Here's why that matters:
Duration Confirms Melasma
Melasma is a chronic condition - it does not resolve on its own without treatment and sun protection. A slowly developing, persistent grey-brown forehead patch over 2 years that worsens with sun is the textbook course.
Key points given this timeline:
- It has not grown rapidly, changed shape, or ulcerated - this rules out anything sinister (melanoma, pigmented BCC)
- 2 years of UV accumulation means the pigment may now be both epidermal AND dermal (mixed type), which is harder to treat
- The longer it goes untreated, the deeper the pigment deposits - dermal melanin responds poorly to topical creams alone
What the 2-Year History Tells a Dermatologist
| Question to ask | Why it matters |
|---|---|
| Did it start around a hormonal change (puberty, pill, pregnancy)? | Hormones are the 2nd biggest melasma trigger after sun |
| Does it fade slightly in winter/indoors? | Epidermal melasma fades when UV is avoided; dermal does not |
| Any family history of similar patches? | Genetic predisposition is common |
| Any medications (phenytoin, OCP)? | Several drugs can trigger melasma |
Why You Should Not Wait Further
Two years is long enough that:
- Topical creams alone may not fully clear it - dermal pigment needs professional treatment
- Sun damage is cumulative - without sunscreen, it deepens every summer
- A dermatologist can do a Wood's lamp test in 30 seconds to determine if the pigment is epidermal (more treatable) or dermal (needs laser/peels)
Immediate Step Right Now
Start a broad-spectrum SPF 50 sunscreen on that area every morning - even before seeing a doctor. This stops further deepening. Two years of untreated melasma can still respond well to treatment if sun protection is started now and maintained strictly.
See a dermatologist for Wood's lamp examination and a proper treatment plan (hydroquinone, tretinoin, or Kligman's triple formula).
History 20-year-old female. Present for about 2 years. Started as a tiny dark dot, enlarged gradually, then stopped growing. Initially itchy; now itching occurs mainly after sun exposure. Similar lesion on the hand. No other symptoms.
Finding Sources
Finding Sources
Searching the Web
solitary dark spot started small enlarged stopped growing itchy after sun exposure hand and forehead young female differential diagnosis dermatology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
mastocytoma adult forehead hand dark brown macule started small enlarged stopped growing itchy heat sun Darier sign
This history points strongly in one direction. Here is the revised, complete analysis:
Revised Differential - The History Changes Everything
The combination of:
- Started as a tiny dark dot → enlarged gradually → stopped growing
- Initially itchy all the time → now mainly after sun/heat exposure
- Similar lesion also on the hand
- Flat, dusky grey-brown, ill-defined patch
- 20-year-old female
...no longer fits melasma well. This pattern fits cutaneous mastocytosis / solitary mastocytoma (urticaria pigmentosa) much better, and a melanocytic nevus (junctional/compound) must also be considered.
Top Diagnosis: Cutaneous Mastocytosis (Urticaria Pigmentosa / Solitary Mastocytoma)
This is the most compelling fit given the full history.
Why it fits so well:
| Feature | This patient | Mastocytosis |
|---|---|---|
| Lesion started as tiny dark dot, enlarged, then stopped | ✅ | Classic growth pattern of mastocytoma |
| Itchy - initially constant, now triggered by sun/heat | ✅ | Pathognomonic - mast cell mediators released by heat, UV, friction |
| Two lesions: forehead AND hand | ✅ | Mastocytomas favor the dorsum of the hand (classic site per textbook) |
| Grey-brown flat macular patch | ✅ | Chamois/slate-brown macules are typical |
| Lesion stable (not growing for some time) | ✅ | Mastocytomas enlarge then stabilize |
From Andrews' Diseases of the Skin: "It originates as a brown macule that urticates on stroking... Although the mastocytoma may occur anywhere on the body, it favors the dorsum of the hand near the wrist."
From Merck Manual: "Skin involvement is often pruritic in mastocytosis... The following may worsen itching: changes in temperature, contact with clothing, hot beverages, exercising - and UV/sun exposure."
The Key Diagnostic Test - Darier's Sign
Firmly stroke or rub the lesion with a blunt object (pen cap, wooden spatula). Wait 3-5 minutes.
- Positive (diagnostic): The lesion becomes red, swollen, urticarial (hive-like) - this is mast cell mediator release and is considered near-pathognomonic for mastocytosis
- Positive in ~50% of solitary mastocytomas, ~90% of generalized forms
- If positive, it strongly confirms cutaneous mastocytosis
Second Diagnosis: Junctional / Compound Melanocytic Nevus (Mole)
A nevus can also:
- Start as a small dot and slowly enlarge then stabilize
- Appear on both face and hand
- Be flat, brown-grey colored
- Itch mildly (especially if irritated by sun)
However, itching specifically triggered by sun/heat is far less characteristic of a simple nevus - this is more specific to mast cell disease.
Revised Differential Diagnosis Table
| Diagnosis | Fits | Against |
|---|---|---|
| Cutaneous mastocytosis / mastocytoma | Started small → grew → stopped; itch triggered by sun/heat; hand lesion (classic site); grey-brown macule | Usually presents in childhood; 20-year-old onset is less common but described |
| Junctional melanocytic nevus | Started small, enlarged slowly, stabilized; face + hand | Itching specifically with sun less typical |
| Melasma | Forehead location; sun-worsened | Does NOT start as a dot and enlarge; not typically on hands; no dot-to-patch evolution |
| Solar lentigo | Sun-exposed site | Does NOT itch; onset at 20 unusual without heavy UV history |
| Fixed drug eruption | Pigmented macule, recurs same site | No drug history given; doesn't grow progressively |
What the Dermatologist Should Do
- Darier's sign test - rub the lesion firmly, wait 5 min. If it urticates → cutaneous mastocytosis confirmed clinically
- Dermoscopy - look for mast cell aggregates vs nevus pattern
- Skin biopsy if Darier's sign equivocal - histology shows mast cell aggregates, positive CD117 (c-Kit) and tryptase staining
- Serum tryptase - if elevated (>20 ng/mL), rule out systemic mastocytosis
- Check the hand lesion - if it also has a positive Darier's sign, diagnosis is almost certain
Management if Mastocytosis Confirmed
- Avoid triggers: heat, sun, friction, alcohol, NSAIDs, hot drinks
- Oral antihistamines (H1 blockers like cetirizine/loratadine) - control itching
- Topical corticosteroids (potent) under occlusion - can reduce mast cell density
- Solitary mastocytomas that are bothersome can be excised
- At 20 years old, adult-onset cutaneous mastocytosis tends to persist (unlike childhood type which involutes) - so proper workup and management is important
- Reassurance: cutaneous-only disease rarely progresses to systemic mastocytosis
Bottom line: The history of "started as a dot, enlarged, then stopped; initially constantly itchy, now itchy only with sun/heat; similar lesion on the hand" is a near-classic presentation of cutaneous mastocytosis. The Darier's sign test at the dermatology visit will likely confirm this. Please see a dermatologist promptly for this test and possible biopsy.
This is a shared conversation. Sign in to Orris to start your own chat.