MASTER PROMPT TEMPLATE ✨ Create a clean high-yield medical infographic poster for medical students preparing for neet pg about: CARDIOVASCULAR SYSTEM Style: modern medical infographic highly organized exam-focused visually memorable colorful but professional easy to review before exams include emojis/icons for memory aid use clear section boxes and arrows use concise bullet points use tables for comparisons use color-coded categories include important high-yield notes and warning signs make it aesthetically pleasing like premium study notes white background readable font structured like a study cheat sheet Must include: Definition Classification Causes / risk factors Pathophysiology Clinical features Diagnosis Management Complications Important investigations High-yield exam pearls Memory tricks / mnemonics Comparison tables if applicable
mkdir -p /tmp/workspace/heart-failure-poster && ls /tmp/workspace/
~/heart-failure-poster/heart_failure_poster.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<meta name="viewport" content="width=device-width, initial-scale=1.0">
<title>Heart Failure – NEET PG High-Yield Infographic</title>
<style>
@import url('https://fonts.googleapis.com/css2?family=Inter:wght@300;400;500;600;700;800;900&family=Poppins:wght@400;600;700;800&display=swap');
* { margin: 0; padding: 0; box-sizing: border-box; }
body {
font-family: 'Inter', sans-serif;
background: #f5f5f5;
color: #1a1a2e;
font-size: 11px;
line-height: 1.5;
}
.page {
width: 1200px;
margin: 0 auto;
background: #ffffff;
padding: 20px 24px 28px;
}
/* ─── HEADER ─── */
.header {
background: linear-gradient(135deg, #1a1a5e 0%, #16213e 40%, #0f3460 80%, #533483 100%);
border-radius: 16px;
padding: 20px 28px;
display: flex;
align-items: center;
justify-content: space-between;
margin-bottom: 18px;
box-shadow: 0 6px 24px rgba(26,26,94,0.25);
}
.header-left h1 {
font-family: 'Poppins', sans-serif;
font-size: 32px;
font-weight: 800;
color: #fff;
letter-spacing: -0.5px;
}
.header-left h1 span { color: #f9ca24; }
.header-left p {
font-size: 12px;
color: #a8d8ea;
margin-top: 4px;
font-weight: 500;
}
.header-badges {
display: flex;
gap: 8px;
flex-wrap: wrap;
justify-content: flex-end;
}
.badge {
background: rgba(255,255,255,0.15);
color: #fff;
border: 1px solid rgba(255,255,255,0.3);
border-radius: 20px;
padding: 4px 12px;
font-size: 10px;
font-weight: 600;
backdrop-filter: blur(4px);
}
.badge.hot { background: rgba(249,202,36,0.25); border-color: #f9ca24; color: #f9ca24; }
/* ─── GRID ─── */
.grid-3 { display: grid; grid-template-columns: 1fr 1fr 1fr; gap: 14px; margin-bottom: 14px; }
.grid-2 { display: grid; grid-template-columns: 1fr 1fr; gap: 14px; margin-bottom: 14px; }
.grid-2-1 { display: grid; grid-template-columns: 2fr 1fr; gap: 14px; margin-bottom: 14px; }
.grid-1-2 { display: grid; grid-template-columns: 1fr 2fr; gap: 14px; margin-bottom: 14px; }
.grid-full { margin-bottom: 14px; }
.span-2 { grid-column: span 2; }
/* ─── CARDS ─── */
.card {
border-radius: 12px;
padding: 14px 16px;
border: 1.5px solid transparent;
position: relative;
overflow: hidden;
}
.card::before {
content: '';
position: absolute;
top: 0; left: 0;
width: 4px;
height: 100%;
border-radius: 12px 0 0 12px;
}
.card-blue { background: #eff6ff; border-color: #bfdbfe; } .card-blue::before { background: #2563eb; }
.card-green { background: #f0fdf4; border-color: #bbf7d0; } .card-green::before { background: #16a34a; }
.card-red { background: #fff1f2; border-color: #fecdd3; } .card-red::before { background: #dc2626; }
.card-purple { background: #faf5ff; border-color: #e9d5ff; } .card-purple::before { background: #7c3aed; }
.card-orange { background: #fff7ed; border-color: #fed7aa; } .card-orange::before { background: #ea580c; }
.card-teal { background: #f0fdfa; border-color: #99f6e4; } .card-teal::before { background: #0d9488; }
.card-yellow { background: #fefce8; border-color: #fde68a; } .card-yellow::before { background: #ca8a04; }
.card-pink { background: #fdf2f8; border-color: #f9a8d4; } .card-pink::before { background: #db2777; }
.card-indigo { background: #eef2ff; border-color: #c7d2fe; } .card-indigo::before { background: #4f46e5; }
.card-dark { background: #1e293b; border-color: #334155; color: #f8fafc; }
.card-dark::before { background: #f9ca24; }
/* ─── SECTION TITLES ─── */
.section-title {
font-family: 'Poppins', sans-serif;
font-size: 11.5px;
font-weight: 700;
margin-bottom: 8px;
display: flex;
align-items: center;
gap: 6px;
text-transform: uppercase;
letter-spacing: 0.5px;
}
.section-title .icon { font-size: 14px; }
.card-blue .section-title { color: #1d4ed8; }
.card-green .section-title { color: #15803d; }
.card-red .section-title { color: #b91c1c; }
.card-purple .section-title { color: #6d28d9; }
.card-orange .section-title { color: #c2410c; }
.card-teal .section-title { color: #0f766e; }
.card-yellow .section-title { color: #92400e; }
.card-pink .section-title { color: #be185d; }
.card-indigo .section-title { color: #3730a3; }
.card-dark .section-title { color: #f9ca24; }
/* ─── LISTS ─── */
ul.dot-list { list-style: none; padding: 0; }
ul.dot-list li {
padding: 2px 0 2px 14px;
position: relative;
font-size: 10.5px;
color: #374151;
}
ul.dot-list li::before {
content: '▸';
position: absolute;
left: 0;
color: #6b7280;
font-size: 9px;
top: 3px;
}
.card-dark ul.dot-list li { color: #e2e8f0; }
.card-dark ul.dot-list li::before { color: #f9ca24; }
/* ─── TABLES ─── */
table.info-table {
width: 100%;
border-collapse: collapse;
font-size: 10px;
margin-top: 4px;
}
table.info-table th {
padding: 5px 8px;
font-weight: 700;
text-align: left;
font-size: 9.5px;
text-transform: uppercase;
letter-spacing: 0.3px;
}
table.info-table td {
padding: 4px 8px;
border-bottom: 1px solid rgba(0,0,0,0.05);
vertical-align: top;
line-height: 1.4;
}
table.info-table tr:last-child td { border-bottom: none; }
.th-blue { background: #dbeafe; color: #1e3a8a; }
.th-green { background: #dcfce7; color: #14532d; }
.th-red { background: #fee2e2; color: #7f1d1d; }
.th-purple { background: #ede9fe; color: #4c1d95; }
.th-orange { background: #fed7aa; color: #7c2d12; }
.th-teal { background: #ccfbf1; color: #134e4a; }
.th-dark { background: #334155; color: #f8fafc; }
.tr-alt:nth-child(even) td { background: rgba(0,0,0,0.025); }
/* ─── TAGS/PILLS ─── */
.pill {
display: inline-block;
padding: 2px 9px;
border-radius: 20px;
font-size: 9.5px;
font-weight: 700;
margin: 2px 2px;
}
.pill-red { background: #fee2e2; color: #b91c1c; border: 1px solid #fca5a5; }
.pill-blue { background: #dbeafe; color: #1d4ed8; border: 1px solid #93c5fd; }
.pill-green { background: #dcfce7; color: #15803d; border: 1px solid #86efac; }
.pill-orange { background: #ffedd5; color: #c2410c; border: 1px solid #fb923c; }
.pill-purple { background: #ede9fe; color: #6d28d9; border: 1px solid #c4b5fd; }
.pill-teal { background: #ccfbf1; color: #0f766e; border: 1px solid #5eead4; }
.pill-yellow { background: #fef3c7; color: #92400e; border: 1px solid #fcd34d; }
.pill-pink { background: #fce7f3; color: #be185d; border: 1px solid #f9a8d4; }
/* ─── HIGHLIGHT BOXES ─── */
.highlight-box {
border-radius: 8px;
padding: 8px 12px;
margin-top: 8px;
font-size: 10px;
font-weight: 600;
display: flex;
align-items: flex-start;
gap: 6px;
}
.hb-red { background: #fef2f2; border: 1.5px solid #ef4444; color: #b91c1c; }
.hb-yellow { background: #fefce8; border: 1.5px solid #eab308; color: #713f12; }
.hb-blue { background: #eff6ff; border: 1.5px solid #3b82f6; color: #1e3a8a; }
.hb-green { background: #f0fdf4; border: 1.5px solid #22c55e; color: #14532d; }
.warn-icon { font-size: 13px; flex-shrink: 0; margin-top: 1px; }
/* ─── MNEMONIC BOXES ─── */
.mnemonic {
background: linear-gradient(135deg, #1e293b, #0f172a);
border-radius: 10px;
padding: 10px 14px;
margin-top: 8px;
color: #f8fafc;
}
.mnemonic .title {
font-family: 'Poppins', sans-serif;
font-size: 10px;
font-weight: 700;
color: #f9ca24;
text-transform: uppercase;
letter-spacing: 0.5px;
margin-bottom: 6px;
}
.mnemonic .letters { display: flex; flex-wrap: wrap; gap: 4px; }
.mnemonic .letter-block {
background: rgba(255,255,255,0.08);
border: 1px solid rgba(249,202,36,0.3);
border-radius: 6px;
padding: 4px 8px;
font-size: 10px;
}
.mnemonic .letter-block strong { color: #f9ca24; font-size: 13px; display: block; }
/* ─── FLOWCHART ─── */
.flow {
display: flex;
align-items: center;
gap: 4px;
flex-wrap: wrap;
margin: 6px 0;
}
.flow-box {
background: #fff;
border: 1.5px solid currentColor;
border-radius: 8px;
padding: 4px 10px;
font-size: 9.5px;
font-weight: 600;
text-align: center;
}
.flow-arrow { font-size: 14px; color: #6b7280; }
/* ─── DRUG TABLE ─── */
.drug-tag {
display: inline-block;
background: #1e40af;
color: #fff;
border-radius: 4px;
padding: 1px 7px;
font-size: 9px;
font-weight: 700;
margin: 1px;
}
/* ─── PEARL BOX ─── */
.pearl {
background: linear-gradient(135deg, #f0fdf4, #dcfce7);
border: 2px solid #16a34a;
border-radius: 10px;
padding: 8px 12px;
margin-top: 6px;
position: relative;
}
.pearl::before {
content: '💎';
position: absolute;
top: -10px;
left: 10px;
font-size: 16px;
}
.pearl p { font-size: 10px; color: #14532d; line-height: 1.5; }
.pearl p strong { color: #166534; }
/* ─── FOOTER ─── */
.footer {
background: #1e293b;
border-radius: 10px;
padding: 10px 20px;
display: flex;
justify-content: space-between;
align-items: center;
margin-top: 14px;
}
.footer p { color: #94a3b8; font-size: 9.5px; }
.footer strong { color: #f9ca24; }
/* ─── DIVIDER ─── */
.divider {
height: 3px;
background: linear-gradient(90deg, #2563eb, #7c3aed, #db2777, #ea580c, #16a34a);
border-radius: 2px;
margin: 14px 0;
}
/* ─── NUMBERED STEPS ─── */
.step {
display: flex;
gap: 8px;
align-items: flex-start;
padding: 4px 0;
}
.step-num {
width: 18px;
height: 18px;
border-radius: 50%;
display: flex;
align-items: center;
justify-content: center;
font-size: 9px;
font-weight: 800;
flex-shrink: 0;
}
.step-text { font-size: 10px; color: #374151; flex: 1; }
.sn-blue { background: #2563eb; color: #fff; }
.sn-green { background: #16a34a; color: #fff; }
.sn-orange { background: #ea580c; color: #fff; }
.sn-purple { background: #7c3aed; color: #fff; }
.sn-red { background: #dc2626; color: #fff; }
strong.accent { color: #2563eb; }
strong.red { color: #dc2626; }
strong.green { color: #16a34a; }
strong.purple { color: #7c3aed; }
strong.orange { color: #ea580c; }
.sub-head {
font-size: 10px;
font-weight: 700;
color: inherit;
margin: 6px 0 3px;
text-transform: uppercase;
letter-spacing: 0.3px;
opacity: 0.8;
}
</style>
</head>
<body>
<div class="page">
<!-- ══════════ HEADER ══════════ -->
<div class="header">
<div class="header-left">
<h1>💓 <span>HEART FAILURE</span> — High-Yield Master Sheet</h1>
<p>CARDIOVASCULAR SYSTEM | NEET PG / USMLE / MD Entrance | Based on Braunwald's, Goldman-Cecil, Goodman & Gilman's</p>
</div>
<div class="header-badges">
<span class="badge hot">🔥 HIGH YIELD</span>
<span class="badge">📚 Braunwald's</span>
<span class="badge">📖 Goldman-Cecil</span>
<span class="badge">💊 Goodman & Gilman</span>
</div>
</div>
<!-- ══════════ ROW 1: Definition + Classification ══════════ -->
<div class="grid-2">
<!-- DEFINITION -->
<div class="card card-blue">
<div class="section-title"><span class="icon">📘</span> Definition</div>
<ul class="dot-list">
<li>Heart failure = clinical syndrome in which the heart <strong>cannot pump sufficient blood</strong> to meet the body's metabolic demands, OR can do so only at <strong>elevated filling pressures</strong></li>
<li>Not a diagnosis itself — it is the <strong>end result</strong> of many cardiac diseases</li>
<li>Affects ~26 million people worldwide; leading cause of hospitalization in adults >65 years</li>
</ul>
<div class="highlight-box hb-blue">
<span class="warn-icon">💡</span>
<span><strong>Key concept:</strong> Cardiac output may be normal at rest but fails to increase with exertion → exercise intolerance is the hallmark symptom</span>
</div>
</div>
<!-- CLASSIFICATION BY EF -->
<div class="card card-purple">
<div class="section-title"><span class="icon">📊</span> Classification by Ejection Fraction</div>
<table class="info-table">
<thead>
<tr><th class="th-purple">Type</th><th class="th-purple">EF</th><th class="th-purple">Mechanism</th><th class="th-purple">Key Feature</th></tr>
</thead>
<tbody class="tr-alt">
<tr><td><strong>HFrEF</strong><br><span style="font-size:9px;color:#6b7280">Reduced</span></td><td style="color:#b91c1c;font-weight:700">< 40%</td><td>Systolic dysfunction; ↓ contractility</td><td>Dilated LV; most evidence-based drugs</td></tr>
<tr><td><strong>HFmrEF</strong><br><span style="font-size:9px;color:#6b7280">Mildly Reduced</span></td><td style="color:#d97706;font-weight:700">40–49%</td><td>Mixed systolic + diastolic</td><td>"Grey zone" — emerging therapies</td></tr>
<tr><td><strong>HFpEF</strong><br><span style="font-size:9px;color:#6b7280">Preserved</span></td><td style="color:#16a34a;font-weight:700">≥ 50%</td><td>Diastolic dysfunction; ↑ stiffness</td><td>Older women, HTN, DM; same mortality as HFrEF</td></tr>
</tbody>
</table>
<div class="highlight-box hb-yellow">
<span class="warn-icon">⚠️</span>
<span>HFpEF mortality = HFrEF mortality. Hospitalization rates are comparable regardless of EF. (Goldman-Cecil)</span>
</div>
</div>
</div>
<!-- ══════════ ROW 2: NYHA + ACC/AHA Staging ══════════ -->
<div class="grid-2">
<!-- NYHA CLASSIFICATION -->
<div class="card card-orange">
<div class="section-title"><span class="icon">🏃</span> NYHA Functional Classification</div>
<table class="info-table">
<thead>
<tr><th class="th-orange">Class</th><th class="th-orange">Symptoms</th><th class="th-orange">Activity</th></tr>
</thead>
<tbody class="tr-alt">
<tr><td><span class="pill pill-green">Class I</span></td><td>No symptoms</td><td>Ordinary activity — no limitation</td></tr>
<tr><td><span class="pill pill-blue">Class II</span></td><td>Mild symptoms</td><td>Slight limitation; comfortable at rest</td></tr>
<tr><td><span class="pill pill-orange">Class III</span></td><td>Moderate symptoms</td><td>Marked limitation; comfortable only at rest</td></tr>
<tr><td><span class="pill pill-red">Class IV</span></td><td>Severe symptoms</td><td>Symptoms at rest; any activity causes discomfort</td></tr>
</tbody>
</table>
</div>
<!-- ACC/AHA STAGING -->
<div class="card card-teal">
<div class="section-title"><span class="icon">📈</span> ACC/AHA Staging (2022 Guidelines)</div>
<table class="info-table">
<thead>
<tr><th class="th-teal">Stage</th><th class="th-teal">Description</th><th class="th-teal">Intervention</th></tr>
</thead>
<tbody class="tr-alt">
<tr><td><span class="pill pill-green">A</span></td><td>At risk — no structural disease, no symptoms</td><td>Modify risk factors (HTN, DM, obesity)</td></tr>
<tr><td><span class="pill pill-blue">B</span></td><td>Pre-HF — structural disease, no symptoms</td><td>Treat structural heart disease</td></tr>
<tr><td><span class="pill pill-orange">C</span></td><td>Symptomatic HF — structural disease + symptoms</td><td>Reduce morbidity & mortality</td></tr>
<tr><td><span class="pill pill-red">D</span></td><td>Advanced/Refractory HF — despite optimal therapy</td><td>Mechanical support, transplant, palliation</td></tr>
</tbody>
</table>
<div class="highlight-box hb-blue">
<span class="warn-icon">💡</span>
<span>Stages are <strong>progressive and not reversible</strong> (unlike NYHA which is dynamic). ACC/AHA staging predicts prognosis.</span>
</div>
</div>
</div>
<div class="divider"></div>
<!-- ══════════ ROW 3: Causes + Pathophysiology ══════════ -->
<div class="grid-2">
<!-- CAUSES -->
<div class="card card-red">
<div class="section-title"><span class="icon">🔎</span> Causes / Etiology</div>
<div class="sub-head">Most Common (>70% in developed world)</div>
<ul class="dot-list">
<li>🫀 <strong>Coronary artery disease</strong> / prior MI (most common — ~70%)</li>
<li>🩺 <strong>Hypertension</strong> — pressure overload → LVH → HFpEF</li>
<li>🍬 <strong>Diabetes mellitus</strong> — diabetic cardiomyopathy</li>
<li>⚖️ <strong>Obesity</strong> — increased preload and afterload</li>
</ul>
<div class="sub-head" style="margin-top:8px">Other Causes (Remember CARDIAC)</div>
<div style="display:flex; flex-wrap:wrap; gap:4px; margin-top:4px;">
<span class="pill pill-red">Cardiomyopathy (DCM/HCM)</span>
<span class="pill pill-orange">Arrhythmias (AF, tachycardia-mediated)</span>
<span class="pill pill-blue">Rheumatic / Valvular disease</span>
<span class="pill pill-purple">Drugs (alcohol, anthracyclines)</span>
<span class="pill pill-teal">Infections (viral myocarditis)</span>
<span class="pill pill-pink">Amyloidosis / Infiltrative</span>
<span class="pill pill-green">Congenital Heart Disease</span>
<span class="pill pill-yellow">Thyroid disease</span>
</div>
</div>
<!-- PATHOPHYSIOLOGY -->
<div class="card card-indigo">
<div class="section-title"><span class="icon">⚙️</span> Pathophysiology — 4 Interrelated Systems</div>
<div class="flow" style="margin-bottom:8px;">
<div class="flow-box" style="color:#2563eb; background:#eff6ff;">Cardiac Injury / Overload</div>
<div class="flow-arrow">→</div>
<div class="flow-box" style="color:#7c3aed; background:#faf5ff;">↓ Cardiac Output</div>
<div class="flow-arrow">→</div>
<div class="flow-box" style="color:#dc2626; background:#fff1f2;">Compensatory Activation</div>
<div class="flow-arrow">→</div>
<div class="flow-box" style="color:#b91c1c; background:#fee2e2;">Pathological Remodeling</div>
</div>
<table class="info-table">
<thead>
<tr><th class="th-purple">System</th><th class="th-purple">Mechanism</th><th class="th-purple">Net Effect</th></tr>
</thead>
<tbody class="tr-alt">
<tr><td>❤️ <strong>Heart</strong></td><td>Hypertrophy → fibrosis → apoptosis → remodeling</td><td>↓ contractility, arrhythmias</td></tr>
<tr><td>🩸 <strong>Vasculature</strong></td><td>↑ afterload (stiffness), endothelial dysfunction</td><td>↑ wall stress, ↑ O₂ demand</td></tr>
<tr><td>🫘 <strong>Kidney</strong></td><td>↓ renal perfusion → ↑ RAAS → Na⁺/H₂O retention</td><td>Volume overload → congestion</td></tr>
<tr><td>🧠 <strong>Neurohormonal</strong></td><td>↑ SNS, ↑ RAAS, ↑ ADH, ↑ Endothelin</td><td>Initially beneficial → long-term harmful</td></tr>
</tbody>
</table>
<div class="highlight-box hb-blue">
<span class="warn-icon">💡</span>
<span><strong>KEY PEARL:</strong> Pathological hypertrophy → ↓ capillary/myocyte ratio → energy deficit → altered gene expression → fibrosis → heart failure (Goodman & Gilman)</span>
</div>
</div>
</div>
<!-- ══════════ ROW 4: Left vs Right HF ══════════ -->
<div class="grid-full">
<div class="card card-pink">
<div class="section-title"><span class="icon">↔️</span> Left-Sided vs Right-Sided Heart Failure — Comparison Table</div>
<table class="info-table">
<thead>
<tr><th class="th-red" style="width:18%">Feature</th><th class="th-red">LEFT Heart Failure (LHF)</th><th style="background:#fce7f3;color:#9d174d;">RIGHT Heart Failure (RHF)</th></tr>
</thead>
<tbody class="tr-alt">
<tr><td><strong>Common Cause</strong></td><td>MI, HTN, AS, MR, DCM</td><td>LHF (most common), COPD, Pulmonary HTN, RV MI</td></tr>
<tr><td><strong>Congestion</strong></td><td>🫁 Pulmonary — lungs, bronchi</td><td>🫁 Systemic — liver, gut, limbs</td></tr>
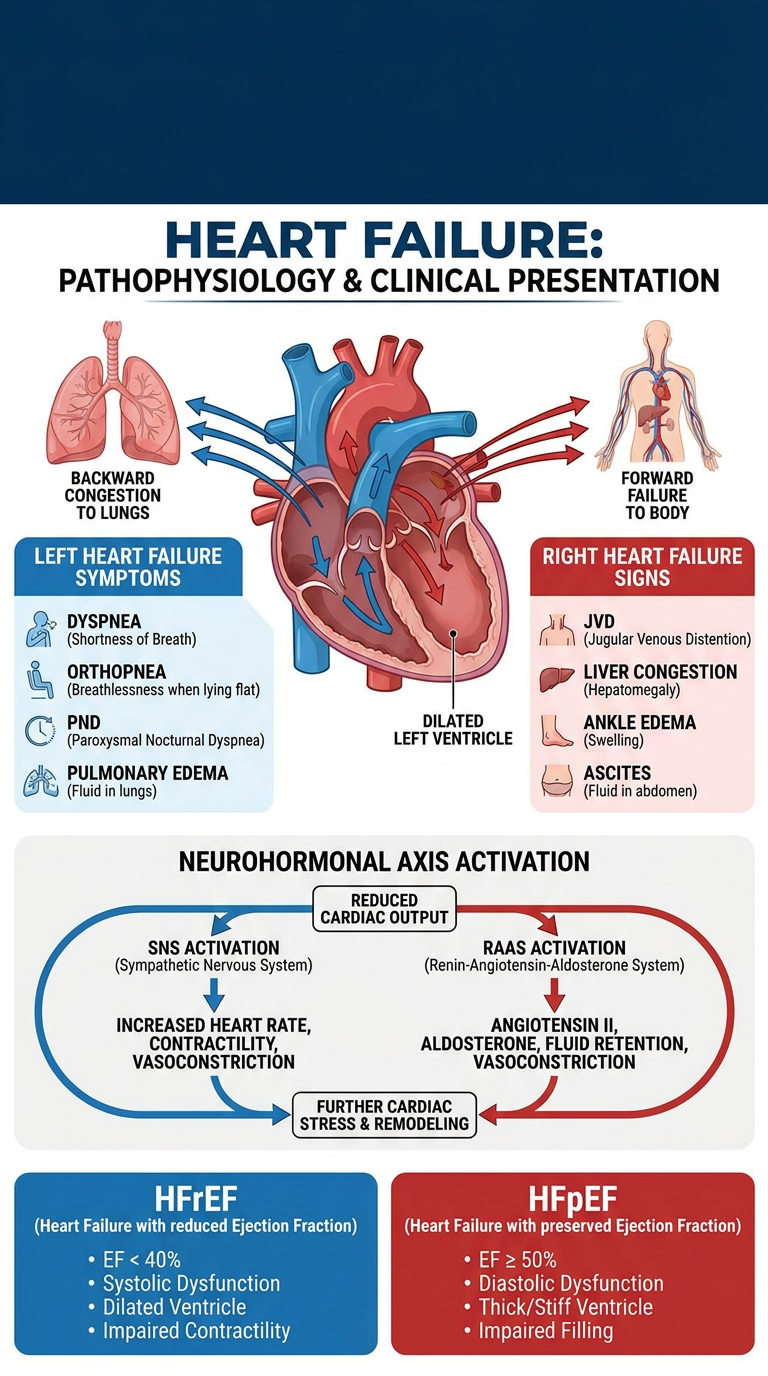
<tr><td><strong>Symptoms</strong></td><td>Dyspnea, orthopnea, PND, cardiac asthma, hemoptysis</td><td>Ankle edema, abdominal distension, anorexia, nausea</td></tr>
<tr><td><strong>Signs</strong></td><td>S3 gallop, basal crepitations, cardiomegaly, displaced apex</td><td>JVD, hepatomegaly, ascites, peripheral edema</td></tr>
<tr><td><strong>Chest X-ray</strong></td><td>Cardiomegaly, upper lobe diversion, Kerley B lines, pulmonary edema, pleural effusion</td><td>Right-sided cardiomegaly, clear lung fields (if isolated RHF)</td></tr>
<tr><td><strong>Key Investigation</strong></td><td>Echo: ↓LVEF; BNP ↑↑; ECG — LVH, LBBB</td><td>Echo: RV dilation; TR; elevated PA pressure</td></tr>
</tbody>
</table>
</div>
</div>
<div class="divider"></div>
<!-- ══════════ ROW 5: Clinical Features + Diagnosis ══════════ -->
<div class="grid-2">
<!-- CLINICAL FEATURES -->
<div class="card card-green">
<div class="section-title"><span class="icon">🩺</span> Clinical Features</div>
<div class="sub-head">Symptoms (FORD mnemonic)</div>
<div class="mnemonic" style="padding:8px 12px; margin-top:4px; margin-bottom:8px;">
<div class="title">🧠 FORD = Key Symptoms of HF</div>
<div class="letters">
<div class="letter-block"><strong>F</strong>atigue / weakness</div>
<div class="letter-block"><strong>O</strong>rthopnea (≥2 pillows)</div>
<div class="letter-block"><strong>R</strong>ight-sided edema</div>
<div class="letter-block"><strong>D</strong>yspnea on exertion → at rest</div>
</div>
</div>
<div class="sub-head">Physical Examination Signs</div>
<ul class="dot-list">
<li>💓 <strong>S3 gallop</strong> — pathognomonic of volume overload / systolic HF (NEET favorite!)</li>
<li>💓 <strong>S4 gallop</strong> — diastolic dysfunction / HFpEF, stiff ventricle</li>
<li>🌊 <strong>JVD</strong> — elevated central venous pressure (right HF)</li>
<li>💧 <strong>Pitting edema</strong> — bilateral ankle to presacral</li>
<li>🫁 <strong>Bibasilar crepitations</strong> (rales) — pulmonary congestion</li>
<li>📍 <strong>Displaced apex</strong> — laterally displaced beyond mid-clavicular line</li>
<li>🩺 <strong>Pulsus alternans</strong> — severe LV dysfunction</li>
<li>🫀 <strong>Cheyne-Stokes breathing</strong> — severe/advanced HF</li>
</ul>
<div class="highlight-box hb-red">
<span class="warn-icon">⚠️</span>
<span><strong>Paroxysmal Nocturnal Dyspnea (PND)</strong> — patient wakes from sleep with breathlessness, must sit up/stand; highly specific for left HF</span>
</div>
</div>
<!-- DIAGNOSIS -->
<div class="card card-blue">
<div class="section-title"><span class="icon">🔬</span> Diagnosis & Investigations</div>
<div class="sub-head">Step-by-Step Approach</div>
<div class="step"><div class="step-num sn-blue">1</div><div class="step-text"><strong>History & Physical Exam</strong> — dyspnea, orthopnea, edema, S3, JVD</div></div>
<div class="step"><div class="step-num sn-blue">2</div><div class="step-text"><strong>ECG</strong> — LVH, Q waves (prior MI), LBBB, AF, arrhythmias; helps determine CRT eligibility (LBBB >150ms)</div></div>
<div class="step"><div class="step-num sn-blue">3</div><div class="step-text"><strong>Chest X-Ray</strong> — Cardiomegaly (CTR >0.5), Kerley B lines, bat-wing pulmonary edema, upper lobe diversion, pleural effusion</div></div>
<div class="step"><div class="step-num sn-blue">4</div><div class="step-text"><strong>Echocardiogram</strong> — GOLD STANDARD; measures LVEF, wall motion, valves, diastolic function</div></div>
<div class="step"><div class="step-num sn-blue">5</div><div class="step-text"><strong>BNP / NT-proBNP</strong> — best initial biomarker; sensitivity ~95-99%; reduced by obesity, ↑ by renal failure & age</div></div>
<div class="step"><div class="step-num sn-blue">6</div><div class="step-text"><strong>Labs</strong> — CBC, BMP, LFTs, TFTs, glucose, lipids, troponin, urinalysis</div></div>
<div class="highlight-box hb-yellow" style="margin-top:8px;">
<span class="warn-icon">⭐</span>
<div>
<strong>BNP PEARLS (NEET PG FAVORITE):</strong><br>
• BNP <100 pg/mL → HF unlikely<br>
• BNP >400 pg/mL → HF very likely<br>
• BNP 100–400 → grey zone (consider other causes)<br>
• Obesity ↓ BNP levels (falsely low!)<br>
• Troponin ↑ in acute HF → worse prognosis
</div>
</div>
</div>
</div>
<!-- ══════════ ROW 6: Management ══════════ -->
<div class="grid-full">
<div class="card card-dark">
<div class="section-title"><span class="icon">💊</span> Management of Heart Failure — HFrEF (LVEF <40%)</div>
<table class="info-table" style="color:#f8fafc;">
<thead>
<tr>
<th class="th-dark">Drug Class</th>
<th class="th-dark">Drugs</th>
<th class="th-dark">Mechanism</th>
<th class="th-dark">LVEF Benefit</th>
<th class="th-dark">Key Contraindication / Note</th>
</tr>
</thead>
<tbody>
<tr style="border-bottom:1px solid rgba(255,255,255,0.08)">
<td><span class="pill pill-blue">ACE Inhibitor</span></td>
<td>Enalapril, Ramipril, Lisinopril</td>
<td>↓ Ang II → vasodilate + ↓ remodeling</td>
<td style="color:#4ade80;font-weight:700">↑ EF, ↑ survival</td>
<td>Avoid in bilateral renal artery stenosis, pregnancy; Dry cough → switch to ARB</td>
</tr>
<tr style="border-bottom:1px solid rgba(255,255,255,0.08); background:rgba(255,255,255,0.03)">
<td><span class="pill pill-purple">Beta-Blocker</span></td>
<td>Carvedilol, Metoprolol succinate, Bisoprolol</td>
<td>↓ SNS → anti-remodeling, anti-arrhythmic</td>
<td style="color:#4ade80;font-weight:700">↑ EF, ↑ survival</td>
<td>START LOW, GO SLOW; avoid in acute decompensation</td>
</tr>
<tr style="border-bottom:1px solid rgba(255,255,255,0.08)">
<td><span class="pill pill-orange">MRA</span></td>
<td>Spironolactone, Eplerenone</td>
<td>Aldosterone antagonist → ↓ fibrosis, ↓ Na retention</td>
<td style="color:#4ade80;font-weight:700">↑ survival</td>
<td>Monitor K⁺ — risk of hyperkalemia; Spironolactone → gynecomastia</td>
</tr>
<tr style="border-bottom:1px solid rgba(255,255,255,0.08); background:rgba(255,255,255,0.03)">
<td><span class="pill pill-teal">ARNI</span></td>
<td>Sacubitril/Valsartan (Entresto)</td>
<td>Neprilysin inhibitor + ARB → ↑ natriuretic peptides</td>
<td style="color:#4ade80;font-weight:700">Superior to ACEi</td>
<td>PARADIGM-HF trial; avoid with ACEi (36hr washout); CI in angioedema</td>
</tr>
<tr style="border-bottom:1px solid rgba(255,255,255,0.08)">
<td><span class="pill pill-green">SGLT2 Inhibitor</span></td>
<td>Dapagliflozin, Empagliflozin</td>
<td>Glucosuria → natriuresis + cardioprotective</td>
<td style="color:#4ade80;font-weight:700">↓ hospitalization</td>
<td>Works in both HFrEF and HFpEF (EMPEROR-Reduced/Preserved trials)</td>
</tr>
<tr style="border-bottom:1px solid rgba(255,255,255,0.08); background:rgba(255,255,255,0.03)">
<td><span class="pill pill-yellow">Diuretics</span></td>
<td>Furosemide (loop), Torsemide, Metolazone (thiazide)</td>
<td>↓ preload → symptom relief (fluid)</td>
<td style="color:#fbbf24;font-weight:700">Symptom only</td>
<td>No mortality benefit alone; Monitor electrolytes; Metolazone used for diuretic resistance</td>
</tr>
<tr style="background:rgba(255,255,255,0.03)">
<td><span class="pill pill-pink">Hydralazine + ISDN</span></td>
<td>Hydralazine + Isosorbide dinitrate</td>
<td>Vasodilator (arterial + venous)</td>
<td style="color:#4ade80;font-weight:700">↑ survival</td>
<td>First-line for HFrEF in Black patients (A-HeFT trial); use if ACEi/ARB not tolerated</td>
</tr>
</tbody>
</table>
</div>
</div>
<!-- ══════════ ROW 7: Device Therapy + HFpEF management ══════════ -->
<div class="grid-2">
<div class="card card-teal">
<div class="section-title"><span class="icon">🔋</span> Device Therapy (HFrEF)</div>
<table class="info-table">
<thead>
<tr><th class="th-teal">Device</th><th class="th-teal">Indication</th><th class="th-teal">Key Criteria</th></tr>
</thead>
<tbody class="tr-alt">
<tr><td><strong>ICD</strong><br>(Implantable Cardioverter Defibrillator)</td><td>Primary prevention of sudden cardiac death</td><td>EF ≤ 35%, NYHA II-III, optimal medical therapy ≥3 months</td></tr>
<tr><td><strong>CRT</strong><br>(Cardiac Resynchronization Therapy)</td><td>Correct dyssynchrony in HF</td><td>EF ≤ 35%, LBBB ≥150ms, NYHA II-IV, sinus rhythm</td></tr>
<tr><td><strong>CRT-D</strong></td><td>Both resynchronization + defibrillation</td><td>Combined criteria</td></tr>
<tr><td><strong>LVAD</strong></td><td>Stage D HF — bridge to transplant or destination therapy</td><td>EF <25%, severe symptoms despite max therapy</td></tr>
</tbody>
</table>
</div>
<div class="card card-orange">
<div class="section-title"><span class="icon">🏥</span> HFpEF Management & Acute Decompensation</div>
<div class="sub-head">HFpEF (EF ≥50%) — Limited evidence-based therapy</div>
<ul class="dot-list">
<li>🎯 Control underlying cause — HTN, DM, AF, obesity</li>
<li>💊 Diuretics — for symptom relief / fluid management</li>
<li>🆕 SGLT2 inhibitors (Empagliflozin) — ↓ hospitalization (EMPEROR-Preserved)</li>
<li>⚠️ ACEi / Beta-blockers — no clear mortality benefit in HFpEF</li>
</ul>
<div class="sub-head" style="margin-top:8px;">Acute Decompensated HF — LMNOP</div>
<div class="mnemonic" style="padding:8px 12px; margin-top:4px;">
<div class="title">🚨 LMNOP — Emergency Treatment</div>
<div class="letters">
<div class="letter-block"><strong>L</strong>asix (furosemide IV)</div>
<div class="letter-block"><strong>M</strong>orphine (anxiety, vasodilation)</div>
<div class="letter-block"><strong>N</strong>itrates (↓ preload)</div>
<div class="letter-block"><strong>O</strong>xygen (high-flow)</div>
<div class="letter-block"><strong>P</strong>ositioning (upright/sit)</div>
</div>
</div>
</div>
</div>
<div class="divider"></div>
<!-- ══════════ ROW 8: Complications + Investigations ══════════ -->
<div class="grid-2">
<div class="card card-red">
<div class="section-title"><span class="icon">⚠️</span> Complications</div>
<ul class="dot-list">
<li>🫀 <strong>Sudden Cardiac Death</strong> — most common cause of death in HF; VF/VT</li>
<li>🫀 <strong>Atrial Fibrillation</strong> — most common arrhythmia complicating HF; ↑ stroke risk</li>
<li>🩸 <strong>Cardiorenal Syndrome</strong> — ↓ renal perfusion → AKI / CKD progression</li>
<li>🫁 <strong>Pulmonary Edema</strong> — acute decompensation, life-threatening</li>
<li>🫁 <strong>Pleural Effusion</strong> — more common on RIGHT side (if unilateral)</li>
<li>🦵 <strong>DVT / Pulmonary Embolism</strong> — stasis + hypercoagulability</li>
<li>🧠 <strong>Cachexia</strong> — cardiac cachexia; ↑ cytokines, ↓ appetite</li>
<li>🩺 <strong>Hepatic congestion</strong> → congestive hepatopathy → cardiac cirrhosis</li>
<li>💊 <strong>Drug toxicity</strong> — digoxin toxicity (hypokalemia precipitates)</li>
</ul>
</div>
<div class="card card-yellow">
<div class="section-title"><span class="icon">🧪</span> Important Investigations Summary</div>
<table class="info-table">
<thead>
<tr><th class="th-orange">Investigation</th><th class="th-orange">Finding / Significance</th></tr>
</thead>
<tbody class="tr-alt">
<tr><td>🔬 <strong>BNP/NT-proBNP</strong></td><td>Best initial test; raised in all HF types; guides therapy</td></tr>
<tr><td>📷 <strong>Echo (TTE)</strong></td><td>GOLD STANDARD — EF, wall motion, valves, diastology</td></tr>
<tr><td>📋 <strong>ECG</strong></td><td>LVH, Q waves, LBBB → guides device therapy</td></tr>
<tr><td>🫁 <strong>Chest X-Ray</strong></td><td>CTR >0.5, Kerley B lines, upper lobe diversion, bat-wing</td></tr>
<tr><td>🩸 <strong>Troponin</strong></td><td>Elevated in acute HF → ongoing myocyte injury → ↑ mortality</td></tr>
<tr><td>🫘 <strong>Renal function/electrolytes</strong></td><td>Baseline; monitor on diuretics/ACEi; eGFR for drug dosing</td></tr>
<tr><td>🦋 <strong>TSH</strong></td><td>Rule out thyroid cause (hypothyroid = DCM, hyperthyroid = AF/HF)</td></tr>
<tr><td>🧬 <strong>Cardiac MRI</strong></td><td>Best for cardiomyopathy characterization, viability, fibrosis</td></tr>
<tr><td>🩺 <strong>Coronary angiography</strong></td><td>If ischemic etiology suspected; assess for revascularization</td></tr>
</tbody>
</table>
</div>
</div>
<!-- ══════════ ROW 9: High-Yield Pearls + Mnemonics ══════════ -->
<div class="grid-2">
<!-- PEARLS -->
<div class="card card-green">
<div class="section-title"><span class="icon">💎</span> High-Yield Exam Pearls (NEET PG Favorites)</div>
<div class="pearl" style="margin-top:12px;">
<p><strong>PEARL 1:</strong> S3 gallop = PATHOGNOMONIC of systolic HF (volume overload). S4 = diastolic dysfunction / stiff ventricle.</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 2:</strong> BNP is REDUCED in obesity (falsely low). INCREASED in renal failure, old age.</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 3:</strong> Sacubitril/Valsartan (ARNI) is SUPERIOR to ACEi alone (PARADIGM-HF trial). Must have 36h washout period between ACEi → ARNI to prevent angioedema.</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 4:</strong> Carvedilol (non-selective BB) is the only beta-blocker proven to reduce mortality in all 3 NYHA classes II, III, IV.</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 5:</strong> Digoxin does NOT reduce mortality — only reduces hospitalizations and symptoms (DIG trial).</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 6:</strong> Pleural effusion in HF is more often <strong>RIGHT-sided</strong>; bilateral is common. Left-sided alone → think other cause.</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 7:</strong> CRT indication = EF ≤35% + LBBB ≥150ms + NYHA II-IV + sinus rhythm — improves EF, symptoms and survival.</p>
</div>
</div>
<!-- MNEMONICS -->
<div class="card card-purple">
<div class="section-title"><span class="icon">🧠</span> Memory Tricks & Mnemonics</div>
<div class="mnemonic" style="margin-bottom:10px;">
<div class="title">🫀 4 PILLARS of HFrEF Treatment — "A-BODE"</div>
<div class="letters">
<div class="letter-block"><strong>A</strong>CEi / ARNI</div>
<div class="letter-block"><strong>B</strong>eta-Blocker</div>
<div class="letter-block"><strong>O</strong>ld — MRA (aldosterone)</div>
<div class="letter-block"><strong>D</strong>apagliflozin (SGLT2i)</div>
<div class="letter-block"><strong>E</strong>diuresis prn</div>
</div>
</div>
<div class="mnemonic" style="margin-bottom:10px;">
<div class="title">🚨 Causes of Acute Decompensation — "FAILURE"</div>
<div class="letters">
<div class="letter-block"><strong>F</strong>orgot medications</div>
<div class="letter-block"><strong>A</strong>rrhythmia / AF</div>
<div class="letter-block"><strong>I</strong>schemia / MI</div>
<div class="letter-block"><strong>L</strong>ifestyle (salt, fluid excess)</div>
<div class="letter-block"><strong>U</strong>pload (fluid overload IV)</div>
<div class="letter-block"><strong>R</strong>enal failure</div>
<div class="letter-block"><strong>E</strong>ndocrine (thyroid, DM)</div>
</div>
</div>
<div class="mnemonic" style="margin-bottom:10px;">
<div class="title">📋 Framingham Criteria (2 major OR 1 major + 2 minor)</div>
<div style="display:flex; gap:8px; margin-top:6px;">
<div style="flex:1; background:rgba(255,255,255,0.07); border-radius:8px; padding:6px 10px;">
<div style="color:#f9ca24; font-size:9.5px; font-weight:700; margin-bottom:4px;">MAJOR CRITERIA</div>
<div style="font-size:9.5px; color:#e2e8f0; line-height:1.6;">
• PND or orthopnea<br>
• S3 gallop<br>
• JVD (venous distension)<br>
• Cardiomegaly<br>
• Acute pulmonary edema<br>
• Hepatojugular reflux<br>
• ≥4.5 kg weight loss in 5 days on treatment
</div>
</div>
<div style="flex:1; background:rgba(255,255,255,0.07); border-radius:8px; padding:6px 10px;">
<div style="color:#a78bfa; font-size:9.5px; font-weight:700; margin-bottom:4px;">MINOR CRITERIA</div>
<div style="font-size:9.5px; color:#e2e8f0; line-height:1.6;">
• Bilateral ankle edema<br>
• Night cough<br>
• Dyspnea on exertion<br>
• Hepatomegaly<br>
• Pleural effusion<br>
• HR >120 bpm<br>
• Tachycardia
</div>
</div>
</div>
</div>
<div class="mnemonic">
<div class="title">💊 Drugs that WORSEN HF — "SAD DRUGS"</div>
<div class="letters">
<div class="letter-block"><strong>S</strong>odium-retaining (NSAIDs, steroids)</div>
<div class="letter-block"><strong>A</strong>nti-arrhythmics (flecainide, disopyramide)</div>
<div class="letter-block"><strong>D</strong>iltilazem / Verapamil (non-DHP CCBs)</div>
<div class="letter-block"><strong>D</strong>oxorubicin / anthracyclines</div>
<div class="letter-block"><strong>R</strong>osiglitazone (TZDs)</div>
<div class="letter-block"><strong>U</strong>nexplained alcohol</div>
<div class="letter-block"><strong>G</strong>rowth hormone excess</div>
<div class="letter-block"><strong>S</strong>timulants (cocaine, meth)</div>
</div>
</div>
</div>
</div>
<!-- ══════════ ROW 10: Comparison Table: HFrEF vs HFpEF ══════════ -->
<div class="grid-full">
<div class="card card-indigo">
<div class="section-title"><span class="icon">⚖️</span> HFrEF vs HFpEF — Master Comparison Table</div>
<table class="info-table">
<thead>
<tr>
<th class="th-purple" style="width:18%">Parameter</th>
<th class="th-purple">HFrEF (Systolic HF)</th>
<th style="background:#ddd6fe;color:#4c1d95;font-weight:700;padding:5px 8px;font-size:9.5px;text-transform:uppercase;letter-spacing:0.3px;">HFpEF (Diastolic HF)</th>
</tr>
</thead>
<tbody class="tr-alt">
<tr><td><strong>EF</strong></td><td style="color:#dc2626;font-weight:700"><40% (reduced)</td><td style="color:#16a34a;font-weight:700">≥50% (preserved)</td></tr>
<tr><td><strong>Mechanism</strong></td><td>↓ Contractility (systolic dysfunction)</td><td>↓ Relaxation / ↑ Stiffness (diastolic dysfunction)</td></tr>
<tr><td><strong>LV size</strong></td><td>Dilated (↑ EDV)</td><td>Normal or small (concentric hypertrophy)</td></tr>
<tr><td><strong>Wall thickness</strong></td><td>Thin walls (dilated)</td><td>Thick walls (hypertrophy)</td></tr>
<tr><td><strong>Common causes</strong></td><td>MI, DCM, myocarditis</td><td>Hypertension, Diabetes, Obesity, Aging</td></tr>
<tr><td><strong>Demographics</strong></td><td>Younger males; post-MI</td><td>Older females; hypertensive</td></tr>
<tr><td><strong>Mortality</strong></td><td style="color:#dc2626">High (comparable to HFpEF)</td><td style="color:#dc2626">Similar to HFrEF</td></tr>
<tr><td><strong>Evidence-based Rx</strong></td><td>ACEi/ARNI + BB + MRA + SGLT2i (4 pillars)</td><td>SGLT2i (empagliflozin) + diuretics; control comorbidities</td></tr>
<tr><td><strong>Echo finding</strong></td><td>E/A <1 pattern reversed; dilated LV; global hypokinesia</td><td>E/e' ratio >13; LA enlargement; concentric LVH</td></tr>
<tr><td><strong>Drug to avoid</strong></td><td>Inotropes (long term); DHP CCBs worsen remodeling</td><td>ACEi (minimal benefit); Nitrates (↓ preload too much)</td></tr>
</tbody>
</table>
</div>
</div>
<!-- ══════════ WARNING SIGNS / RED FLAGS ══════════ -->
<div class="grid-3">
<div class="card card-red">
<div class="section-title"><span class="icon">🚨</span> Red Flag / Warning Signs</div>
<div class="highlight-box hb-red">
<span class="warn-icon">🆘</span>
<div>
<strong>Admit Immediately if:</strong><br>
• SpO₂ <90% despite O₂<br>
• HR >130 bpm or <40 bpm<br>
• SBP <90 mmHg (cardiogenic shock)<br>
• New-onset HF with hemodynamic instability<br>
• Altered mental status
</div>
</div>
<ul class="dot-list" style="margin-top:8px;">
<li>🔴 Acute pulmonary edema — EMERGENCY</li>
<li>🔴 Cardiogenic shock — LVAD / transplant urgency</li>
<li>🔴 Ventricular tachycardia → SCD risk</li>
</ul>
</div>
<div class="card card-green">
<div class="section-title"><span class="icon">📊</span> Prognosis / Staging</div>
<ul class="dot-list">
<li>1-year mortality: NYHA IV = ~50%</li>
<li>5-year mortality: ~50% overall (worse than most cancers)</li>
<li>SCD accounts for ~50% of deaths in HFrEF</li>
<li>↑ BNP = ↑ mortality risk</li>
<li>↑ Troponin in acute HF = ↑ in-hospital mortality</li>
<li>Hyponatremia = poor prognostic sign</li>
<li>EF improvement on therapy = favorable prognosis</li>
</ul>
<div class="highlight-box hb-green">
<span class="warn-icon">✅</span>
<span>LVEF can <strong>recover</strong> in tachycardia-mediated CMP, peripartum CMP, and alcohol CMP with treatment!</span>
</div>
</div>
<div class="card card-yellow">
<div class="section-title"><span class="icon">🌟</span> One-Liners to Remember</div>
<ul class="dot-list">
<li>🎯 CAD = #1 cause of HF in developed world (~70%)</li>
<li>🎯 Echo = investigation of choice for HF</li>
<li>🎯 S3 = best bedside sign for systolic HF</li>
<li>🎯 Sacubitril/Valsartan = superior to ACEi (PARADIGM-HF)</li>
<li>🎯 SGLT2i works in BOTH HFrEF and HFpEF</li>
<li>🎯 Digoxin = symptom relief only, NOT mortality benefit</li>
<li>🎯 Ivabradine — HR reduction in sinus tachycardia when BB not tolerated</li>
<li>🎯 ICD if EF ≤35% after 90 days optimal therapy</li>
<li>🎯 Pleural effusion in HF = usually RIGHT-sided</li>
<li>🎯 Cheyne-Stokes = ominous sign of severe/advanced HF</li>
</ul>
</div>
</div>
<!-- ══════════ FOOTER ══════════ -->
<div class="footer">
<p>📚 Sources: <strong>Braunwald's Heart Disease</strong> | <strong>Goldman-Cecil Medicine</strong> | <strong>Goodman & Gilman's Pharmacology</strong> | <strong>Fuster & Hurst's The Heart</strong></p>
<p>🩺 <strong>NEET PG / MD Entrance High-Yield Sheet</strong> | Cardiovascular System | ✨ Orris AI</p>
</div>
</div>
</body>
</html>
cd /tmp/workspace/heart-failure-poster && python3 -c " import subprocess, sys # Try weasyprint first try: import weasyprint weasyprint.HTML(filename='heart_failure_poster.html').write_pdf('heart_failure_poster.pdf') print('WeasyPrint: SUCCESS') except Exception as e: print(f'WeasyPrint failed: {e}') # Try xhtml2pdf try: from xhtml2pdf import pisa with open('heart_failure_poster.html', 'rb') as src, open('heart_failure_poster.pdf', 'wb') as dest: pisa.CreatePDF(src, dest) print('xhtml2pdf: SUCCESS') except Exception as e2: print(f'xhtml2pdf failed: {e2}') "
pip install --user weasyprint --quiet 2>&1 | tail -5
cd /tmp/workspace/heart-failure-poster && python3 -c " # Use reportlab to build a PDF from the poster content # Since HTML→PDF isn't directly available, let's use the reportlab approach # but given the complexity, let's try selenium or playwright import subprocess result = subprocess.run(['python3', '-c', 'import playwright'], capture_output=True, text=True) print('playwright:', result.returncode) result2 = subprocess.run(['python3', '-c', 'import selenium'], capture_output=True, text=True) print('selenium:', result2.returncode) result3 = subprocess.run(['chromium-browser', '--version'], capture_output=True, text=True) print('chromium:', result3.stdout, result3.stderr) result4 = subprocess.run(['chromium', '--version'], capture_output=True, text=True) print('chromium2:', result4.stdout, result4.stderr) result5 = subprocess.run(['google-chrome', '--version'], capture_output=True, text=True) print('chrome:', result5.stdout, result5.stderr) "
python3 -c "import cssselect2; print(cssselect2.__file__)"
python3 -c " import sys sys.path.insert(0, '/opt/amazon/genesis1p-tools/venv/lib64/python3.12/site-packages') import weasyprint print('weasyprint available via venv path') " 2>&1
ls -lh /tmp/workspace/heart-failure-poster/
Heart Failure medical infographic poster for NEET PG students. Include: anatomical heart diagram showing enlarged dilated left ventricle, arrows showing backward congestion to lungs and forward failure to body. Label left heart failure symptoms (dyspnea, orthopnea, PND, pulmonary edema) on left side and right heart failure signs (JVD, liver congestion, ankle edema, ascites) on right side. Show neurohormonal axis with RAAS and SNS activation loop. Color-coded boxes for HFrEF vs HFpEF. Professional medical style, white background, blue and red color scheme, clean typography.
💓 HEART FAILURE — High-Yield Infographic Poster
📥 Download Your Poster
heart failure poster
HTML File · HTML
Open in any browser and use Ctrl+P → Save as PDF (set to landscape, scale to fit) for a perfect print-ready PDF.
🖼️ Visual Pathophysiology Diagram
📋 What's Inside the Poster (All 12 Sections)
| Section | Content |
|---|---|
| 📘 Definition | Clinical syndrome, global statistics, key concept |
| 📊 Classification by EF | HFrEF / HFmrEF / HFpEF with EF cutoffs |
| 🏃 NYHA Functional Classes | I-IV with activity limitations |
| 📈 ACC/AHA Staging 2022 | Stages A-D with intervention goals |
| 🔎 Causes / Etiology | CAD #1 cause + CARDIAC mnemonic |
| ⚙️ Pathophysiology | 4-system model (Heart/Vessels/Kidney/Neurohormonal) |
| ↔️ Left vs Right HF | Full comparison table |
| 🩺 Clinical Features | FORD mnemonic + all physical signs |
| 🔬 Diagnosis | Step-by-step + BNP pearls |
| 💊 Management | 4 pillars of HFrEF + LMNOP for acute HF |
| ⚠️ Complications | SCD, AF, cardiorenal syndrome |
| 💎 Pearls + Mnemonics | ABODE, FAILURE, Framingham, SAD DRUGS |
🔥 Top 5 NEET PG One-Liners
- S3 gallop = pathognomonic of systolic HF (volume overload)
- BNP reduced in obesity (falsely low) - always remember!
- Sacubitril/Valsartan (PARADIGM-HF) is SUPERIOR to ACEi alone
- SGLT2 inhibitors work in BOTH HFrEF and HFpEF
- ICD = EF ≤35% + NYHA II-III + on optimal therapy ≥3 months
MASTER PROMPT TEMPLATE ✨ Create a clean high-yield medical infographic poster for emergency medicine pg resident 1st year about: ACUTE SPINE INJURY Style: modern medical infographic highly organized exam-focused visually memorable colorful but professional easy to review before exams include emojis/icons for memory aid use clear section boxes and arrows use concise bullet points use tables for comparisons use color-coded categories include important high-yield notes and warning signs make it aesthetically pleasing like premium study notes white background readable font structured like a study cheat sheet Must include: Definition Classification Causes / risk factors Pathophysiology Clinical features Diagnosis Management Complications Important investigations High-yield exam pearls Memory tricks / mnemonics Comparison tables if applicable
mkdir -p /tmp/workspace/spine-injury-poster && echo "ready"
~/spine-injury-poster/acute_spine_injury_poster.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<meta name="viewport" content="width=device-width, initial-scale=1.0">
<title>Acute Spine Injury – Emergency Medicine High-Yield Infographic</title>
<style>
@import url('https://fonts.googleapis.com/css2?family=Inter:wght@300;400;500;600;700;800;900&family=Poppins:wght@400;600;700;800&display=swap');
* { margin: 0; padding: 0; box-sizing: border-box; }
body {
font-family: 'Inter', sans-serif;
background: #f1f5f9;
color: #0f172a;
font-size: 11px;
line-height: 1.5;
}
.page {
width: 1200px;
margin: 0 auto;
background: #ffffff;
padding: 20px 24px 28px;
}
/* ─── HEADER ─── */
.header {
background: linear-gradient(135deg, #0f172a 0%, #1e3a5f 35%, #1d4ed8 70%, #7c3aed 100%);
border-radius: 16px;
padding: 20px 28px;
display: flex;
align-items: center;
justify-content: space-between;
margin-bottom: 16px;
box-shadow: 0 8px 32px rgba(15,23,42,0.3);
position: relative;
overflow: hidden;
}
.header::before {
content: '🦴';
position: absolute;
right: 200px;
top: 50%;
transform: translateY(-50%);
font-size: 90px;
opacity: 0.08;
}
.header-left h1 {
font-family: 'Poppins', sans-serif;
font-size: 30px;
font-weight: 800;
color: #fff;
letter-spacing: -0.5px;
}
.header-left h1 span { color: #fbbf24; }
.header-left p {
font-size: 11.5px;
color: #93c5fd;
margin-top: 4px;
font-weight: 500;
}
.header-badges {
display: flex;
gap: 7px;
flex-wrap: wrap;
justify-content: flex-end;
}
.badge {
background: rgba(255,255,255,0.12);
color: #fff;
border: 1px solid rgba(255,255,255,0.25);
border-radius: 20px;
padding: 4px 12px;
font-size: 9.5px;
font-weight: 700;
backdrop-filter: blur(4px);
}
.badge.hot { background: rgba(251,191,36,0.2); border-color: #fbbf24; color: #fbbf24; }
.badge.em { background: rgba(239,68,68,0.2); border-color: #ef4444; color: #fca5a5; }
/* ─── GRID LAYOUTS ─── */
.grid-3 { display: grid; grid-template-columns: 1fr 1fr 1fr; gap: 13px; margin-bottom: 13px; }
.grid-2 { display: grid; grid-template-columns: 1fr 1fr; gap: 13px; margin-bottom: 13px; }
.grid-1-2 { display: grid; grid-template-columns: 1fr 2fr; gap: 13px; margin-bottom: 13px; }
.grid-2-1 { display: grid; grid-template-columns: 2fr 1fr; gap: 13px; margin-bottom: 13px; }
.grid-full { margin-bottom: 13px; }
/* ─── CARDS ─── */
.card {
border-radius: 12px;
padding: 13px 15px;
border: 1.5px solid transparent;
position: relative;
overflow: hidden;
}
.card::before {
content: '';
position: absolute;
top: 0; left: 0;
width: 4px; height: 100%;
border-radius: 12px 0 0 12px;
}
.card-blue { background: #eff6ff; border-color: #bfdbfe; } .card-blue::before { background: #2563eb; }
.card-green { background: #f0fdf4; border-color: #bbf7d0; } .card-green::before { background: #16a34a; }
.card-red { background: #fff1f2; border-color: #fecdd3; } .card-red::before { background: #dc2626; }
.card-purple { background: #faf5ff; border-color: #e9d5ff; } .card-purple::before { background: #7c3aed; }
.card-orange { background: #fff7ed; border-color: #fed7aa; } .card-orange::before { background: #ea580c; }
.card-teal { background: #f0fdfa; border-color: #99f6e4; } .card-teal::before { background: #0d9488; }
.card-yellow { background: #fefce8; border-color: #fde68a; } .card-yellow::before { background: #ca8a04; }
.card-pink { background: #fdf2f8; border-color: #f9a8d4; } .card-pink::before { background: #db2777; }
.card-indigo { background: #eef2ff; border-color: #c7d2fe; } .card-indigo::before { background: #4f46e5; }
.card-slate { background: #f8fafc; border-color: #cbd5e1; } .card-slate::before { background: #475569; }
.card-dark { background: #0f172a; border-color: #1e293b; color: #f8fafc; } .card-dark::before { background: #fbbf24; }
.card-crimson { background: #fff0f0; border-color: #fca5a5; } .card-crimson::before { background: #b91c1c; }
/* ─── SECTION TITLES ─── */
.section-title {
font-family: 'Poppins', sans-serif;
font-size: 11px;
font-weight: 700;
margin-bottom: 8px;
display: flex;
align-items: center;
gap: 5px;
text-transform: uppercase;
letter-spacing: 0.6px;
}
.card-blue .section-title { color: #1d4ed8; }
.card-green .section-title { color: #15803d; }
.card-red .section-title { color: #b91c1c; }
.card-purple .section-title { color: #6d28d9; }
.card-orange .section-title { color: #c2410c; }
.card-teal .section-title { color: #0f766e; }
.card-yellow .section-title { color: #92400e; }
.card-pink .section-title { color: #be185d; }
.card-indigo .section-title { color: #3730a3; }
.card-slate .section-title { color: #334155; }
.card-dark .section-title { color: #fbbf24; }
.card-crimson .section-title { color: #991b1b; }
/* ─── LISTS ─── */
ul.dot-list { list-style: none; padding: 0; }
ul.dot-list li { padding: 2px 0 2px 14px; position: relative; font-size: 10.5px; color: #374151; }
ul.dot-list li::before { content: '▸'; position: absolute; left: 0; color: #6b7280; font-size: 9px; top: 3px; }
.card-dark ul.dot-list li { color: #cbd5e1; }
.card-dark ul.dot-list li::before { color: #fbbf24; }
/* ─── TABLES ─── */
table.info-table {
width: 100%;
border-collapse: collapse;
font-size: 10px;
margin-top: 4px;
}
table.info-table th {
padding: 5px 7px;
font-weight: 700;
text-align: left;
font-size: 9.5px;
text-transform: uppercase;
letter-spacing: 0.3px;
}
table.info-table td {
padding: 4px 7px;
border-bottom: 1px solid rgba(0,0,0,0.05);
vertical-align: top;
line-height: 1.4;
}
table.info-table tr:last-child td { border-bottom: none; }
.tr-alt tr:nth-child(even) td { background: rgba(0,0,0,0.022); }
.th-blue { background: #dbeafe; color: #1e3a8a; }
.th-green { background: #dcfce7; color: #14532d; }
.th-red { background: #fee2e2; color: #7f1d1d; }
.th-purple { background: #ede9fe; color: #4c1d95; }
.th-orange { background: #fed7aa; color: #7c2d12; }
.th-teal { background: #ccfbf1; color: #134e4a; }
.th-slate { background: #e2e8f0; color: #1e293b; }
.th-dark { background: #1e293b; color: #f8fafc; }
.th-indigo { background: #e0e7ff; color: #312e81; }
/* ─── PILLS ─── */
.pill { display: inline-block; padding: 2px 8px; border-radius: 20px; font-size: 9px; font-weight: 700; margin: 1px 2px; }
.pill-red { background: #fee2e2; color: #b91c1c; border: 1px solid #fca5a5; }
.pill-blue { background: #dbeafe; color: #1d4ed8; border: 1px solid #93c5fd; }
.pill-green { background: #dcfce7; color: #15803d; border: 1px solid #86efac; }
.pill-orange { background: #ffedd5; color: #c2410c; border: 1px solid #fb923c; }
.pill-purple { background: #ede9fe; color: #6d28d9; border: 1px solid #c4b5fd; }
.pill-teal { background: #ccfbf1; color: #0f766e; border: 1px solid #5eead4; }
.pill-yellow { background: #fef3c7; color: #92400e; border: 1px solid #fcd34d; }
.pill-pink { background: #fce7f3; color: #be185d; border: 1px solid #f9a8d4; }
.pill-slate { background: #f1f5f9; color: #475569; border: 1px solid #cbd5e1; }
.pill-crimson{ background: #fff1f2; color: #9f1239; border: 1px solid #fda4af; }
/* ─── HIGHLIGHT / ALERT BOXES ─── */
.alert {
border-radius: 8px;
padding: 7px 11px;
margin-top: 7px;
font-size: 10px;
font-weight: 600;
display: flex;
align-items: flex-start;
gap: 6px;
line-height: 1.5;
}
.alert-red { background: #fef2f2; border: 1.5px solid #ef4444; color: #991b1b; }
.alert-yellow { background: #fefce8; border: 1.5px solid #eab308; color: #713f12; }
.alert-blue { background: #eff6ff; border: 1.5px solid #3b82f6; color: #1e3a8a; }
.alert-green { background: #f0fdf4; border: 1.5px solid #22c55e; color: #14532d; }
.alert-orange { background: #fff7ed; border: 1.5px solid #f97316; color: #7c2d12; }
.ai { font-size: 13px; flex-shrink: 0; margin-top: 1px; }
/* ─── MNEMONIC BOXES ─── */
.mnemonic {
background: linear-gradient(135deg, #0f172a, #1e293b);
border-radius: 10px;
padding: 9px 13px;
margin-top: 7px;
color: #f8fafc;
}
.mnemonic .mtitle {
font-family: 'Poppins', sans-serif;
font-size: 9.5px;
font-weight: 700;
color: #fbbf24;
text-transform: uppercase;
letter-spacing: 0.6px;
margin-bottom: 6px;
}
.mnemonic .letters { display: flex; flex-wrap: wrap; gap: 4px; }
.mnemonic .lb {
background: rgba(255,255,255,0.07);
border: 1px solid rgba(251,191,36,0.25);
border-radius: 6px;
padding: 3px 8px;
font-size: 10px;
}
.mnemonic .lb strong { color: #fbbf24; font-size: 12px; display: block; line-height: 1.2; }
/* ─── FLOW ARROWS ─── */
.flow {
display: flex;
align-items: center;
flex-wrap: wrap;
gap: 4px;
margin: 5px 0;
}
.fbox {
border-radius: 7px;
padding: 3px 9px;
font-size: 9.5px;
font-weight: 600;
border: 1.5px solid currentColor;
text-align: center;
}
.farr { font-size: 14px; color: #6b7280; }
/* ─── PEARL BOXES ─── */
.pearl {
background: linear-gradient(135deg, #f0fdf4, #dcfce7);
border: 1.5px solid #16a34a;
border-radius: 9px;
padding: 7px 11px;
margin-top: 6px;
position: relative;
}
.pearl::before { content: '💎'; position: absolute; top: -10px; left: 8px; font-size: 15px; }
.pearl p { font-size: 10px; color: #14532d; line-height: 1.5; }
/* ─── STEPS ─── */
.step { display: flex; gap: 7px; align-items: flex-start; padding: 3px 0; }
.snum {
width: 17px; height: 17px;
border-radius: 50%;
display: flex; align-items: center; justify-content: center;
font-size: 8.5px; font-weight: 800; flex-shrink: 0;
}
.sn-red { background: #dc2626; color: #fff; }
.sn-blue { background: #2563eb; color: #fff; }
.sn-green { background: #16a34a; color: #fff; }
.sn-orange { background: #ea580c; color: #fff; }
.sn-purple { background: #7c3aed; color: #fff; }
.stxt { font-size: 10.5px; color: #374151; flex: 1; }
/* ─── SUB-HEADINGS ─── */
.sh { font-size: 9.5px; font-weight: 700; text-transform: uppercase; letter-spacing: 0.4px; margin: 7px 0 3px; opacity: 0.75; }
.card-blue .sh { color: #1d4ed8; }
.card-green .sh { color: #15803d; }
.card-red .sh { color: #b91c1c; }
.card-purple .sh { color: #6d28d9; }
.card-orange .sh { color: #c2410c; }
.card-teal .sh { color: #0f766e; }
.card-yellow .sh { color: #92400e; }
.card-dark .sh { color: #fbbf24; }
.card-crimson .sh { color: #991b1b; }
.card-indigo .sh { color: #3730a3; }
/* ─── SYNDROME MINI-CARDS ─── */
.syndrome-grid {
display: grid;
grid-template-columns: 1fr 1fr;
gap: 7px;
margin-top: 5px;
}
.syn-card {
border-radius: 8px;
padding: 7px 10px;
border: 1.5px solid transparent;
}
.syn-central { background: #eff6ff; border-color: #93c5fd; }
.syn-brown { background: #fdf2f8; border-color: #f9a8d4; }
.syn-ant { background: #fff1f2; border-color: #fca5a5; }
.syn-post { background: #f0fdfa; border-color: #99f6e4; }
.syn-conus { background: #faf5ff; border-color: #d8b4fe; }
.syn-cauda { background: #fefce8; border-color: #fde68a; }
.syn-title { font-size: 9.5px; font-weight: 800; margin-bottom: 3px; }
.syn-central .syn-title { color: #1d4ed8; }
.syn-brown .syn-title { color: #be185d; }
.syn-ant .syn-title { color: #b91c1c; }
.syn-post .syn-title { color: #0f766e; }
.syn-conus .syn-title { color: #6d28d9; }
.syn-cauda .syn-title { color: #92400e; }
.syn-body { font-size: 9.5px; color: #374151; line-height: 1.5; }
/* ─── DIVIDER ─── */
.divider {
height: 3px;
background: linear-gradient(90deg, #dc2626, #ea580c, #fbbf24, #16a34a, #2563eb, #7c3aed);
border-radius: 2px;
margin: 13px 0;
}
/* ─── NEXUS BOX ─── */
.criteria-box {
background: #fff;
border: 2px solid #2563eb;
border-radius: 10px;
padding: 8px 12px;
margin-top: 5px;
}
.criteria-box .ctitle {
font-family: 'Poppins', sans-serif;
font-size: 10px;
font-weight: 700;
color: #1d4ed8;
margin-bottom: 5px;
text-transform: uppercase;
letter-spacing: 0.4px;
}
.criteria-box ul { list-style: none; padding: 0; }
.criteria-box ul li { font-size: 10px; color: #374151; padding: 2px 0 2px 14px; position: relative; }
.criteria-box ul li::before { content: '✓'; color: #16a34a; position: absolute; left: 0; font-weight: 700; }
/* ─── FOOTER ─── */
.footer {
background: #0f172a;
border-radius: 10px;
padding: 10px 20px;
display: flex;
justify-content: space-between;
align-items: center;
margin-top: 13px;
}
.footer p { color: #94a3b8; font-size: 9.5px; }
.footer strong { color: #fbbf24; }
/* ─── VERDICT TAG ─── */
.verdict {
display: inline-flex;
align-items: center;
gap: 4px;
padding: 3px 10px;
border-radius: 20px;
font-size: 9px;
font-weight: 800;
text-transform: uppercase;
letter-spacing: 0.4px;
}
.vgood { background: #dcfce7; color: #14532d; border: 1px solid #86efac; }
.vmod { background: #fef3c7; color: #92400e; border: 1px solid #fcd34d; }
.vpoor { background: #fee2e2; color: #991b1b; border: 1px solid #fca5a5; }
</style>
</head>
<body>
<div class="page">
<!-- ══════════ HEADER ══════════ -->
<div class="header">
<div class="header-left">
<h1>🦴 <span>ACUTE SPINE INJURY</span> — Emergency Medicine Master Sheet</h1>
<p>EMERGENCY MEDICINE | PGY-1 Resident Reference | Based on Rosen's EM, Tintinalli's EM, Current Surgical Therapy, Rockwood & Green's, Bailey & Love's</p>
</div>
<div class="header-badges">
<span class="badge hot">🔥 HIGH YIELD</span>
<span class="badge em">🚨 EMERGENCY</span>
<span class="badge">📚 Rosen's EM</span>
<span class="badge">📖 Tintinalli</span>
<span class="badge">🦴 Rockwood & Green</span>
</div>
</div>
<!-- ══════════ ROW 1: Definition + Overview ══════════ -->
<div class="grid-2">
<div class="card card-blue">
<div class="section-title"><span>📘</span> Definition & Overview</div>
<ul class="dot-list">
<li><strong>Acute Spinal Cord Injury (SCI):</strong> Traumatic insult to the spinal cord causing transient or permanent motor, sensory, and/or autonomic dysfunction below the level of injury</li>
<li><strong>Spinal column injury ≠ SCI</strong> — vertebral fracture/dislocation may or may not injure the cord</li>
<li><strong>Incidence:</strong> ~54 cases per million/year in USA; ~18,000 new cases/year</li>
<li><strong>Demographics:</strong> Males ~80% (4:1 M:F ratio); peak age = late teens to 20s; mean age is increasing as population ages</li>
<li><strong>Most common level:</strong> Cervical > Thoracic > Lumbar</li>
</ul>
<div class="alert alert-blue">
<span class="ai">💡</span>
<div>SCI is commonly <strong>comorbid with multiorgan injury</strong>. Assess with standard ATLS protocol — Airway, Breathing, Circulation FIRST before neurologic evaluation.</div>
</div>
</div>
<div class="card card-red">
<div class="section-title"><span>⚡</span> Causes / Risk Factors / Mechanisms</div>
<div class="sh">Common Causes (in order)</div>
<div style="display:flex;flex-wrap:wrap;gap:3px;margin-bottom:6px;">
<span class="pill pill-red">🚗 MVA ~38%</span>
<span class="pill pill-orange">🤸 Falls ~31%</span>
<span class="pill pill-blue">🔫 Violence ~14%</span>
<span class="pill pill-teal">🏊 Sports/Recreation ~9%</span>
<span class="pill pill-purple">🏥 Medical/Surgical ~4%</span>
</div>
<div class="sh">Mechanism by Level</div>
<table class="info-table">
<thead><tr><th class="th-red">Level</th><th class="th-red">Mechanism</th><th class="th-red">Classic Injury Pattern</th></tr></thead>
<tbody class="tr-alt">
<tr><td><strong>C-spine</strong></td><td>Flexion, Extension, Rotation, Axial load</td><td>Jefferson (C1), Odontoid (C2), Hangman (C2)</td></tr>
<tr><td><strong>T-spine</strong></td><td>High-energy axial load/flexion</td><td>Chance fracture (seatbelt), burst fracture</td></tr>
<tr><td><strong>L-spine</strong></td><td>Axial compression, hyperflexion</td><td>Burst fracture, Chance fracture</td></tr>
<tr><td><strong>Penetrating</strong></td><td>GSW, stabbing</td><td>Brown-Séquard syndrome (hemisection)</td></tr>
</tbody>
</table>
<div class="alert alert-orange" style="margin-top:6px;">
<span class="ai">⚠️</span>
<span><strong>10–40% of SCI patients have MULTIPLE noncontiguous fractures</strong> — always image entire spine if one level is found!</span>
</div>
</div>
</div>
<!-- ══════════ ROW 2: Pathophysiology ══════════ -->
<div class="grid-full">
<div class="card card-purple">
<div class="section-title"><span>⚙️</span> Pathophysiology — Primary vs Secondary Injury</div>
<div style="display:grid; grid-template-columns: 1fr 1fr 3fr; gap:10px; align-items:start;">
<div>
<div class="sh">Primary Injury</div>
<ul class="dot-list">
<li>Direct mechanical disruption</li>
<li>Compression by bony fragments, disc, hematoma</li>
<li>Laceration / Transection</li>
<li>Irreversible in complete SCI</li>
</ul>
</div>
<div>
<div class="sh">Secondary Injury (treatable target)</div>
<ul class="dot-list">
<li>⏱ <strong>0–2 hrs:</strong> Arteriolar disruption → grey matter ischemia</li>
<li>⏱ <strong>2–48 hrs:</strong> Cytokine release, inflammation, apoptosis</li>
<li>⏱ <strong>Up to 3 weeks:</strong> Ongoing apoptotic cell death</li>
<li>Ion dysregulation, glutamate excitotoxicity, ROS</li>
<li>Loss of autoregulation → watershed ischemia</li>
</ul>
</div>
<div>
<div class="sh">Secondary Injury Cascade Flowchart</div>
<div class="flow" style="flex-direction:column; align-items:flex-start; gap:3px;">
<div style="display:flex; align-items:center; gap:5px;">
<div class="fbox" style="color:#7c3aed; background:#faf5ff;">Mechanical Trauma</div>
<div class="farr">→</div>
<div class="fbox" style="color:#dc2626; background:#fff1f2;">Vascular Disruption + ↓ O₂</div>
<div class="farr">→</div>
<div class="fbox" style="color:#b91c1c; background:#fee2e2;">Grey Matter Ischemia (0–2h)</div>
</div>
<div style="display:flex; align-items:center; gap:5px; margin-left:10px;">
<div class="farr">↓</div>
</div>
<div style="display:flex; align-items:center; gap:5px;">
<div class="fbox" style="color:#ea580c; background:#fff7ed;">↑ Cytokines + Inflammation</div>
<div class="farr">→</div>
<div class="fbox" style="color:#c2410c; background:#ffedd5;">Apoptosis (24–48h)</div>
<div class="farr">→</div>
<div class="fbox" style="color:#ca8a04; background:#fefce8;">Glial Scar Formation (weeks)</div>
</div>
</div>
<div class="alert alert-yellow" style="margin-top:6px;">
<span class="ai">🎯</span>
<span><strong>Clinical relevance:</strong> Preventing hypotension (SBP <90 mmHg) and hypoxia is the most impactful emergency intervention — both worsen secondary injury dramatically.</span>
</div>
</div>
</div>
</div>
</div>
<div class="divider"></div>
<!-- ══════════ ROW 3: ASIA Scale + Incomplete Syndromes ══════════ -->
<div class="grid-2">
<!-- ASIA CLASSIFICATION -->
<div class="card card-teal">
<div class="section-title"><span>📊</span> ASIA Impairment Scale (AIS)</div>
<div style="font-size:9.5px; color:#0f766e; margin-bottom:6px; font-style:italic;">American Spinal Injury Association — Gold standard neurological classification</div>
<table class="info-table">
<thead><tr><th class="th-teal">Grade</th><th class="th-teal">Name</th><th class="th-teal">Definition</th><th class="th-teal">Prognosis</th></tr></thead>
<tbody>
<tr style="background:#fff1f2"><td><span style="font-size:18px; font-weight:900; color:#dc2626;">A</span></td><td><strong>Complete</strong></td><td>No motor OR sensory function in S4–S5</td><td><span class="verdict vpoor">Poor</span></td></tr>
<tr style="background:#fff7ed"><td><span style="font-size:18px; font-weight:900; color:#ea580c;">B</span></td><td><strong>Sensory Incomplete</strong></td><td>Sensory preserved, NO motor below NLI, including S4–S5</td><td><span class="verdict vmod">Moderate</span></td></tr>
<tr style="background:#fefce8"><td><span style="font-size:18px; font-weight:900; color:#ca8a04;">C</span></td><td><strong>Motor Incomplete</strong></td><td>Motor preserved below NLI; >50% key muscles Grade <3</td><td><span class="verdict vmod">Variable</span></td></tr>
<tr style="background:#f0fdf4"><td><span style="font-size:18px; font-weight:900; color:#16a34a;">D</span></td><td><strong>Motor Incomplete</strong></td><td>Motor preserved; >50% key muscles Grade ≥3</td><td><span class="verdict vgood">Good</span></td></tr>
<tr style="background:#eff6ff"><td><span style="font-size:18px; font-weight:900; color:#2563eb;">E</span></td><td><strong>Normal</strong></td><td>Normal motor and sensory function</td><td><span class="verdict vgood">Excellent</span></td></tr>
</tbody>
</table>
<div class="alert alert-yellow" style="margin-top:7px;">
<span class="ai">⚠️</span>
<div><strong>SACRAL SPARING = Key for Complete vs Incomplete:</strong><br>
Check <strong>S4-S5</strong> — any perianal sensation or voluntary anal contraction = INCOMPLETE injury (prognostically much better!)</div>
</div>
<div class="alert alert-blue" style="margin-top:5px;">
<span class="ai">📌</span>
<span>ASIA motor scale: 0 to 5 per key muscle group. <strong>10 key muscles</strong> tested each side; max score = 100.</span>
</div>
</div>
<!-- INCOMPLETE SYNDROMES -->
<div class="card card-orange">
<div class="section-title"><span>🧩</span> Incomplete SCI Syndromes</div>
<div style="font-size:9.5px; color:#c2410c; margin-bottom:6px; font-style:italic;">~90% of incomplete injuries fit one of these three major patterns (Rosen's EM)</div>
<div class="syndrome-grid">
<div class="syn-card syn-central">
<div class="syn-title">🔴 Central Cord Syndrome</div>
<div class="syn-body">
<strong>Most common</strong> (~9% all SCI; ~50% incomplete)<br>
<strong>Mechanism:</strong> Hyperextension injury in elderly with cervical spondylosis; degenerative arthritis<br>
<strong>Features:</strong> Arms >> Legs weakness; variable sensory loss; bladder dysfunction (retention)<br>
<strong>Prognosis:</strong> <span class="verdict vmod">Moderate</span> — ~80% regain walking ability<br>
<strong>Key:</strong> Face spared
</div>
</div>
<div class="syn-card syn-brown">
<div class="syn-title">🟣 Brown-Séquard Syndrome</div>
<div class="syn-body">
<strong>Mechanism:</strong> Hemisection of cord; classic = penetrating injury (GSW, stab)<br>
<strong>IPSILATERAL:</strong> Motor paralysis + vibration/proprioception loss (dorsal columns)<br>
<strong>CONTRALATERAL:</strong> Pain & temperature loss (spinothalamic) — 1–2 levels below<br>
<strong>Prognosis:</strong> <span class="verdict vgood">Best</span> of all syndromes
</div>
</div>
<div class="syn-card syn-ant">
<div class="syn-title">🔴 Anterior Cord Syndrome</div>
<div class="syn-body">
<strong>Mechanism:</strong> Flexion injury; disc herniation; aortic surgery; anterior spinal artery territory<br>
<strong>LOST:</strong> Motor (corticospinal) + Pain & Temperature (spinothalamic)<br>
<strong>SPARED:</strong> Vibration + Proprioception (posterior columns)<br>
<strong>Prognosis:</strong> <span class="verdict vpoor">Worst</span> — <10% motor recovery
</div>
</div>
<div class="syn-card syn-post">
<div class="syn-title">🟢 Posterior Cord Syndrome</div>
<div class="syn-body">
<strong>Rare</strong>; hyperextension + posterior column injury<br>
<strong>LOST:</strong> Vibration, Proprioception, Light touch<br>
<strong>SPARED:</strong> Pain & Temperature; Motor intact<br>
<strong>Presents:</strong> Sensory ataxia (wide-based gait), loss of position sense
</div>
</div>
<div class="syn-card syn-conus">
<div class="syn-title">🟣 Conus Medullaris Syndrome</div>
<div class="syn-body">
<strong>Level:</strong> T12–L1 burst fracture; injury to sacral cord (S2–S5)<br>
<strong>Mixed UMN + LMN features</strong><br>
Paraparesis + saddle anesthesia + bowel/bladder dysfunction + impotence<br>
<strong>Perianal sensation usually SPARED</strong>
</div>
</div>
<div class="syn-card syn-cauda">
<div class="syn-title">🟡 Cauda Equina Syndrome</div>
<div class="syn-body">
<strong>SURGICAL EMERGENCY</strong> — nerve roots, NOT cord<br>
<strong>Saddle anesthesia</strong> (S3–S5) + bowel/bladder dysfunction<br>
LMN pattern: flaccid weakness, absent reflexes<br>
<strong>Prognosis:</strong> <span class="verdict vgood">Better than cord</span> (LMN resilience)<br>
<strong>MRI STAT → surgery within 24–48h</strong>
</div>
</div>
</div>
</div>
</div>
<!-- ══════════ ROW 4: Clinical Features + Neurogenic/Spinal Shock ══════════ -->
<div class="grid-2">
<div class="card card-indigo">
<div class="section-title"><span>🩺</span> Clinical Features</div>
<div class="sh">Red Flag Signs of SCI (Overt)</div>
<ul class="dot-list">
<li>🦽 <strong>Flaccid paralysis</strong> below level of injury (acute phase)</li>
<li>😶 <strong>Sensory loss</strong> — pain, temperature, light touch, proprioception</li>
<li>💉 <strong>Priapism</strong> — pathognomonic of SCI in male trauma patients!</li>
<li>🫁 <strong>Paradoxical breathing</strong> — diaphragm active, intercostals paralyzed (C3–C5 injury)</li>
<li>💓 <strong>Bradycardia + Hypotension</strong> — neurogenic shock (above T6)</li>
<li>🌡️ <strong>Poikilothermia</strong> — inability to regulate temperature</li>
<li>🧠 <strong>Loss of tendon reflexes</strong> below level (spinal shock phase)</li>
</ul>
<div class="sh">Level-Specific Features (Memory Aid)</div>
<table class="info-table">
<thead><tr><th class="th-indigo">Level</th><th class="th-indigo">Respiratory</th><th class="th-indigo">Key Deficit</th></tr></thead>
<tbody class="tr-alt">
<tr><td>C3–C4</td><td style="color:#dc2626;">Ventilator dependent</td><td>Quadriplegia; diaphragm loss</td></tr>
<tr><td>C5</td><td style="color:#ea580c;">Partial ventilation</td><td>Elbow flexion present; wrist ext gone</td></tr>
<tr><td>C6</td><td style="color:#ca8a04;">Intact</td><td>Wrist ext present; hand grip absent</td></tr>
<tr><td>C7</td><td style="color:#16a34a;">Intact</td><td>Elbow ext present; finger ext absent</td></tr>
<tr><td>T1–T12</td><td style="color:#16a34a;">Intact</td><td>Paraplegia; intercostal loss varies</td></tr>
<tr><td>L1–S1</td><td style="color:#16a34a;">Intact</td><td>Hip/knee weakness; cauda equina risk</td></tr>
</tbody>
</table>
</div>
<div class="card card-crimson">
<div class="section-title"><span>⚡</span> Neurogenic Shock vs Spinal Shock</div>
<table class="info-table">
<thead><tr><th class="th-red">Feature</th><th class="th-red">Neurogenic Shock</th><th class="th-red">Spinal Shock</th></tr></thead>
<tbody class="tr-alt">
<tr><td><strong>Definition</strong></td><td>Hemodynamic instability from loss of sympathetic tone</td><td>Loss of all spinal reflexes below injury level</td></tr>
<tr><td><strong>Mechanism</strong></td><td>↓ SVR (vasodilation) ± ↓ HR (vagal dominance)</td><td>Temporary physiologic silence of cord below injury</td></tr>
<tr><td><strong>Level</strong></td><td>Above T6 (interrupts T1–L2 sympathetic chain)</td><td>Any level</td></tr>
<tr><td><strong>BP</strong></td><td style="color:#dc2626;">↓ Hypotension</td><td>Normal</td></tr>
<tr><td><strong>HR</strong></td><td style="color:#dc2626;">↓ Bradycardia (paradoxical!)</td><td>Normal</td></tr>
<tr><td><strong>Skin</strong></td><td>Warm, flushed (vasodilated)</td><td>Variable</td></tr>
<tr><td><strong>Duration</strong></td><td>Days to weeks</td><td>1–24 hours (reflexes return)</td></tr>
<tr><td><strong>Reflexes</strong></td><td>Absent (initially)</td><td>Absent then hyperreflexia returns</td></tr>
<tr><td><strong>Incidence</strong></td><td>7–20% of SCI</td><td>All complete SCIs initially</td></tr>
<tr><td><strong>Rx</strong></td><td>IV fluids (cautious) + Vasopressors (Norepinephrine/Phenylephrine)</td><td>No specific treatment; time-based resolution</td></tr>
</tbody>
</table>
<div class="alert alert-red" style="margin-top:6px;">
<span class="ai">🚨</span>
<div><strong>CRITICAL PEARL:</strong> Neurogenic shock = <strong>bradycardia + hypotension</strong>. Hypovolemic shock = <strong>tachycardia + hypotension</strong>. Distinguish them — giving excessive fluids in neurogenic shock worsens pulmonary edema!</div>
</div>
<div class="alert alert-orange" style="margin-top:5px;">
<span class="ai">⚠️</span>
<span><strong>Bulbocavernosus reflex return = end of spinal shock.</strong> Any deficit remaining after this point reflects true neurological injury.</span>
</div>
</div>
</div>
<div class="divider"></div>
<!-- ══════════ ROW 5: Diagnosis / Imaging ══════════ -->
<div class="grid-2">
<div class="card card-blue">
<div class="section-title"><span>🔬</span> Diagnosis & Imaging Decision Rules</div>
<div class="criteria-box">
<div class="ctitle">🟦 NEXUS Low-Risk Criteria — ALL 5 must be present to CLEAR c-spine without imaging</div>
<ul>
<li>No midline cervical tenderness</li>
<li>No focal neurologic deficit</li>
<li>Normal alertness / mental status</li>
<li>No intoxication</li>
<li>No painful distracting injury</li>
</ul>
<div style="margin-top:5px; font-size:9.5px; color:#1d4ed8;"><strong>Sensitivity 99.6%, NPV 99.8%</strong></div>
</div>
<div class="criteria-box" style="border-color:#7c3aed; margin-top:7px;">
<div class="ctitle" style="color:#6d28d9;">🟣 Canadian C-Spine Rule (CCR) — 3 Questions</div>
<ul>
<li><strong>Q1:</strong> Any HIGH-RISK factor? → Age ≥65, dangerous mechanism, paresthesias → Image</li>
<li><strong>Q2:</strong> Any LOW-RISK factor? → Simple rear-end MVC, ambulatory, delayed onset, no midline tenderness → can assess ROM</li>
<li><strong>Q3:</strong> Can patient actively rotate neck 45° L & R? → No imaging needed</li>
</ul>
<div style="margin-top:5px; font-size:9.5px; color:#6d28d9;"><strong>Sensitivity 99.4%, Specificity 45.1%</strong> — more specific than NEXUS</div>
</div>
<div class="alert alert-blue" style="margin-top:7px;">
<span class="ai">💡</span>
<span>CCR is <strong>more specific</strong> (fewer unnecessary scans) than NEXUS. Both have similar sensitivity. NEXUS is easier to apply at bedside.</span>
</div>
</div>
<div class="card card-green">
<div class="section-title"><span>📷</span> Imaging Modalities</div>
<div class="step"><div class="snum sn-blue">1</div><div class="stxt"><strong>CT Scan — Investigation of Choice (acute trauma)</strong><br>More sensitive/specific than X-ray for vertebral fracture/dislocation. <span style="color:#dc2626;font-weight:700">If high-quality CT available → X-ray NOT required for c-spine</span>. Must image ENTIRE spine if one fracture found (10–40% multiple levels).</div></div>
<div class="step"><div class="snum sn-blue">2</div><div class="stxt"><strong>MRI — Best for cord, ligament, disc, vascular injury</strong><br>Identifies epidural hematoma, disc herniation, cord edema/hemorrhage. Recommended when: (a) neuro deficit without CT finding, (b) pre-surgical planning, (c) SCIWORA. Best prognostication tool. Time-intensive — challenging in acute trauma.</div></div>
<div class="step"><div class="snum sn-blue">3</div><div class="stxt"><strong>Plain X-Ray (3 views) — When CT unavailable</strong><br>AP + Lateral + Odontoid views for c-spine. Limited sensitivity. Level 1 evidence supports if CT unavailable.</div></div>
<div class="sh" style="margin-top:8px;">SCIWORA — Spinal Cord Injury Without Radiographic Abnormality</div>
<ul class="dot-list">
<li>Presents almost exclusively in <strong>children</strong></li>
<li>Normal CT + X-ray; MRI may show cord changes</li>
<li>Both complete and incomplete SCI can occur as SCIWORA</li>
<li>Current definition: abnormal on MRI but not CT/X-ray</li>
</ul>
<div class="alert alert-yellow" style="margin-top:5px;">
<span class="ai">⭐</span>
<span><strong>MRI findings predict prognosis:</strong> Cord hemorrhage = poor outcome. Cord edema alone = better recovery potential.</span>
</div>
</div>
</div>
<!-- ══════════ ROW 6: Management ══════════ -->
<div class="grid-full">
<div class="card card-dark">
<div class="section-title"><span>💊</span> Management — Emergency to Surgical</div>
<div style="display:grid; grid-template-columns: 1fr 1fr 1fr; gap:10px;">
<div>
<div class="sh">🚨 IMMEDIATE (Primary Survey — ATLS)</div>
<div class="step"><div class="snum sn-red">A</div><div class="stxt" style="color:#cbd5e1;"><strong>Airway</strong> — Inline cervical stabilization; RSI for GCS ≤8; C3–4 → anticipate resp failure; video laryngoscopy preferred</div></div>
<div class="step"><div class="snum sn-red">B</div><div class="stxt" style="color:#cbd5e1;"><strong>Breathing</strong> — O₂ supplementation; monitor SpO₂ >95%; paradoxical breathing = cord above T6</div></div>
<div class="step"><div class="snum sn-red">C</div><div class="stxt" style="color:#cbd5e1;"><strong>Circulation</strong> — Avoid SBP <90 mmHg (target MAP 85–90 mmHg for 7 days in cervical/thoracic SCI). IV access ×2, crystalloid cautiously. Vasopressors for neurogenic shock.</div></div>
<div class="step"><div class="snum sn-red">D</div><div class="stxt" style="color:#cbd5e1;"><strong>Disability</strong> — GCS, pupils, ASIA grading, dermatome/myotome testing</div></div>
<div class="step"><div class="snum sn-red">E</div><div class="stxt" style="color:#cbd5e1;"><strong>Exposure/Immobilization</strong> — Rigid cervical collar; backboard transfer; log-roll ONLY with inline stabilization</div></div>
</div>
<div>
<div class="sh">🏥 SECONDARY MANAGEMENT</div>
<ul class="dot-list" style="color:#cbd5e1;">
<li><strong>Immobilization:</strong> Hard cervical collar until cleared; rigid backboard during transport</li>
<li><strong>MAP Target:</strong> 85–90 mmHg for 7 days (neuroprotective)</li>
<li><strong>Vasopressors:</strong> Norepinephrine 1st choice; Phenylephrine for bradycardia-predominant; Dopamine alternative</li>
<li><strong>Foley catheter:</strong> Neurogenic bladder; strict I&O monitoring</li>
<li><strong>Bowel regimen:</strong> Prevent ileus and autonomic dysreflexia triggers</li>
<li><strong>DVT prophylaxis:</strong> LMWH + sequential compression (high VTE risk)</li>
<li><strong>PPI/H2RA:</strong> Prevent stress ulcer (Cushing ulcer)</li>
<li><strong>Pressure ulcer prevention:</strong> Turn every 2 hours</li>
<li><strong>Transfer:</strong> Specialized SCI center → improved outcomes</li>
</ul>
</div>
<div>
<div class="sh">💉 Methylprednisolone (MPSS) — Controversial</div>
<div style="background:rgba(251,191,36,0.12); border:1px solid rgba(251,191,36,0.3); border-radius:8px; padding:8px 10px; margin-bottom:7px;">
<div style="color:#fbbf24; font-size:9.5px; font-weight:700; margin-bottom:4px;">NASCIS III / AOSPine 2017 Protocol</div>
<ul class="dot-list" style="color:#e2e8f0;">
<li>Consider ONLY if started within <strong>8 hours of injury</strong></li>
<li>30 mg/kg IV bolus over 15 min → then 5.4 mg/kg/h × 23h</li>
<li>DO NOT give after 8 hours (risks outweigh benefits)</li>
<li>DO NOT use 48-hour infusion</li>
</ul>
<div style="color:#fca5a5; font-size:9.5px; font-weight:700; margin-top:5px;">⚠️ AAN recommends AGAINST routine use — risk of GI hemorrhage + respiratory infection without proven functional benefit</div>
</div>
<div class="sh">🔪 Surgical Indications</div>
<ul class="dot-list" style="color:#cbd5e1;">
<li>Cord compression with incomplete deficit (urgent)</li>
<li>Cauda equina syndrome → <strong>surgery within 24–48h</strong></li>
<li>Unstable spinal fracture with neurological progression</li>
<li>STASCIS trial: early decompression <24h → better ASIA grade improvement</li>
</ul>
</div>
</div>
</div>
</div>
<!-- ══════════ ROW 7: Autonomic Dysreflexia + Complications ══════════ -->
<div class="grid-2">
<div class="card card-red">
<div class="section-title"><span>⚡</span> Autonomic Dysreflexia — Life-Threatening Emergency</div>
<div class="alert alert-red">
<span class="ai">🆘</span>
<div><strong>POTENTIALLY FATAL — unique to SCI patients</strong><br>
Occurs in up to 56% of patients with lesions ABOVE T5–T6</div>
</div>
<div class="sh">Triggers (afferent stimuli from hollow viscera)</div>
<div style="display:flex; flex-wrap:wrap; gap:3px; margin-bottom:5px;">
<span class="pill pill-red">🚽 Bladder distension (most common)</span>
<span class="pill pill-orange">💩 Bowel impaction</span>
<span class="pill pill-purple">🤰 Uterine contractions</span>
<span class="pill pill-teal">💊 Tight clothing/pressure sores</span>
<span class="pill pill-blue">🩺 Catheterization</span>
</div>
<div class="sh">Clinical Features</div>
<ul class="dot-list">
<li>🔴 <strong>Paroxysmal severe hypertension</strong> — may be >200/100 mmHg</li>
<li>💆 Pounding headache (most common symptom)</li>
<li>💓 Paradoxical bradycardia (baroreceptor reflex)</li>
<li>🌊 Flushing + diaphoresis ABOVE level of injury</li>
<li>🧊 Pallor + piloerection BELOW level of injury</li>
<li>👃 Nasal congestion, blurred vision, anxiety</li>
</ul>
<div class="sh">Treatment — REMOVE THE TRIGGER FIRST</div>
<div class="step"><div class="snum sn-red">1</div><div class="stxt"><strong>Sit patient upright</strong> (orthostatic BP drop helps)</div></div>
<div class="step"><div class="snum sn-red">2</div><div class="stxt"><strong>Loosen clothing</strong>, check for pressure points</div></div>
<div class="step"><div class="snum sn-red">3</div><div class="stxt"><strong>Bladder:</strong> Catheterize or check/irrigate blocked catheter (most common trigger)</div></div>
<div class="step"><div class="snum sn-red">4</div><div class="stxt"><strong>Bowel:</strong> Digital rectal exam → disimpact (use lidocaine gel)</div></div>
<div class="step"><div class="snum sn-red">5</div><div class="stxt"><strong>Pharmacological:</strong> Nitrates (sublingual/topical) or Nifedipine if HTN persists</div></div>
<div class="step"><div class="snum sn-red">6</div><div class="stxt"><strong>In labor:</strong> Regional anesthesia (spinal/epidural) eliminates dysreflexia triggers</div></div>
</div>
<div class="card card-yellow">
<div class="section-title"><span>⚠️</span> Complications — Acute & Long-Term</div>
<div class="sh">Acute Complications (ICU Phase)</div>
<ul class="dot-list">
<li>🫁 <strong>Respiratory failure</strong> — #1 cause of death; C3–C5 = ventilator-dependent</li>
<li>💉 <strong>Neurogenic shock</strong> — hypotension + bradycardia; requires vasopressors</li>
<li>⚡ <strong>Spinal shock</strong> — flaccid paralysis, absent reflexes, atonic bladder</li>
<li>🤢 <strong>Dysphagia</strong> — aspiration risk, especially c-spine injury</li>
<li>🧪 <strong>Stress ulcers</strong> (Cushing ulcer) — prophylaxis mandatory</li>
<li>🦵 <strong>DVT/PE</strong> — highest VTE risk of any trauma; LMWH + SCD</li>
</ul>
<div class="sh">Subacute/Chronic Complications</div>
<ul class="dot-list">
<li>🔄 <strong>Spasticity</strong> — UMN pattern after spinal shock resolves; treat with baclofen</li>
<li>🚽 <strong>Neurogenic bladder</strong> — urinary retention → recurrent UTI; intermittent catheterization</li>
<li>💩 <strong>Neurogenic bowel</strong> — constipation, impaction → autonomic dysreflexia trigger</li>
<li>🩹 <strong>Pressure ulcers</strong> — over sacrum, heels, occiput; reposition q2h</li>
<li>🌡️ <strong>Thermoregulatory failure</strong> — poikilothermia; risk of hyperthermia/hypothermia</li>
<li>🦴 <strong>Heterotopic ossification</strong> — ectopic bone around joints; ↑ alkaline phosphatase</li>
<li>🧠 <strong>Autonomic dysreflexia</strong> — above T6; life-threatening hypertensive emergency</li>
<li>💀 <strong>Psychiatric:</strong> Depression, anxiety, PTSD — major quality-of-life impact</li>
</ul>
</div>
</div>
<div class="divider"></div>
<!-- ══════════ ROW 8: High-Yield Pearls + Mnemonics ══════════ -->
<div class="grid-2">
<div class="card card-green">
<div class="section-title"><span>💎</span> High-Yield Exam Pearls</div>
<div class="pearl" style="margin-top:12px;">
<p><strong>PEARL 1:</strong> PRIAPISM in a trauma patient = SCI until proven otherwise. Always examine perineum in polytrauma.</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 2:</strong> Central Cord Syndrome = ARMS weaker than LEGS. Classic: elderly with neck hyperextension (minor injury, degenerative spine). Most common incomplete SCI syndrome.</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 3:</strong> Brown-Séquard = BEST prognosis. Anterior Cord = WORST prognosis (<10% motor recovery). Know these for any exam question!</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 4:</strong> Sacral sparing (S4–S5) = INCOMPLETE injury = much better prognosis. ALWAYS check perianal sensation + voluntary anal contraction.</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 5:</strong> SCIWORA = almost exclusively in CHILDREN. Normal CT/X-ray but abnormal MRI. Flexible pediatric ligaments allow cord injury without bony injury.</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 6:</strong> Cauda Equina = SADDLE ANESTHESIA + bilateral leg weakness + bladder/bowel dysfunction. LMN lesion → FLACCID. SURGICAL EMERGENCY — MRI STAT.</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 7:</strong> Methylprednisolone — ONLY within 8 hours, and highly controversial. AAN says avoid. AOSPine says CONSIDER. Know both perspectives for MCQs.</p>
</div>
</div>
<div class="card card-purple">
<div class="section-title"><span>🧠</span> Memory Tricks & Mnemonics</div>
<div class="mnemonic" style="margin-bottom:9px;">
<div class="mtitle">🧠 Incomplete SCI Syndromes — "CAB + P" (Central, Anterior, Brown, Posterior)</div>
<div class="letters">
<div class="lb"><strong>C</strong>entral — Arms > Legs; Hyperextension elderly; Best common incomplete</div>
<div class="lb"><strong>A</strong>nterior — Motor GONE + Pain/Temp GONE; Vibration SAVED; Worst prognosis</div>
<div class="lb"><strong>B</strong>rown-Séquard — IPSIlateral motor; CONTRAlateral pain/temp; Best prognosis</div>
<div class="lb"><strong>P</strong>osterior — Vibration/Proprioception LOST; Sensory ataxia; Rare</div>
</div>
</div>
<div class="mnemonic" style="margin-bottom:9px;">
<div class="mtitle">🦴 NEXUS Criteria — "No Tender Neurological Nonsense in Intoxicated Distracting"</div>
<div class="letters">
<div class="lb"><strong>N</strong>o midline tenderness</div>
<div class="lb"><strong>N</strong>o focal neuro deficit</div>
<div class="lb"><strong>N</strong>ormal alertness</div>
<div class="lb"><strong>N</strong>o intoxication</div>
<div class="lb"><strong>N</strong>o distracting injury</div>
</div>
</div>
<div class="mnemonic" style="margin-bottom:9px;">
<div class="mtitle">🚨 Neurogenic Shock vs Hypovolemic Shock — "Brad vs Tachy"</div>
<div style="display:grid; grid-template-columns:1fr 1fr; gap:6px; margin-top:4px;">
<div style="background:rgba(251,191,36,0.12); border:1px solid rgba(251,191,36,0.3); border-radius:7px; padding:6px 9px;">
<div style="color:#fbbf24; font-size:9.5px; font-weight:700; margin-bottom:3px;">NEUROGENIC SHOCK</div>
<div style="font-size:9.5px; color:#e2e8f0;">↓ BP + <strong>↓ HR (bradycardia)</strong><br>Warm, flushed skin<br>SCI above T6<br>Rx: Vasopressors (NE)</div>
</div>
<div style="background:rgba(239,68,68,0.1); border:1px solid rgba(239,68,68,0.3); border-radius:7px; padding:6px 9px;">
<div style="color:#fca5a5; font-size:9.5px; font-weight:700; margin-bottom:3px;">HYPOVOLEMIC SHOCK</div>
<div style="font-size:9.5px; color:#e2e8f0;">↓ BP + <strong>↑ HR (tachycardia)</strong><br>Cold, clammy skin<br>Blood loss<br>Rx: Fluids + blood</div>
</div>
</div>
</div>
<div class="mnemonic">
<div class="mtitle">📋 Classic Cervical Fractures — "Jefferson HANGS from the Dens"</div>
<div class="letters">
<div class="lb"><strong>J</strong>efferson = C1 burst (axial load; "broke the ring"); <strong>STABLE</strong> — transverse lig determines</div>
<div class="lb"><strong>H</strong>angman = C2 pedicle fracture (bilateral); hyperextension/axial; often paradoxically stable</div>
<div class="lb"><strong>O</strong>dontoid = C2 dens fracture; Types I/II/III; Type II most common + unstable</div>
<div class="lb"><strong>C</strong>hance = T-L junction; seatbelt; "chance of getting it in rear-end collision"</div>
</div>
</div>
</div>
</div>
<!-- ══════════ ROW 9: Important Investigations + Comparison Table ══════════ -->
<div class="grid-2">
<div class="card card-slate">
<div class="section-title"><span>🧪</span> Important Investigations Summary</div>
<table class="info-table">
<thead><tr><th class="th-slate">Investigation</th><th class="th-slate">When & Why</th><th class="th-slate">Key Finding</th></tr></thead>
<tbody class="tr-alt">
<tr><td>🩻 <strong>CT Spine (entire)</strong></td><td>First-line in all trauma if NEXUS positive or CCR positive</td><td>Fracture/dislocation, cord compression</td></tr>
<tr><td>🧲 <strong>MRI Spine</strong></td><td>Deficit without CT finding; pre-op planning; SCIWORA; prognosis</td><td>Cord hemorrhage (bad) vs edema (better)</td></tr>
<tr><td>📋 <strong>3-View X-Ray</strong></td><td>When CT unavailable (AP + Lateral + Odontoid)</td><td>Limited sensitivity — use CT if possible</td></tr>
<tr><td>🩸 <strong>CBC, BMP, Coags</strong></td><td>All trauma patients; baseline before surgery</td><td>Anemia, coagulopathy, renal function</td></tr>
<tr><td>🫀 <strong>ECG / Cardiac monitoring</strong></td><td>Above T6 — arrhythmia, bradycardia, heart blocks</td><td>Sinus bradycardia, AV blocks</td></tr>
<tr><td>🫁 <strong>ABG + SpO₂</strong></td><td>Respiratory compromise; cervical SCI</td><td>Hypoxia, hypercarbia → intubate</td></tr>
<tr><td>🍼 <strong>Urinalysis + Foley</strong></td><td>All SCI — neurogenic bladder, UTI screening</td><td>Retention, hematuria</td></tr>
<tr><td>🦴 <strong>CXR + FAST</strong></td><td>Polytrauma — associated injuries</td><td>Pneumothorax, hemothorax, free fluid</td></tr>
</tbody>
</table>
</div>
<div class="card card-pink">
<div class="section-title"><span>⚖️</span> Quick Reference — SCI Syndrome Comparison</div>
<table class="info-table">
<thead><tr><th class="th-red" style="width:18%">Syndrome</th><th class="th-red">Motor</th><th class="th-red">Pain/Temp</th><th class="th-red">Vibration/Proprioception</th><th class="th-red">Prognosis</th></tr></thead>
<tbody>
<tr style="background:#eff6ff"><td><strong>Central Cord</strong></td><td>Arms > Legs</td><td>Variable loss</td><td>Usually preserved</td><td><span class="verdict vmod">Moderate</span></td></tr>
<tr style="background:#fdf2f8"><td><strong>Brown-Séquard</strong></td><td>Ipsilateral loss</td><td>Contralateral loss</td><td>Ipsilateral loss</td><td><span class="verdict vgood">Best</span></td></tr>
<tr style="background:#fff1f2"><td><strong>Anterior Cord</strong></td><td>Bilateral loss</td><td>Bilateral loss</td><td>SPARED ✓</td><td><span class="verdict vpoor">Worst</span></td></tr>
<tr style="background:#f0fdfa"><td><strong>Posterior Cord</strong></td><td>Intact</td><td>Intact ✓</td><td>Bilateral loss</td><td><span class="verdict vmod">Variable</span></td></tr>
<tr style="background:#faf5ff"><td><strong>Conus Medullaris</strong></td><td>Para+UMN+LMN</td><td>Saddle loss</td><td>Variable</td><td><span class="verdict vmod">Mixed</span></td></tr>
<tr style="background:#fefce8"><td><strong>Cauda Equina</strong></td><td>LMN (flaccid)</td><td>Saddle (S3–5)</td><td>Loss</td><td><span class="verdict vgood">Better (LMN)</span></td></tr>
</tbody>
</table>
<div class="alert alert-orange" style="margin-top:7px;">
<span class="ai">🎯</span>
<div><strong>KEY EXAM DISTINGUISHER:</strong><br>
• Anterior cord: vibration/proprioception SPARED (posterior columns intact)<br>
• Posterior cord: pain/temp SPARED (spinothalamic intact)<br>
• Brown-Séquard: DISSOCIATED sensory loss (each side has different deficits)</div>
</div>
</div>
</div>
<!-- ══════════ ROW 10: EM-Specific Quick Reference ══════════ -->
<div class="grid-3">
<div class="card card-red">
<div class="section-title"><span>🚨</span> Red Flags / Immediate Actions</div>
<div class="alert alert-red" style="margin-bottom:5px;">
<span class="ai">🆘</span>
<div>
<strong>Immediate Intubation if:</strong><br>
• C3–C4 injury (diaphragm at risk)<br>
• SpO₂ <90% despite O₂<br>
• GCS ≤8 or airway at risk<br>
• Paradoxical breathing pattern<br>
• Rapid respiratory deterioration
</div>
</div>
<ul class="dot-list">
<li>🔴 SBP <90 → MAP <85 → vasopressors NOW</li>
<li>🔴 Priapism → SCI until proven otherwise</li>
<li>🔴 Cauda equina signs → MRI STAT + surgical consult</li>
<li>🔴 New neuro deficit on exam → re-image immediately</li>
<li>🔴 Bulging bladder → catheterize (avoid autonomic dysreflexia)</li>
</ul>
</div>
<div class="card card-teal">
<div class="section-title"><span>💉</span> Vasopressor Choice in Neurogenic Shock</div>
<table class="info-table">
<thead><tr><th class="th-teal">Agent</th><th class="th-teal">Mechanism</th><th class="th-teal">Use When</th></tr></thead>
<tbody class="tr-alt">
<tr><td><strong>Norepinephrine</strong></td><td>α1 + β1; ↑ SVR + HR</td><td>1st line; low BP + low HR</td></tr>
<tr><td><strong>Phenylephrine</strong></td><td>Pure α1; ↑ SVR</td><td>When tachycardia also present</td></tr>
<tr><td><strong>Dopamine</strong></td><td>DA + β + α (dose-dependent)</td><td>Alternative; avoid high doses</td></tr>
<tr><td><strong>Atropine</strong></td><td>Anti-muscarinic; ↑ HR</td><td>Symptomatic bradycardia alone</td></tr>
</tbody>
</table>
<div class="alert alert-green" style="margin-top:6px;">
<span class="ai">🎯</span>
<span>MAP target: <strong>85–90 mmHg</strong> × 7 days post-injury (especially thoracic/cervical SCI) — maintains spinal cord perfusion pressure.</span>
</div>
</div>
<div class="card card-yellow">
<div class="section-title"><span>🌟</span> One-Liners for Exams</div>
<ul class="dot-list">
<li>🎯 Priapism in trauma → SCI</li>
<li>🎯 Paradoxical breathing → cervical SCI (C3–C5)</li>
<li>🎯 NEXUS: 5 criteria; all must be normal to clear</li>
<li>🎯 Central cord → elderly + hyperextension + spondylosis</li>
<li>🎯 Brown-Séquard → stab wound to back</li>
<li>🎯 Anterior cord → aortic surgery / disc herniation</li>
<li>🎯 Cauda equina → saddle anesthesia → MRI STAT</li>
<li>🎯 SCIWORA → children only</li>
<li>🎯 10–40% have multiple noncontiguous fractures → image whole spine</li>
<li>🎯 Neurogenic shock = bradycardia + hypotension (not tachy)</li>
<li>🎯 Sacral sparing = incomplete = better prognosis</li>
<li>🎯 Bulbocavernosus reflex return = end of spinal shock</li>
<li>🎯 MAP 85–90 mmHg × 7 days = neuroprotective target</li>
<li>🎯 MPSS = ONLY within 8 hours; controversial; consider carefully</li>
</ul>
</div>
</div>
<!-- ══════════ FOOTER ══════════ -->
<div class="footer">
<p>📚 Sources: <strong>Rosen's Emergency Medicine</strong> | <strong>Tintinalli's EM</strong> | <strong>Current Surgical Therapy 14e</strong> | <strong>Rockwood & Green's Fractures</strong> | <strong>Bailey & Love's Surgery</strong> | <strong>Bradley & Daroff's Neurology</strong></p>
<p>🚨 <strong>Emergency Medicine PGY-1 Reference</strong> | Acute Spine Injury | ✨ Orris AI</p>
</div>
</div>
</body>
</html>
ls -lh /tmp/workspace/spine-injury-poster/
Acute spinal cord injury medical diagram showing: cross-sectional view of spinal cord with color-coded injury syndrome patterns - Central Cord Syndrome (central gray area highlighted red, arms more affected), Brown-Sequard Syndrome (left half highlighted showing ipsilateral motor loss and contralateral pain/temperature loss), Anterior Cord Syndrome (anterior horn and spinothalamic tract highlighted, posterior columns spared), and Posterior Cord Syndrome (dorsal columns highlighted). Show anatomical tracts labeled: Corticospinal tract, Spinothalamic tract, Dorsal columns. Professional medical illustration style, white background, clean colors, labeled diagrams.
🦴 ACUTE SPINE INJURY — Emergency Medicine PGY-1 Master Sheet
📥 Download Your Poster
acute spine injury poster
HTML File · HTML
Open in any browser → Ctrl+P → Save as PDF (landscape orientation, scale to fit) for a print-ready study sheet.
🖼️ Spinal Cord Syndrome Anatomy Diagram
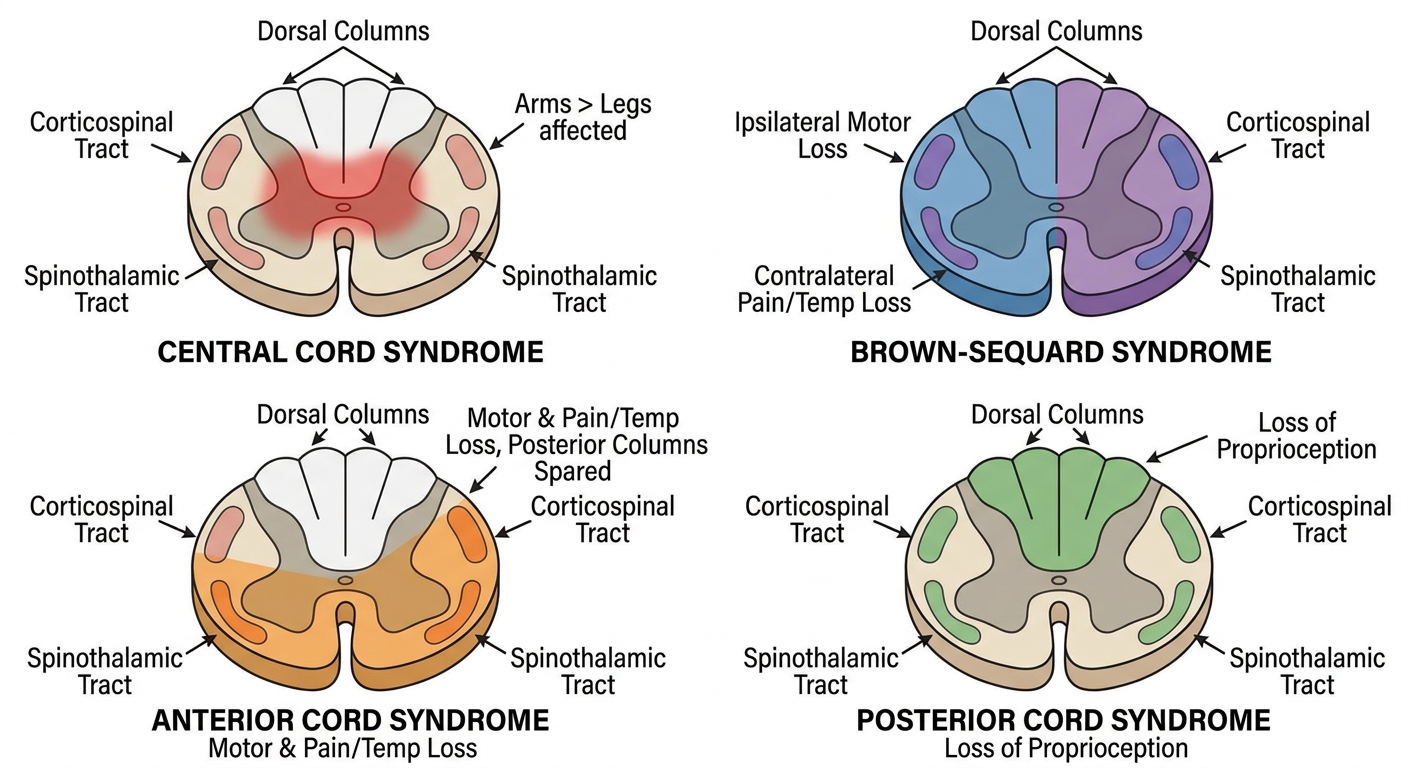
📋 What's Inside the Poster — All 12 Sections
| Section | Key Content |
|---|---|
| 📘 Definition & Overview | Incidence, demographics, scope |
| ⚡ Causes / Risk Factors | MVA 38%, Falls 31%, Penetrating; mechanism by level |
| ⚙️ Pathophysiology | Primary vs Secondary injury; cascade timeline |
| 📊 ASIA Impairment Scale | Grades A–E with prognosis; sacral sparing rule |
| 🧩 Incomplete SCI Syndromes | All 6 syndromes with mechanism, features, prognosis |
| 🩺 Clinical Features | Level-specific deficits, red flag signs |
| ⚡ Neurogenic vs Spinal Shock | Full comparison table — key EM differentiator |
| 🔬 Diagnosis | NEXUS criteria, Canadian C-Spine Rule, CT vs MRI |
| 💊 Management | ATLS approach, MAP targets, vasopressors, MPSS |
| ⚠️ Complications | Autonomic dysreflexia (emergency!), DVT, pressure sores |
| 💎 High-Yield Pearls | 7 exam-critical one-liners |
| 🧠 Mnemonics | CAB+P syndromes, NEXUS, Neurogenic vs Hypovolemic |
🔥 Top 5 Emergency Pearls
- Priapism in trauma = SCI until proven otherwise - always examine the perineum
- Neurogenic shock = bradycardia + hypotension (NOT tachycardia - key differentiator from hemorrhagic shock)
- Brown-Séquard = best prognosis; Anterior Cord = worst (<10% motor recovery)
- Sacral sparing (S4-S5) = incomplete injury - check perianal sensation in every SCI patient
- MAP 85-90 mmHg for 7 days = neuroprotective target post-SCI (most impactful ED intervention)
MASTER PROMPT TEMPLATE ✨ Create a clean high-yield medical infographic poster for emergency medicine pg resident 1st year about: NOR ADRENALINE Style: modern medical infographic highly organized exam-focused visually memorable colorful but professional easy to review before exams include emojis/icons for memory aid use clear section boxes and arrows use concise bullet points use tables for comparisons use color-coded categories include important high-yield notes and warning signs make it aesthetically pleasing like premium study notes white background readable font structured like a study cheat sheet Must include: Definition Classification Causes / risk factors Pathophysiology Clinical features Diagnosis Management Complications Important investigations High-yield exam pearls Memory tricks / mnemonics Comparison tables , ecgs, xrays, ct photos, mri photos if applicable
mkdir -p /tmp/workspace/noradrenaline-poster && echo "ready"
~/noradrenaline-poster/noradrenaline_poster.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<meta name="viewport" content="width=device-width, initial-scale=1.0">
<title>Noradrenaline (Norepinephrine) – Emergency Medicine High-Yield Infographic</title>
<style>
@import url('https://fonts.googleapis.com/css2?family=Inter:wght@300;400;500;600;700;800;900&family=Poppins:wght@400;600;700;800&display=swap');
* { margin: 0; padding: 0; box-sizing: border-box; }
body {
font-family: 'Inter', sans-serif;
background: #f1f5f9;
color: #0f172a;
font-size: 11px;
line-height: 1.5;
}
.page {
width: 1200px;
margin: 0 auto;
background: #ffffff;
padding: 20px 24px 28px;
}
/* ─── HEADER ─── */
.header {
background: linear-gradient(135deg, #0f172a 0%, #1e1b4b 30%, #7c3aed 65%, #dc2626 100%);
border-radius: 16px;
padding: 20px 28px;
display: flex;
align-items: center;
justify-content: space-between;
margin-bottom: 16px;
box-shadow: 0 8px 32px rgba(15,23,42,0.35);
position: relative;
overflow: hidden;
}
.header::after {
content: '⚡';
position: absolute;
right: 180px;
top: 50%;
transform: translateY(-50%);
font-size: 110px;
opacity: 0.06;
}
.header-left h1 {
font-family: 'Poppins', sans-serif;
font-size: 30px;
font-weight: 800;
color: #fff;
letter-spacing: -0.5px;
}
.header-left h1 span { color: #fbbf24; }
.header-left h1 .sub { color: #a5b4fc; font-size: 14px; font-weight: 500; margin-left: 8px; }
.header-left p { font-size: 11px; color: #c4b5fd; margin-top: 4px; font-weight: 500; }
.header-badges { display: flex; gap: 7px; flex-wrap: wrap; justify-content: flex-end; }
.badge { background: rgba(255,255,255,0.12); color: #fff; border: 1px solid rgba(255,255,255,0.25); border-radius: 20px; padding: 4px 12px; font-size: 9.5px; font-weight: 700; }
.badge.hot { background: rgba(251,191,36,0.2); border-color: #fbbf24; color: #fbbf24; }
.badge.em { background: rgba(239,68,68,0.2); border-color: #ef4444; color: #fca5a5; }
.badge.rx { background: rgba(167,139,250,0.2); border-color: #a78bfa; color: #c4b5fd; }
/* ─── GRIDS ─── */
.grid-3 { display: grid; grid-template-columns: 1fr 1fr 1fr; gap: 13px; margin-bottom: 13px; }
.grid-2 { display: grid; grid-template-columns: 1fr 1fr; gap: 13px; margin-bottom: 13px; }
.grid-2-1 { display: grid; grid-template-columns: 2fr 1fr; gap: 13px; margin-bottom: 13px; }
.grid-1-2 { display: grid; grid-template-columns: 1fr 2fr; gap: 13px; margin-bottom: 13px; }
.grid-full { margin-bottom: 13px; }
/* ─── CARDS ─── */
.card { border-radius: 12px; padding: 13px 15px; border: 1.5px solid transparent; position: relative; overflow: hidden; }
.card::before { content: ''; position: absolute; top: 0; left: 0; width: 4px; height: 100%; border-radius: 12px 0 0 12px; }
.card-blue { background: #eff6ff; border-color: #bfdbfe; } .card-blue::before { background: #2563eb; }
.card-green { background: #f0fdf4; border-color: #bbf7d0; } .card-green::before { background: #16a34a; }
.card-red { background: #fff1f2; border-color: #fecdd3; } .card-red::before { background: #dc2626; }
.card-purple { background: #faf5ff; border-color: #e9d5ff; } .card-purple::before { background: #7c3aed; }
.card-orange { background: #fff7ed; border-color: #fed7aa; } .card-orange::before { background: #ea580c; }
.card-teal { background: #f0fdfa; border-color: #99f6e4; } .card-teal::before { background: #0d9488; }
.card-yellow { background: #fefce8; border-color: #fde68a; } .card-yellow::before { background: #ca8a04; }
.card-pink { background: #fdf2f8; border-color: #f9a8d4; } .card-pink::before { background: #db2777; }
.card-indigo { background: #eef2ff; border-color: #c7d2fe; } .card-indigo::before { background: #4f46e5; }
.card-slate { background: #f8fafc; border-color: #cbd5e1; } .card-slate::before { background: #475569; }
.card-dark { background: #0f172a; border-color: #1e293b; color: #f8fafc; } .card-dark::before { background: #fbbf24; }
.card-crimson{ background: #fff0f0; border-color: #fca5a5; } .card-crimson::before{ background: #b91c1c; }
.card-violet { background: #f5f3ff; border-color: #ddd6fe; } .card-violet::before { background: #6d28d9; }
/* ─── SECTION TITLES ─── */
.st { font-family: 'Poppins', sans-serif; font-size: 11px; font-weight: 700; margin-bottom: 7px; display: flex; align-items: center; gap: 5px; text-transform: uppercase; letter-spacing: 0.6px; }
.card-blue .st { color: #1d4ed8; } .card-green .st { color: #15803d; } .card-red .st { color: #b91c1c; }
.card-purple .st { color: #6d28d9; } .card-orange .st { color: #c2410c; } .card-teal .st { color: #0f766e; }
.card-yellow .st { color: #92400e; } .card-pink .st { color: #be185d; } .card-indigo .st { color: #3730a3; }
.card-slate .st { color: #334155; } .card-dark .st { color: #fbbf24; } .card-crimson .st { color: #991b1b; }
.card-violet .st { color: #5b21b6; }
/* ─── LISTS ─── */
ul.dl { list-style: none; padding: 0; }
ul.dl li { padding: 2px 0 2px 14px; position: relative; font-size: 10.5px; color: #374151; }
ul.dl li::before { content: '▸'; position: absolute; left: 0; color: #6b7280; font-size: 9px; top: 3px; }
.card-dark ul.dl li { color: #cbd5e1; }
.card-dark ul.dl li::before { color: #fbbf24; }
/* ─── TABLES ─── */
table.t { width: 100%; border-collapse: collapse; font-size: 10px; margin-top: 4px; }
table.t th { padding: 5px 7px; font-weight: 700; text-align: left; font-size: 9.5px; text-transform: uppercase; letter-spacing: 0.3px; }
table.t td { padding: 4px 7px; border-bottom: 1px solid rgba(0,0,0,0.05); vertical-align: top; line-height: 1.4; }
table.t tr:last-child td { border-bottom: none; }
table.t tr:nth-child(even) td { background: rgba(0,0,0,0.022); }
.tb { background: #dbeafe; color: #1e3a8a; } .tg { background: #dcfce7; color: #14532d; }
.tr { background: #fee2e2; color: #7f1d1d; } .tp { background: #ede9fe; color: #4c1d95; }
.to { background: #fed7aa; color: #7c2d12; } .tt { background: #ccfbf1; color: #134e4a; }
.ts { background: #e2e8f0; color: #1e293b; } .td { background: #1e293b; color: #f8fafc; }
.ti { background: #e0e7ff; color: #312e81; } .ty { background: #fef3c7; color: #713f12; }
/* ─── PILLS ─── */
.pill { display: inline-block; padding: 2px 8px; border-radius: 20px; font-size: 9px; font-weight: 700; margin: 1px 2px; }
.pr { background: #fee2e2; color: #b91c1c; border: 1px solid #fca5a5; }
.pb { background: #dbeafe; color: #1d4ed8; border: 1px solid #93c5fd; }
.pg { background: #dcfce7; color: #15803d; border: 1px solid #86efac; }
.po { background: #ffedd5; color: #c2410c; border: 1px solid #fb923c; }
.pp { background: #ede9fe; color: #6d28d9; border: 1px solid #c4b5fd; }
.pt { background: #ccfbf1; color: #0f766e; border: 1px solid #5eead4; }
.py { background: #fef3c7; color: #92400e; border: 1px solid #fcd34d; }
.ppk { background: #fce7f3; color: #be185d; border: 1px solid #f9a8d4; }
/* ─── ALERTS ─── */
.al { border-radius: 8px; padding: 7px 11px; margin-top: 7px; font-size: 10px; font-weight: 600; display: flex; align-items: flex-start; gap: 6px; line-height: 1.5; }
.al-r { background: #fef2f2; border: 1.5px solid #ef4444; color: #991b1b; }
.al-y { background: #fefce8; border: 1.5px solid #eab308; color: #713f12; }
.al-b { background: #eff6ff; border: 1.5px solid #3b82f6; color: #1e3a8a; }
.al-g { background: #f0fdf4; border: 1.5px solid #22c55e; color: #14532d; }
.al-o { background: #fff7ed; border: 1.5px solid #f97316; color: #7c2d12; }
.al-p { background: #faf5ff; border: 1.5px solid #8b5cf6; color: #4c1d95; }
.ai { font-size: 14px; flex-shrink: 0; margin-top: 0; }
/* ─── MNEMONIC ─── */
.mn { background: linear-gradient(135deg, #0f172a, #1e293b); border-radius: 10px; padding: 9px 13px; margin-top: 7px; color: #f8fafc; }
.mn .mnt { font-family: 'Poppins', sans-serif; font-size: 9.5px; font-weight: 700; color: #fbbf24; text-transform: uppercase; letter-spacing: 0.6px; margin-bottom: 6px; }
.mn .lts { display: flex; flex-wrap: wrap; gap: 4px; }
.mn .lb { background: rgba(255,255,255,0.07); border: 1px solid rgba(251,191,36,0.25); border-radius: 6px; padding: 3px 8px; font-size: 10px; }
.mn .lb strong { color: #fbbf24; font-size: 12px; display: block; line-height: 1.2; }
/* ─── FLOW ─── */
.flow { display: flex; align-items: center; flex-wrap: wrap; gap: 4px; margin: 6px 0; }
.fb { border-radius: 7px; padding: 3px 9px; font-size: 9.5px; font-weight: 600; border: 1.5px solid currentColor; text-align: center; }
.fa { font-size: 16px; color: #6b7280; }
/* ─── PEARL ─── */
.pearl { background: linear-gradient(135deg, #f0fdf4, #dcfce7); border: 1.5px solid #16a34a; border-radius: 9px; padding: 7px 11px; margin-top: 8px; position: relative; }
.pearl::before { content: '💎'; position: absolute; top: -11px; left: 8px; font-size: 15px; }
.pearl p { font-size: 10px; color: #14532d; line-height: 1.5; }
/* ─── RECEPTOR BOX ─── */
.rec-grid { display: grid; grid-template-columns: 1fr 1fr; gap: 7px; margin-top: 6px; }
.rec-card { border-radius: 9px; padding: 7px 10px; border: 1.5px solid transparent; }
.rec-a1 { background: #fff1f2; border-color: #fca5a5; }
.rec-a2 { background: #fff7ed; border-color: #fdba74; }
.rec-b1 { background: #eff6ff; border-color: #93c5fd; }
.rec-b2 { background: #f0fdf4; border-color: #86efac; }
.rec-title { font-size: 10px; font-weight: 800; margin-bottom: 4px; }
.rec-a1 .rec-title { color: #b91c1c; }
.rec-a2 .rec-title { color: #c2410c; }
.rec-b1 .rec-title { color: #1d4ed8; }
.rec-b2 .rec-title { color: #15803d; }
.rec-body { font-size: 9.5px; color: #374151; line-height: 1.4; }
/* ─── STEP ─── */
.step { display: flex; gap: 7px; align-items: flex-start; padding: 3px 0; }
.snum { width: 17px; height: 17px; border-radius: 50%; display: flex; align-items: center; justify-content: center; font-size: 8.5px; font-weight: 800; flex-shrink: 0; }
.sr { background: #dc2626; color: #fff; }
.sb { background: #2563eb; color: #fff; }
.sg { background: #16a34a; color: #fff; }
.so { background: #ea580c; color: #fff; }
.sp { background: #7c3aed; color: #fff; }
.stxt { font-size: 10.5px; color: #374151; flex: 1; }
/* ─── SH ─── */
.sh { font-size: 9.5px; font-weight: 700; text-transform: uppercase; letter-spacing: 0.4px; margin: 7px 0 3px; opacity: 0.75; }
.card-blue .sh { color: #1d4ed8; } .card-green .sh { color: #15803d; } .card-red .sh { color: #b91c1c; }
.card-purple .sh { color: #6d28d9; } .card-orange .sh { color: #c2410c; } .card-teal .sh { color: #0f766e; }
.card-yellow .sh { color: #92400e; } .card-dark .sh { color: #fbbf24; } .card-crimson .sh { color: #991b1b; }
.card-indigo .sh { color: #3730a3; } .card-violet .sh { color: #5b21b6; } .card-slate .sh { color: #334155; }
/* ─── DIVIDER ─── */
.divider { height: 3px; background: linear-gradient(90deg, #dc2626, #ea580c, #fbbf24, #7c3aed, #2563eb, #16a34a); border-radius: 2px; margin: 13px 0; }
/* ─── BIG DRUG INFO BOX ─── */
.drug-header {
background: linear-gradient(135deg, #1e1b4b, #312e81);
border-radius: 10px;
padding: 10px 15px;
display: flex;
align-items: center;
gap: 14px;
margin-bottom: 8px;
}
.drug-emoji { font-size: 32px; }
.drug-name { font-family: 'Poppins', sans-serif; font-size: 20px; font-weight: 800; color: #fbbf24; }
.drug-alias { font-size: 10px; color: #c4b5fd; margin-top: 2px; }
.drug-class-tag { background: rgba(251,191,36,0.15); border: 1px solid rgba(251,191,36,0.3); color: #fbbf24; border-radius: 6px; padding: 3px 10px; font-size: 9.5px; font-weight: 700; }
/* ─── DOSING BOX ─── */
.dose-box {
background: #0f172a;
border: 2px solid #fbbf24;
border-radius: 10px;
padding: 10px 14px;
margin-top: 6px;
}
.dose-box .dt { font-family: 'Poppins', sans-serif; font-size: 10px; font-weight: 700; color: #fbbf24; text-transform: uppercase; letter-spacing: 0.5px; margin-bottom: 6px; }
.dose-row { display: flex; align-items: center; gap: 8px; padding: 3px 0; border-bottom: 1px solid rgba(255,255,255,0.07); }
.dose-row:last-child { border-bottom: none; }
.dose-label { font-size: 9.5px; color: #94a3b8; font-weight: 600; min-width: 100px; }
.dose-val { font-size: 11px; font-weight: 700; color: #fbbf24; }
.dose-note { font-size: 9px; color: #cbd5e1; margin-left: 4px; }
/* ─── FOOTER ─── */
.footer { background: #0f172a; border-radius: 10px; padding: 10px 20px; display: flex; justify-content: space-between; align-items: center; margin-top: 13px; }
.footer p { color: #94a3b8; font-size: 9.5px; }
.footer strong { color: #fbbf24; }
</style>
</head>
<body>
<div class="page">
<!-- ══════════ HEADER ══════════ -->
<div class="header">
<div class="header-left">
<h1>💊 <span>NORADRENALINE</span> <span class="sub">(Norepinephrine · Levophed)</span></h1>
<p>EMERGENCY MEDICINE PGY-1 | Vasopressor Master Reference | Lippincott Pharmacology · Tintinalli's · Rosen's EM · Goldman-Cecil · Harrison's · Fischer's Surgery</p>
</div>
<div class="header-badges">
<span class="badge hot">🔥 HIGH YIELD</span>
<span class="badge em">🚨 FIRST-LINE VASOPRESSOR</span>
<span class="badge rx">💊 Catecholamine</span>
<span class="badge">📚 Lippincott Pharm</span>
</div>
</div>
<!-- ══════════ ROW 1: Identity Card + Classification ══════════ -->
<div class="grid-2">
<!-- IDENTITY CARD -->
<div class="card card-violet">
<div class="st"><span>🪪</span> Drug Identity Card</div>
<div class="drug-header">
<div class="drug-emoji">⚡</div>
<div>
<div class="drug-name">Noradrenaline</div>
<div class="drug-alias">Norepinephrine · Levophed · NE · NAd</div>
</div>
<div>
<span class="drug-class-tag">Endogenous Catecholamine</span>
</div>
</div>
<table class="t">
<tbody>
<tr><td style="font-weight:700;color:#5b21b6;width:38%">Chemical Class</td><td>Catecholamine (sympathomimetic amine)</td></tr>
<tr><td style="font-weight:700;color:#5b21b6">Synthesis</td><td>Tyrosine → DOPA → Dopamine → <strong>Norepinephrine</strong> (via dopamine β-hydroxylase)</td></tr>
<tr><td style="font-weight:700;color:#5b21b6">Storage</td><td>Adrenal medulla (20%), sympathetic nerve terminals (80%)</td></tr>
<tr><td style="font-weight:700;color:#5b21b6">Route</td><td>IV infusion ONLY (not oral; rapid first-pass metabolism)</td></tr>
<tr><td style="font-weight:700;color:#5b21b6">Onset</td><td>1–2 min; Duration = 1–2 min after stopping infusion</td></tr>
<tr><td style="font-weight:700;color:#5b21b6">Metabolism</td><td>MAO + COMT → inactive metabolites (VMA, normetanephrine) → urine</td></tr>
<tr><td style="font-weight:700;color:#5b21b6">Elimination T½</td><td>2–2.5 minutes (very short — allows fine titration)</td></tr>
</tbody>
</table>
</div>
<!-- RECEPTOR PROFILE -->
<div class="card card-indigo">
<div class="st"><span>🔬</span> Receptor Profile & Actions</div>
<div style="text-align:center; margin-bottom:6px;">
<span style="font-size:10px; color:#3730a3; font-weight:700;">NE Receptor Affinity Ranking: </span>
<span class="pill pr">α1 >>></span>
<span class="pill po">α2 >></span>
<span class="pill pb">β1 ></span>
<span class="pill pg">β2 (minimal)</span>
</div>
<div class="rec-grid">
<div class="rec-card rec-a1">
<div class="rec-title">🔴 α1 — DOMINANT</div>
<div class="rec-body">
<strong>Location:</strong> Vascular smooth muscle<br>
<strong>Effect:</strong> ↑↑↑ Vasoconstriction → ↑ SVR → ↑ BP<br>
<strong>Clinical:</strong> Raises MAP; useful in distributive shock<br>
<strong>Also:</strong> Pupil dilation, intestinal relaxation
</div>
</div>
<div class="rec-card rec-a2">
<div class="rec-title">🟠 α2 — Moderate</div>
<div class="rec-body">
<strong>Location:</strong> Presynaptic nerve terminals<br>
<strong>Effect:</strong> ↓ NE release (negative feedback)<br>
<strong>Also:</strong> Platelet aggregation, CNS sedation (if crosses BBB)
</div>
</div>
<div class="rec-card rec-b1">
<div class="rec-title">🔵 β1 — Moderate</div>
<div class="rec-body">
<strong>Location:</strong> Heart (SA node, myocardium)<br>
<strong>Effect:</strong> ↑ Inotropy + ↑ Chronotropy (HR increase)<br>
<strong>BUT:</strong> Net HR often ↓ due to baroreceptor reflex bradycardia<br>
<strong>Net CO:</strong> Usually maintained or slightly ↑
</div>
</div>
<div class="rec-card rec-b2">
<div class="rec-title">🟢 β2 — Minimal</div>
<div class="rec-body">
<strong>Location:</strong> Bronchial, vascular smooth muscle<br>
<strong>Effect:</strong> Minimal bronchodilation; minimal metabolic effect<br>
<strong>Key:</strong> Unlike epinephrine, NE does NOT significantly activate β2<br>
<strong>Result:</strong> No major bronchodilation or hyperglycemia
</div>
</div>
</div>
<div class="al al-b" style="margin-top:6px;">
<span class="ai">💡</span>
<span><strong>NET EFFECT:</strong> Potent vasoconstriction (↑ SVR) + cardiac support (↑ inotropy) + <strong>reflex bradycardia</strong> (due to baroreceptor activation from ↑ BP). MAP rises significantly.</span>
</div>
</div>
</div>
<!-- ══════════ ROW 2: Biosynthesis Pathway + Hemodynamic Effects ══════════ -->
<div class="grid-2">
<div class="card card-teal">
<div class="st"><span>🧬</span> Catecholamine Biosynthesis Pathway</div>
<div style="margin: 6px 0;">
<div class="flow" style="flex-direction:column; align-items:flex-start; gap:2px;">
<div style="display:flex; align-items:center; gap:8px;">
<div class="fb" style="color:#0f766e; background:#f0fdfa; min-width:160px; text-align:left; padding:4px 10px;">🥩 <strong>Phenylalanine</strong> (dietary)</div>
</div>
<div style="padding-left:20px; color:#0d9488; font-size:9.5px;">↓ Phenylalanine hydroxylase</div>
<div style="display:flex; align-items:center; gap:8px;">
<div class="fb" style="color:#ca8a04; background:#fefce8; min-width:160px; text-align:left; padding:4px 10px;">🟡 <strong>Tyrosine</strong></div>
</div>
<div style="padding-left:20px; color:#0d9488; font-size:9.5px;">↓ Tyrosine hydroxylase ⭐ <span style="color:#dc2626; font-weight:700;">RATE-LIMITING STEP</span></div>
<div style="display:flex; align-items:center; gap:8px;">
<div class="fb" style="color:#7c3aed; background:#faf5ff; min-width:160px; text-align:left; padding:4px 10px;">💜 <strong>L-DOPA</strong></div>
</div>
<div style="padding-left:20px; color:#0d9488; font-size:9.5px;">↓ DOPA decarboxylase (AADC)</div>
<div style="display:flex; align-items:center; gap:8px;">
<div class="fb" style="color:#1d4ed8; background:#eff6ff; min-width:160px; text-align:left; padding:4px 10px;">🔵 <strong>Dopamine</strong></div>
</div>
<div style="padding-left:20px; color:#0d9488; font-size:9.5px;">↓ Dopamine β-hydroxylase (DBH) — in vesicles</div>
<div style="display:flex; align-items:center; gap:8px;">
<div class="fb" style="color:#dc2626; background:#fff1f2; min-width:160px; text-align:left; padding:4px 10px; border-width:2.5px; font-size:12px;">🔴 <strong>NOREPINEPHRINE ★</strong></div>
</div>
<div style="padding-left:20px; color:#0d9488; font-size:9.5px;">↓ PNMT (only in adrenal medulla & some brain neurons)</div>
<div style="display:flex; align-items:center; gap:8px;">
<div class="fb" style="color:#ea580c; background:#fff7ed; min-width:160px; text-align:left; padding:4px 10px;">🟠 <strong>Epinephrine</strong></div>
</div>
</div>
</div>
<div class="al al-y" style="margin-top:4px;">
<span class="ai">⭐</span>
<span>Tyrosine hydroxylase = rate-limiting enzyme → inhibited by catecholamine end-product feedback. Target of reserpine (depletes vesicle stores) and metyrosine.</span>
</div>
</div>
<div class="card card-red">
<div class="st"><span>💓</span> Hemodynamic Effects</div>
<table class="t">
<thead><tr><th class="tr">Parameter</th><th class="tr">Effect</th><th class="tr">Mechanism</th></tr></thead>
<tbody>
<tr><td>🩸 <strong>MAP / DBP</strong></td><td style="color:#dc2626; font-weight:700;">↑↑↑ RISES</td><td>α1 → ↑ SVR (vasoconstriction)</td></tr>
<tr><td>💓 <strong>Heart Rate</strong></td><td style="color:#16a34a; font-weight:700;">↓ Decreases (reflex)</td><td>Baroreceptor reflex bradycardia; vagal activation overcomes β1</td></tr>
<tr><td>🫀 <strong>Cardiac Output</strong></td><td>→ Maintained or slightly ↑</td><td>β1 inotropy + ↑ preload; but ↑ afterload may ↓ CO in weak hearts</td></tr>
<tr><td>🩹 <strong>SVR</strong></td><td style="color:#dc2626; font-weight:700;">↑↑↑ Major ↑</td><td>Primary α1 action</td></tr>
<tr><td>🫀 <strong>Contractility</strong></td><td style="color:#16a34a;">↑ Positive inotrope</td><td>β1 stimulation</td></tr>
<tr><td>🩺 <strong>Pulse Pressure</strong></td><td>Narrows slightly</td><td>DBP rises more than SBP</td></tr>
<tr><td>🫘 <strong>Renal Blood Flow</strong></td><td style="color:#dc2626;">↓ Reduced</td><td>Renal artery vasoconstriction</td></tr>
<tr><td>💧 <strong>Skin/Gut Blood Flow</strong></td><td style="color:#dc2626;">↓ Reduced</td><td>Peripheral α1 vasoconstriction</td></tr>
<tr><td>🧠 <strong>Cerebral/Coronary</strong></td><td style="color:#16a34a;">→ Maintained</td><td>Autoregulation; ↑ MAP helps perfusion</td></tr>
<tr><td>🍬 <strong>Blood Glucose</strong></td><td>Minimal change</td><td>Minimal β2 (no glycogenolysis)</td></tr>
</tbody>
</table>
<div class="al al-b" style="margin-top:5px;">
<span class="ai">💡</span>
<span><strong>KEY BARORECEPTOR REFLEX:</strong> ↑ BP → baroreceptors activate → ↑ vagal tone → reflex bradycardia. Net HR = ↓ despite β1 activation. Atropine blocks this reflex → reveals tachycardia.</span>
</div>
</div>
</div>
<div class="divider"></div>
<!-- ══════════ ROW 3: INDICATIONS + DOSING ══════════ -->
<div class="grid-2">
<div class="card card-green">
<div class="st"><span>✅</span> Indications — When to Use NE</div>
<div class="sh">Primary Indication: Shock States</div>
<table class="t">
<thead><tr><th class="tg">Shock Type</th><th class="tg">Role</th><th class="tg">Evidence</th></tr></thead>
<tbody>
<tr style="background:#f0fdf4"><td>🦠 <strong>Septic Shock</strong></td><td><span class="pill pg">1st LINE</span> — Start after 30 mL/kg IVF</td><td>Survivor sepsis campaign; NE superior to dopamine (↓ arrhythmias)</td></tr>
<tr><td>🫀 <strong>Cardiogenic Shock</strong></td><td><span class="pill pg">Preferred 1st line</span> over epinephrine</td><td>Recent data: epinephrine ↑ mortality in cardiogenic shock → NE preferred</td></tr>
<tr style="background:#f0fdf4"><td>🧠 <strong>Neurogenic Shock</strong></td><td><span class="pill pg">1st LINE</span></td><td>α1 restores lost sympathetic tone; target MAP 85–90 mmHg</td></tr>
<tr><td>💉 <strong>Post-Cardiac Arrest</strong></td><td><span class="pill pg">Preferred</span> vasopressor</td><td>Maintain MAP after ROSC; push-dose epi while NE drip prepared</td></tr>
<tr style="background:#f0fdf4"><td>🩺 <strong>Anaphylaxis (refractory)</strong></td><td><span class="pill py">2nd line</span></td><td>After epinephrine fails; for refractory hypotension component</td></tr>
<tr><td>🫘 <strong>Hepatorenal Syndrome</strong></td><td><span class="pill py">2nd line</span></td><td>NE + albumin + furosemide — reversed type 1 HRS in studies</td></tr>
<tr style="background:#f0fdf4"><td>💊 <strong>Distributive Shock (other)</strong></td><td><span class="pill pg">1st LINE</span></td><td>Adrenal crisis, drug-induced, spinal shock</td></tr>
</tbody>
</table>
<div class="al al-g" style="margin-top:6px;">
<span class="ai">🏆</span>
<span><strong>SURVIVNG SEPSIS CAMPAIGN 2021:</strong> NE = preferred 1st-line vasopressor in septic shock. Add vasopressin (0.03 U/min) when NE dose is high, before escalating NE further.</span>
</div>
</div>
<div class="card card-dark">
<div class="st"><span>💉</span> Dosing & Administration</div>
<div class="dose-box">
<div class="dt">⚡ Standard Dosing Regimen</div>
<div class="dose-row"><div class="dose-label">Starting Dose</div><div class="dose-val">0.01–0.1 mcg/kg/min</div><div class="dose-note">(~0.5–2 mcg/min in 70kg adult)</div></div>
<div class="dose-row"><div class="dose-label">Usual Range</div><div class="dose-val">0.01–3 mcg/kg/min</div><div class="dose-note">(Fischer's; titrate to MAP ≥65 mmHg)</div></div>
<div class="dose-row"><div class="dose-label">Septic Shock (Tintinalli)</div><div class="dose-val">0.5–30 mcg/min</div><div class="dose-note">absolute dose (non-weight-based)</div></div>
<div class="dose-row"><div class="dose-label">Goldman-Cecil Range</div><div class="dose-val">1–50 mcg/min</div><div class="dose-note">with MAP target 65–70 mmHg</div></div>
<div class="dose-row"><div class="dose-label">High-Dose / Refractory</div><div class="dose-val">>0.25 mcg/kg/min</div><div class="dose-note">consider adding vasopressin</div></div>
</div>
<div class="sh" style="margin-top:10px;">Administration Rules</div>
<div class="step"><div class="snum sp">1</div><div class="stxt" style="color:#cbd5e1;"><strong>Central Line PREFERRED</strong> — extravasation causes tissue necrosis. Peripheral use acceptable short-term: large bore, proximal, secured, non-distal vein</div></div>
<div class="step"><div class="snum sp">2</div><div class="stxt" style="color:#cbd5e1;"><strong>Never bolus — always continuous infusion</strong> via pump. Short half-life (2 min) allows rapid titration up/down</div></div>
<div class="step"><div class="snum sp">3</div><div class="stxt" style="color:#cbd5e1;"><strong>Dilution:</strong> 4 mg in 250 mL D5W = 16 mcg/mL; or 8 mg in 250 mL = 32 mcg/mL</div></div>
<div class="step"><div class="snum sp">4</div><div class="stxt" style="color:#cbd5e1;"><strong>Target MAP:</strong> ≥65 mmHg (septic shock); 85–90 mmHg (spinal cord/neurogenic shock)</div></div>
<div class="step"><div class="snum sp">5</div><div class="stxt" style="color:#cbd5e1;"><strong>Monitoring:</strong> Continuous arterial line preferred; HR, BP, UO, lactate, skin perfusion q1h</div></div>
<div class="al al-y" style="margin-top:8px;">
<span class="ai">⚠️</span>
<span style="color:#713f12;"><strong>If MAP >65 on NE 0.25+ mcg/kg/min → ADD VASOPRESSIN 0.03 U/min</strong> (steroid-sparing, NE-sparing effect; avoids toxicity)</span>
</div>
</div>
</div>
<!-- ══════════ ROW 4: Adverse Effects + Contraindications ══════════ -->
<div class="grid-2">
<div class="card card-crimson">
<div class="st"><span>⚠️</span> Adverse Effects & Complications</div>
<div class="sh">Primary Adverse Effects</div>
<table class="t">
<thead><tr><th class="tr">Adverse Effect</th><th class="tr">Mechanism</th><th class="tr">Management</th></tr></thead>
<tbody>
<tr><td>🩹 <strong>Tissue Necrosis</strong><br><span style="font-size:9px;color:#6b7280">(Extravasation)</span></td><td>α1 vasoconstriction → ischemia at injection site; skin blanching → sloughing</td><td><strong>Phentolamine</strong> (α-blocker) inject SC around area; OR topical nitroglycerin; OR intradermal terbutaline</td></tr>
<tr><td>💓 <strong>Reflex Bradycardia</strong></td><td>↑ BP → baroreceptor activation → ↑ vagal tone</td><td>Usually benign; reduce dose if hemodynamically significant; atropine if severe</td></tr>
<tr><td>💉 <strong>Hypertension</strong></td><td>Excessive α1 vasoconstriction; over-titration</td><td>Reduce infusion rate; assess MAP target</td></tr>
<tr><td>🫀 <strong>Decreased CO</strong><br><span style="font-size:9px;color:#6b7280">(high doses)</span></td><td>↑ Afterload (SVR) → in hearts with poor function → ↓ CO</td><td>Add dobutamine if inotropy needed; consider ARNI/MCS in cardiogenic</td></tr>
<tr><td>🫘 <strong>Renal Ischemia</strong></td><td>↓ Renal blood flow via renal artery constriction</td><td>Monitor creatinine/urine output; avoid unnecessary high doses</td></tr>
<tr><td>🫀 <strong>Mesenteric Ischemia</strong></td><td>Gut vasoconstriction → bowel ischemia (prolonged use)</td><td>Minimize dose; monitor lactate; consider nutritional support</td></tr>
<tr><td>🧊 <strong>Peripheral Ischemia</strong></td><td>Digit/limb vasoconstriction; ischemic digits, nose</td><td>Minimize dose; local vasodilators; avoid in PAD if possible</td></tr>
<tr><td>💛 <strong>Hyperglycemia</strong></td><td>Mild (minimal β2 activity)</td><td>Monitor glucose; insulin if needed</td></tr>
<tr><td>🫁 <strong>Pulmonary HTN</strong></td><td>Pulmonary vasoconstriction (high doses)</td><td>Use lowest effective dose; consider inhaled vasodilators</td></tr>
</tbody>
</table>
<div class="al al-r" style="margin-top:6px;">
<span class="ai">🚨</span>
<div><strong>EXTRAVASATION EMERGENCY:</strong> If NE leaks into tissue → immediate phentolamine 5–10 mg in 10 mL NS injected SC into affected area. Do within 12 hours. Alternative: topical nitroglycerin patch over area.</div>
</div>
</div>
<div class="card card-orange">
<div class="st"><span>🚫</span> Contraindications & Cautions</div>
<div class="sh">Absolute Contraindications</div>
<ul class="dl">
<li>❌ <strong>Hypovolemic shock (uncorrected)</strong> — NE without adequate volume = fatal vasoconstriction; always resuscitate first with 30 mL/kg crystalloid</li>
<li>❌ <strong>Mesenteric/peripheral vascular thrombosis</strong> — increases ischemia</li>
<li>❌ <strong>Halothane anesthesia</strong> — risk of severe arrhythmias</li>
<li>❌ <strong>Cyclopropane anesthesia</strong> — ventricular fibrillation risk</li>
</ul>
<div class="sh">Relative Contraindications / Use with Caution</div>
<ul class="dl">
<li>⚠️ <strong>Severe cardiac dysfunction / LV failure</strong> — ↑ afterload worsens CO; add dobutamine</li>
<li>⚠️ <strong>MAO inhibitors</strong> — potentiation of pressor response (exaggerated HTN); use lowest dose with extreme caution</li>
<li>⚠️ <strong>Tricyclic antidepressants</strong> — potentiation via inhibiting NE reuptake</li>
<li>⚠️ <strong>Pregnancy</strong> — uterine vasoconstriction → fetal ischemia; use only when maternal benefit outweighs risk</li>
<li>⚠️ <strong>Severe atherosclerosis / PVD</strong> — peripheral ischemia risk</li>
</ul>
<div class="sh">Drug Interactions</div>
<table class="t">
<thead><tr><th class="to">Drug</th><th class="to">Interaction</th><th class="to">Effect</th></tr></thead>
<tbody>
<tr><td>MAO inhibitors</td><td>↓ NE breakdown</td><td>↑↑↑ Hypertensive crisis</td></tr>
<tr><td>TCAs (imipramine)</td><td>Block NE reuptake</td><td>↑ Pressor effect</td></tr>
<tr><td>Halogenated anesthetics</td><td>Sensitize myocardium</td><td>VF risk</td></tr>
<tr><td>α-blockers (phentolamine)</td><td>Antagonize α1</td><td>↓ BP effect; used for extravasation</td></tr>
<tr><td>β-blockers</td><td>Block β1/β2</td><td>Unmasks pure α1 — HTN ↑↑</td></tr>
<tr><td>Oxytocin</td><td>Additive vasoconstriction</td><td>↑ HTN risk</td></tr>
</tbody>
</table>
</div>
</div>
<div class="divider"></div>
<!-- ══════════ ROW 5: Vasopressor Comparison Table ══════════ -->
<div class="grid-full">
<div class="card card-dark">
<div class="st"><span>⚖️</span> Vasopressor Comparison Table — Emergency Medicine Quick Reference</div>
<table class="t" style="color:#f8fafc;">
<thead>
<tr>
<th class="td">Drug</th>
<th class="td">α1</th><th class="td">β1</th><th class="td">β2</th><th class="td">Dop</th>
<th class="td">MAP</th><th class="td">HR</th><th class="td">CO</th><th class="td">SVR</th>
<th class="td">Primary Use</th>
<th class="td">Key Feature</th>
</tr>
</thead>
<tbody>
<tr style="background:rgba(239,68,68,0.15)">
<td><strong style="color:#fbbf24;">⚡ Norepinephrine</strong></td>
<td><span style="color:#ef4444;font-weight:700;">++++</span></td>
<td><span style="color:#60a5fa;font-weight:700;">++</span></td>
<td><span style="color:#4ade80;">+</span></td>
<td>0</td>
<td style="color:#4ade80;">↑↑↑</td>
<td style="color:#f87171;">↓ (reflex)</td>
<td>→/↑</td>
<td style="color:#ef4444;">↑↑↑</td>
<td><span class="pill pg">🥇 Septic/Distributive</span></td>
<td>1st-line most shock; reflex bradycardia</td>
</tr>
<tr style="background:rgba(255,255,255,0.03)">
<td><strong>Epinephrine</strong></td>
<td><span style="color:#ef4444;font-weight:700;">+++</span></td>
<td><span style="color:#60a5fa;font-weight:700;">++++</span></td>
<td><span style="color:#4ade80;font-weight:700;">+++</span></td>
<td>0</td>
<td style="color:#4ade80;">↑↑</td>
<td style="color:#ef4444;">↑↑</td>
<td style="color:#4ade80;">↑↑</td>
<td style="color:#ef4444;">↑↑</td>
<td><span class="pill pr">🏥 Anaphylaxis; 2nd-line sepsis</span></td>
<td>Tachycardia; hyperglycemia; lactic acidosis; arrhythmogenic</td>
</tr>
<tr style="background:rgba(255,255,255,0.06)">
<td><strong>Dopamine</strong></td>
<td>0/+ (dose)</td>
<td><span style="color:#60a5fa;font-weight:700;">+++</span></td>
<td><span style="color:#4ade80;">+</span></td>
<td><span style="color:#a78bfa;font-weight:700;">+++</span></td>
<td style="color:#4ade80;">↑↑</td>
<td style="color:#ef4444;">↑↑</td>
<td style="color:#4ade80;">↑↑</td>
<td>→/↑</td>
<td><span class="pill py">⚠️ No longer 1st-line; special cases</span></td>
<td>MORE arrhythmias (AF) than NE; dose-dependent effects</td>
</tr>
<tr style="background:rgba(255,255,255,0.03)">
<td><strong>Vasopressin</strong></td>
<td>0</td><td>0</td><td>0</td><td>0</td>
<td style="color:#4ade80;">↑</td>
<td style="color:#f87171;">↓</td>
<td style="color:#f87171;">↓ slightly</td>
<td style="color:#ef4444;">↑↑</td>
<td><span class="pill pb">2nd-line add-on to NE</span></td>
<td>No arrhythmias; 0.03 U/min fixed dose; non-adrenergic</td>
</tr>
<tr style="background:rgba(255,255,255,0.06)">
<td><strong>Phenylephrine</strong></td>
<td><span style="color:#ef4444;font-weight:700;">++++</span></td>
<td>0</td><td>0</td><td>0</td>
<td style="color:#4ade80;">↑↑</td>
<td style="color:#f87171;">↓↓ (reflex)</td>
<td style="color:#f87171;">↓</td>
<td style="color:#ef4444;">↑↑↑</td>
<td><span class="pill ppk">If tachyarrhythmia with NE</span></td>
<td>Pure α1; no β; ↓ CO; avoid in cardiogenic shock</td>
</tr>
<tr style="background:rgba(255,255,255,0.03)">
<td><strong>Dobutamine</strong></td>
<td>0/+</td>
<td><span style="color:#60a5fa;font-weight:700;">++++</span></td>
<td><span style="color:#4ade80;font-weight:700;">++</span></td>
<td>0</td>
<td>→/↓</td>
<td style="color:#ef4444;">↑</td>
<td style="color:#4ade80;">↑↑↑</td>
<td style="color:#f87171;">↓</td>
<td><span class="pill pb">Cardiogenic shock + NE</span></td>
<td>Pure inotrope; vasodilator; add to NE when CO low</td>
</tr>
<tr style="background:rgba(255,255,255,0.06)">
<td><strong>Angiotensin II</strong></td>
<td>0</td><td>0</td><td>0</td><td>0</td>
<td style="color:#4ade80;">↑↑</td>
<td>→</td>
<td>→</td>
<td style="color:#ef4444;">↑↑</td>
<td><span class="pill po">Refractory shock (NE failed)</span></td>
<td>Non-catecholamine; Giapreza; thrombotic risk; last resort</td>
</tr>
</tbody>
</table>
</div>
</div>
<!-- ══════════ ROW 6: Monitoring + NE in Special Scenarios ══════════ -->
<div class="grid-2">
<div class="card card-blue">
<div class="st"><span>📊</span> Monitoring on Norepinephrine</div>
<div class="sh">Hemodynamic Targets</div>
<table class="t">
<thead><tr><th class="tb">Parameter</th><th class="tb">Target</th><th class="tb">Note</th></tr></thead>
<tbody>
<tr><td>MAP</td><td style="color:#16a34a;font-weight:700;">≥ 65 mmHg</td><td>Septic shock standard; may need 85–90 in spinal SCI</td></tr>
<tr><td>Urine Output</td><td style="color:#16a34a;font-weight:700;">> 0.5 mL/kg/hr</td><td>Marker of end-organ perfusion</td></tr>
<tr><td>Lactate</td><td style="color:#16a34a;font-weight:700;">< 2 mmol/L</td><td>Target clearance >10% per 2h; rising lactate = inadequate perfusion</td></tr>
<tr><td>ScvO₂</td><td style="color:#16a34a;font-weight:700;">> 70%</td><td>Central venous O₂ saturation</td></tr>
<tr><td>HR</td><td>60–100 bpm</td><td>NE often causes reflex bradycardia; <40 → reduce dose</td></tr>
<tr><td>Skin perfusion</td><td>Warm extremities</td><td>Mottling, cold digits = ischemia; minimize dose</td></tr>
<tr><td>Creatinine/BUN</td><td>Stable/improving</td><td>Monitor for renal ischemia</td></tr>
</tbody>
</table>
<div class="sh" style="margin-top:6px;">Weaning Protocol</div>
<ul class="dl">
<li>Wean by 0.01–0.05 mcg/kg/min every 15–30 min once MAP stable >65 for 4+ hours</li>
<li>Ensure volume resuscitation adequate before weaning</li>
<li>Wean vasopressin last (add first, remove last)</li>
<li>Watch for vasoplegic rebound when discontinuing (have fluids ready)</li>
</ul>
</div>
<div class="card card-purple">
<div class="st"><span>🏥</span> NE in Special Clinical Scenarios</div>
<table class="t">
<thead><tr><th class="tp">Scenario</th><th class="tp">NE Role</th><th class="tp">Special Consideration</th></tr></thead>
<tbody>
<tr><td>🦠 <strong>Septic Shock</strong></td><td>🥇 1st line</td><td>Start early (even peripheral); target MAP 65; add vasopressin when dose >0.25 mcg/kg/min</td></tr>
<tr><td>🫀 <strong>Cardiogenic Shock</strong></td><td>🥇 Preferred over Epi</td><td>Epi ↑ mortality data → use NE; ADD dobutamine for inotropy; consider IABP/Impella</td></tr>
<tr><td>🧠 <strong>Neurogenic Shock</strong></td><td>🥇 1st line</td><td>Target MAP 85–90 mmHg × 7 days; bradycardia prominent → atropine/pacing if needed</td></tr>
<tr><td>🔄 <strong>Post-Cardiac Arrest</strong></td><td>Preferred vasopressor</td><td>Push-dose epi while NE drip prepared; concurrent dobutamine if EF low</td></tr>
<tr><td>💊 <strong>Anaphylaxis</strong></td><td>2nd line (after epi IM)</td><td>For refractory hypotension after IM epinephrine; vasoplegic component</td></tr>
<tr><td>🤰 <strong>Obstetric Hypotension</strong></td><td>Use cautiously</td><td>Uterine vasoconstriction risk; phenylephrine or ephedrine preferred in spinal anesthesia hypotension</td></tr>
<tr><td>👶 <strong>Pediatric Septic Shock</strong></td><td>1st or 2nd line</td><td>NE or Epinephrine 1st line equally; NE 0.1–2 mcg/kg/min; epinephrine associated with faster shock reversal in children</td></tr>
<tr><td>🏥 <strong>ARDS + Sepsis</strong></td><td>Maintain MAP ≥65</td><td>Avoid excessive fluids (lung protective); early NE reduces fluid loading</td></tr>
</tbody>
</table>
</div>
</div>
<div class="divider"></div>
<!-- ══════════ ROW 7: High-Yield Pearls + Mnemonics ══════════ -->
<div class="grid-2">
<div class="card card-green">
<div class="st"><span>💎</span> High-Yield Exam Pearls</div>
<div class="pearl" style="margin-top:12px;">
<p><strong>PEARL 1:</strong> NE = α1 >> β1; produces vasoconstriction + reflex bradycardia. NET HR = down despite β1 stimulation (baroreceptor overrides β1).</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 2:</strong> NE is the FIRST-LINE vasopressor in septic shock (Surviving Sepsis Campaign). Dopamine is NOT preferred — higher rate of atrial fibrillation and arrhythmias (Goldman-Cecil).</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 3:</strong> In cardiogenic shock — NE is preferred over epinephrine. Recent data show epinephrine associated with INCREASED MORTALITY in cardiogenic shock (Rosen's EM).</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 4:</strong> EXTRAVASATION = tissue necrosis. Antidote = PHENTOLAMINE (α-blocker, 5–10 mg SC around area). Alternative: topical nitroglycerin or intradermal terbutaline (Lippincott).</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 5:</strong> Half-life = 2 minutes (very short). Allows rapid titration. Given only by IV infusion. Metabolized by MAO + COMT → vanillylmandelic acid (VMA) in urine.</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 6:</strong> Rate-limiting step in catecholamine synthesis = TYROSINE HYDROXYLASE (Tyrosine → L-DOPA). Inhibited by end-product feedback. Target of metyrosine (Pheochromocytoma Rx).</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 7:</strong> When NE dose >0.25 mcg/kg/min without MAP target → ADD VASOPRESSIN 0.03 U/min fixed (do NOT titrate — higher doses = vasospasm). Do not add vasopressin as first agent.</p>
</div>
<div class="pearl" style="margin-top:14px;">
<p><strong>PEARL 8:</strong> NE vs Epinephrine for ANAPHYLAXIS — Epinephrine IM (thigh) is the FIRST LINE treatment for anaphylaxis. NE is second-line for refractory hypotension after Epi IM.</p>
</div>
</div>
<div class="card card-yellow">
<div class="st"><span>🧠</span> Memory Tricks & Mnemonics</div>
<div class="mn" style="margin-bottom:9px;">
<div class="mnt">⚡ NE Receptor Profile — "Alpha MAJOR, Beta Minor"</div>
<div class="lts">
<div class="lb"><strong>α1</strong> DOMINANT → Vasoconstrict → ↑ BP → ↑↑↑ SVR</div>
<div class="lb"><strong>β1</strong> moderate → ↑ Inotropy BUT reflex ↓ HR wins</div>
<div class="lb"><strong>β2</strong> minimal → No bronchodilation, no hypoglycemia</div>
<div class="lb"><strong>Net HR:</strong> ↓ (baroreceptor reflex OVERCOMES β1)</div>
</div>
</div>
<div class="mn" style="margin-bottom:9px;">
<div class="mnt">🏆 Vasopressor Order — "NE VADs" (Surviving Sepsis)</div>
<div class="lts">
<div class="lb"><strong>N</strong>orepinephrine — 1st line ALWAYS</div>
<div class="lb"><strong>E</strong>pinephrine — 2nd line (add to NE)</div>
<div class="lb"><strong>VA</strong>sopressin — add-on at 0.03 U/min (NE-sparing)</div>
<div class="lb"><strong>D</strong>opamine — NO (more arrhythmias)</div>
<div class="lb"><strong>S</strong>teroids (hydrocortisone) — refractory shock</div>
</div>
</div>
<div class="mn" style="margin-bottom:9px;">
<div class="mnt">💊 NE vs Epinephrine — "NE = No Excitement (no β2)"</div>
<div style="display:grid; grid-template-columns:1fr 1fr; gap:6px; margin-top:4px;">
<div style="background:rgba(239,68,68,0.12); border:1px solid rgba(239,68,68,0.3); border-radius:7px; padding:6px 9px;">
<div style="color:#fca5a5; font-size:9.5px; font-weight:700; margin-bottom:3px;">⚡ NOREPINEPHRINE</div>
<div style="font-size:9.5px; color:#e2e8f0; line-height:1.6;">α1 >> β1; no β2<br>↑↑ BP; ↓ HR (reflex)<br>No glycogenolysis<br>No bronchodilation<br>1st-line: septic/distributive</div>
</div>
<div style="background:rgba(251,191,36,0.12); border:1px solid rgba(251,191,36,0.3); border-radius:7px; padding:6px 9px;">
<div style="color:#fbbf24; font-size:9.5px; font-weight:700; margin-bottom:3px;">🟡 EPINEPHRINE</div>
<div style="font-size:9.5px; color:#e2e8f0; line-height:1.6;">α1 + β1 + β2 all active<br>↑ BP; ↑↑ HR; ↑ CO<br>Hyperglycemia<br>Bronchodilation (β2)<br>1st-line: Anaphylaxis</div>
</div>
</div>
</div>
<div class="mn">
<div class="mnt">🧪 Catecholamine Synthesis Mnemonic — "The DOPE Needs No Escape"</div>
<div class="lts">
<div class="lb"><strong>T</strong>yrosine → rate-limiting step (TH enzyme)</div>
<div class="lb"><strong>D</strong>OPA → via tyrosine hydroxylase</div>
<div class="lb"><strong>D</strong>opamine → via AADC</div>
<div class="lb"><strong>N</strong>orepinephrine → via DBH (in vesicles)</div>
<div class="lb"><strong>E</strong>pinephrine → via PNMT (adrenal medulla only)</div>
</div>
</div>
<div class="al al-r" style="margin-top:8px;">
<span class="ai">🚨</span>
<div><strong>DANGER — WHEN TO STOP / REDUCE NE:</strong><br>
• Ischemic digits / mottled extremities (limb-threatening)<br>
• SBP >180 mmHg (over-pressor)<br>
• HR <40 bpm (severe reflex bradycardia)<br>
• Rising lactate despite MAP >65 (maldistribution)</div>
</div>
</div>
</div>
<!-- ══════════ ROW 8: One-Liners + Quick Summary ══════════ -->
<div class="grid-3">
<div class="card card-slate">
<div class="st"><span>🌟</span> One-Liners for Exams</div>
<ul class="dl">
<li>🎯 NE = <strong>α1 >> β1</strong>; minimal β2</li>
<li>🎯 Net HR = <strong>↓</strong> (reflex bradycardia wins)</li>
<li>🎯 1st-line vasopressor: <strong>septic + distributive + neurogenic shock</strong></li>
<li>🎯 NOT 1st-line in anaphylaxis — <strong>epinephrine IM is</strong></li>
<li>🎯 Preferred over epinephrine in <strong>cardiogenic shock</strong></li>
<li>🎯 Extravasation → <strong>phentolamine SC</strong></li>
<li>🎯 Add <strong>vasopressin 0.03 U/min</strong> when NE dose is high</li>
<li>🎯 Metabolized by <strong>MAO + COMT</strong></li>
<li>🎯 Half-life = <strong>2 minutes</strong> → allows precise titration</li>
<li>🎯 Dopamine = more AF than NE → <strong>no longer 1st line</strong></li>
<li>🎯 Rate-limiting step of synthesis = <strong>tyrosine hydroxylase</strong></li>
<li>🎯 MAOIs + NE = <strong>hypertensive crisis</strong> risk</li>
<li>🎯 Target MAP: <strong>≥65 septic</strong>; <strong>85–90 neurogenic</strong></li>
<li>🎯 Peripheral use OK short-term but <strong>central line preferred</strong></li>
</ul>
</div>
<div class="card card-teal">
<div class="st"><span>⚗️</span> Pharmacokinetics Summary</div>
<table class="t">
<thead><tr><th class="tt">Parameter</th><th class="tt">Value</th></tr></thead>
<tbody>
<tr><td>Route</td><td>IV infusion ONLY</td></tr>
<tr><td>Onset</td><td>1–2 minutes</td></tr>
<tr><td>Duration</td><td>1–2 min after stopping</td></tr>
<tr><td>Half-life</td><td>~2 minutes</td></tr>
<tr><td>Protein binding</td><td>~25%</td></tr>
<tr><td>Metabolism</td><td>MAO + COMT (liver, kidney, nerve terminal)</td></tr>
<tr><td>Metabolites</td><td>VMA, Normetanephrine (urine)</td></tr>
<tr><td>Renal dose adj</td><td>Not required</td></tr>
<tr><td>Hepatic dose adj</td><td>Not required</td></tr>
</tbody>
</table>
<div class="al al-b" style="margin-top:6px;">
<span class="ai">💡</span>
<span>VMA (vanillylmandelic acid) is the major urinary metabolite of both NE and epinephrine. Elevated in pheochromocytoma diagnosis.</span>
</div>
</div>
<div class="card card-pink">
<div class="st"><span>🔴</span> NE vs Dopamine — The Classic Controversy</div>
<table class="t">
<thead><tr><th class="tr">Feature</th><th class="tr">Norepinephrine</th><th class="tr">Dopamine</th></tr></thead>
<tbody>
<tr><td>Receptors</td><td>α1 >> β1</td><td>D1 > β1 > α1 (dose-dep)</td></tr>
<tr><td>HR</td><td>↓ (reflex brady)</td><td>↑↑ (chronotropic)</td></tr>
<tr><td>Arrhythmias</td><td style="color:#16a34a;font-weight:700;">Less</td><td style="color:#dc2626;font-weight:700;">More (esp. AF)</td></tr>
<tr><td>Mortality</td><td style="color:#16a34a;font-weight:700;">Lower (slightly)</td><td>Higher</td></tr>
<tr><td>Renal "protection"</td><td>No specific benefit</td><td>Myth dispelled — no benefit</td></tr>
<tr><td>Recommendation</td><td style="color:#16a34a;font-weight:700;">1st LINE</td><td style="color:#dc2626;font-weight:700;">NOT 1st line</td></tr>
<tr><td>Exception</td><td>—</td><td>Bradycardia + hypotension</td></tr>
</tbody>
</table>
<div class="al al-y" style="margin-top:6px;">
<span class="ai">⭐</span>
<span><strong>De Backer 2010 (NEJM):</strong> RCT showed dopamine → more arrhythmias (24.1% vs 12.4%) and trend toward worse outcomes vs NE in septic shock → NE became definitive 1st-line.</span>
</div>
</div>
</div>
<!-- ══════════ FOOTER ══════════ -->
<div class="footer">
<p>📚 Sources: <strong>Lippincott Illustrated Reviews Pharmacology</strong> | <strong>Tintinalli's EM</strong> | <strong>Rosen's Emergency Medicine</strong> | <strong>Goldman-Cecil Medicine</strong> | <strong>Harrison's Principles 22E</strong> | <strong>Fischer's Mastery of Surgery</strong></p>
<p>🚨 <strong>Emergency Medicine PGY-1 Reference</strong> | Noradrenaline / Norepinephrine | ✨ Orris AI</p>
</div>
</div>
</body>
</html>
ls -lh /tmp/workspace/noradrenaline-poster/
Norepinephrine (noradrenaline) pharmacology medical infographic diagram showing: adrenergic receptor subtypes (alpha-1, alpha-2, beta-1, beta-2) with their locations and effects on the body. Central nervous system pathway showing sympathetic nervous system activation, adrenal medulla releasing catecholamines. Biosynthesis pathway: Tyrosine to DOPA to Dopamine to Norepinephrine to Epinephrine. Hemodynamic effects arrows showing increased SVR, MAP increase, reflex bradycardia via baroreceptors. Chemical structure of norepinephrine. Color-coded: red for alpha-1 effects, blue for beta-1 effects. Professional medical illustration, white background, clean and educational style.
⚡ NORADRENALINE — Emergency Medicine PGY-1 Master Sheet
📥 Download Your Poster
noradrenaline poster
HTML File · HTML
Open in any browser → Ctrl+P → Save as PDF (landscape, scale to fit) for a print-ready study sheet.
🖼️ Pharmacology Mechanism Diagram
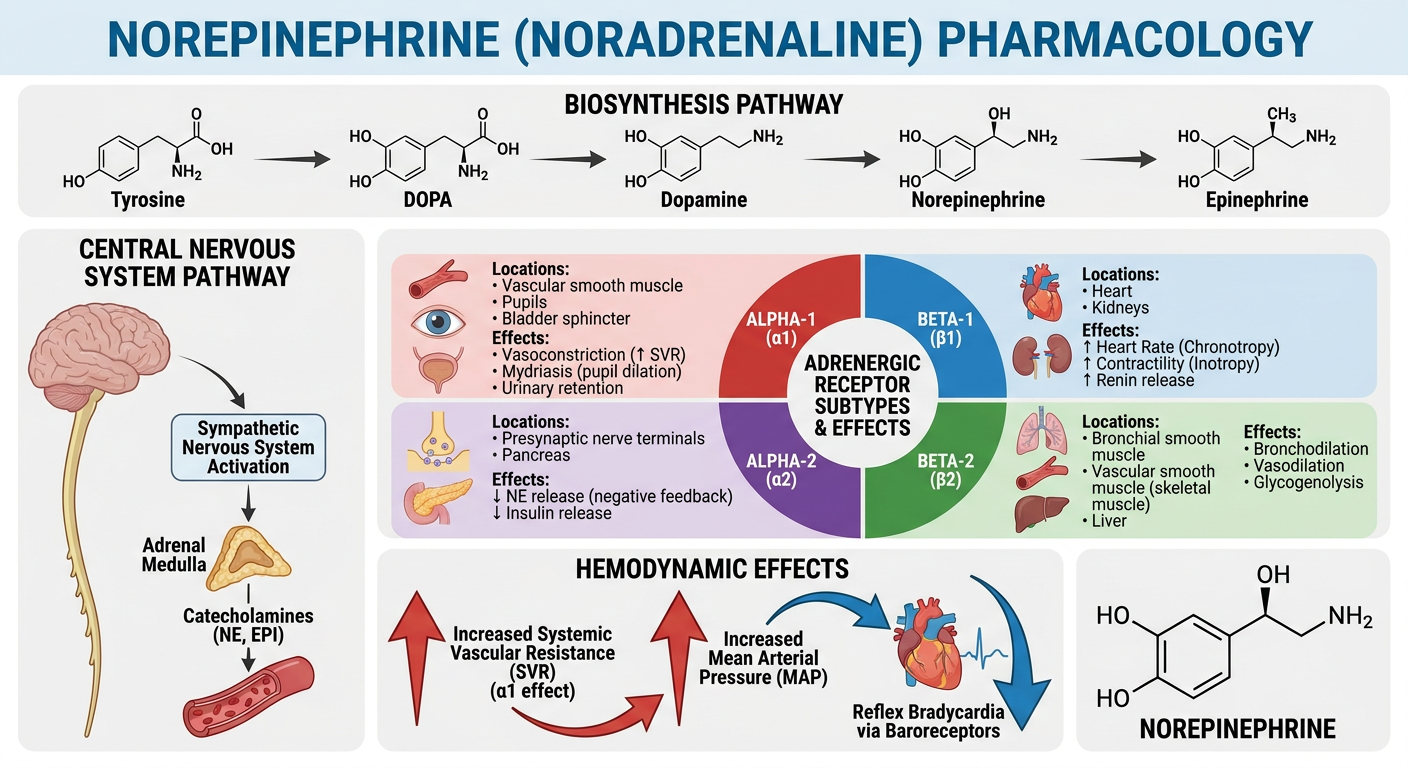
📋 What's Inside — All Sections Covered
| Section | Key Content |
|---|---|
| 🪪 Drug Identity | Names, chemical class, route, onset, metabolism, half-life |
| 🔬 Receptor Profile | α1 (dominant), α2, β1, β2 — each receptor's location & effect |
| 🧬 Biosynthesis Pathway | Tyrosine → DOPA → Dopamine → NE → Epi (rate-limiting step = Tyrosine hydroxylase) |
| 💓 Hemodynamic Effects | ↑↑↑ MAP, ↓ HR (reflex bradycardia), ↑ SVR, maintained CO |
| ✅ Indications | Septic shock (1st line), cardiogenic, neurogenic, post-arrest |
| 💉 Dosing | 0.01–3 mcg/kg/min; MAP targets; central vs peripheral; titration |
| ⚠️ Adverse Effects | Extravasation necrosis, reflex bradycardia, renal/mesenteric ischemia |
| 🚫 Contraindications | Uncorrected hypovolemia, MAOIs, halothane anesthesia |
| ⚖️ Vasopressor Comparison | NE vs Epinephrine vs Dopamine vs Vasopressin vs Phenylephrine vs Dobutamine |
| 📊 Monitoring | MAP ≥65, UO, lactate, ScvO₂, weaning protocol |
| 💎 8 High-Yield Pearls | Exam-critical one-liners from authoritative sources |
| 🧠 Mnemonics | NE receptor profile, vasopressor order, NE vs Epi comparison |
🔥 Top 5 Must-Know Facts for Exams
- α1 >>> β1; minimal β2 — vasoconstriction dominates; net HR decreases (baroreceptor reflex)
- 1st-line in septic shock — superior to dopamine (less AF, fewer arrhythmias) - De Backer 2010
- Cardiogenic shock: prefer NE over Epinephrine — Epi associated with ↑ mortality in cardiogenic shock
- Extravasation = tissue necrosis → phentolamine SC (α-blocker; inject within 12h)
- Half-life = 2 minutes — allows minute-to-minute titration; add vasopressin 0.03 U/min when NE dose is high