Discuss the post-mortem findings on the face and neck in a case of complete typical hanging, correlating with the above case.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the material needed. Let me compile the comprehensive answer.
Post-Mortem Findings on the Face and Neck in Complete Typical Hanging
Context note - "Complete typical hanging": In complete hanging, the entire body weight acts as the constricting force (feet off the ground). In typical hanging, the knot is positioned over the occiput (back of the neck), which places maximum pressure on the front and sides of the neck, directly over the carotid vessels. These two features together produce the classic, well-defined pattern described below.
A. External Findings on the Face
1. Facial Pallor (Characteristic Feature)
In complete typical hanging, the face is usually pale, not congested. This is the cardinal and distinguishing finding. Pallor results from complete occlusion of both the carotid arteries (requiring only ~3.5-5 kg of pressure) and vertebral arteries, meaning no blood pools in the head. Vagal inhibition also contributes to facial pallor. This distinguishes complete hanging from partial/atypical hanging, where facial congestion and petechiae are more common.
- Correlation with the case: If the case shows a pale, drained face, it supports complete suspension where all arterial supply to the head was occluded.
2. Eyes
- The eyeballs appear prominent and protrude due to congestion (more pronounced in partial hanging but may be seen in complete hanging as well).
- The eyes may be closed or partially open; pupils are usually dilated.
- The conjunctivae are congested; petechial hemorrhages in the conjunctivae are found in ~25% of cases, though they are far more common in incomplete suspension.
- "Le facie sympathique": If the ligature knot compresses the cervical sympathetic chain, the ipsilateral eye may remain open with a dilated pupil - a sign indicating antemortem hanging.
3. Tongue
The tongue is one of the most diagnostically useful findings in hanging:
- It is swollen, turgid, and blue at the base.
- The noose lifts the glossopharyngeal skeleton, causing protrusion of the tongue between the lips and teeth.
- The protruding portion dries out, becoming dark brown or black in colour, due to desiccation (Figure 8.21, DiMaio).
- In complete typical hanging, the tongue may be clamped between the teeth or lips.

Fig: Protrusion of tongue with bluish-purple lips in hanging (DiMaio's Forensic Pathology, 3rd Ed.)
4. Lips and Oral Mucosa
- The lips and oral mucous membranes are cyanosed/blue due to asphyxial congestion.
- Slight bloody froth may occasionally be seen at the mouth and nostrils from rupture of engorged vessels in congested lungs - this should not be mistaken for evidence of assault.
5. Salivary Staining (Important Antemortem Sign)
- Saliva dribbles from the angle of the mouth on the side opposite to the knot - a dried rivulet running down the chest is a classic finding.
- This results from stimulation of the salivary glands and pterygopalatine ganglion by the ligature, as well as congestive hypoxia.
- Medicolegal importance: Salivary staining is an important indicator of antemortem hanging - it cannot be reproduced postmortem. Absence does not exclude hanging.
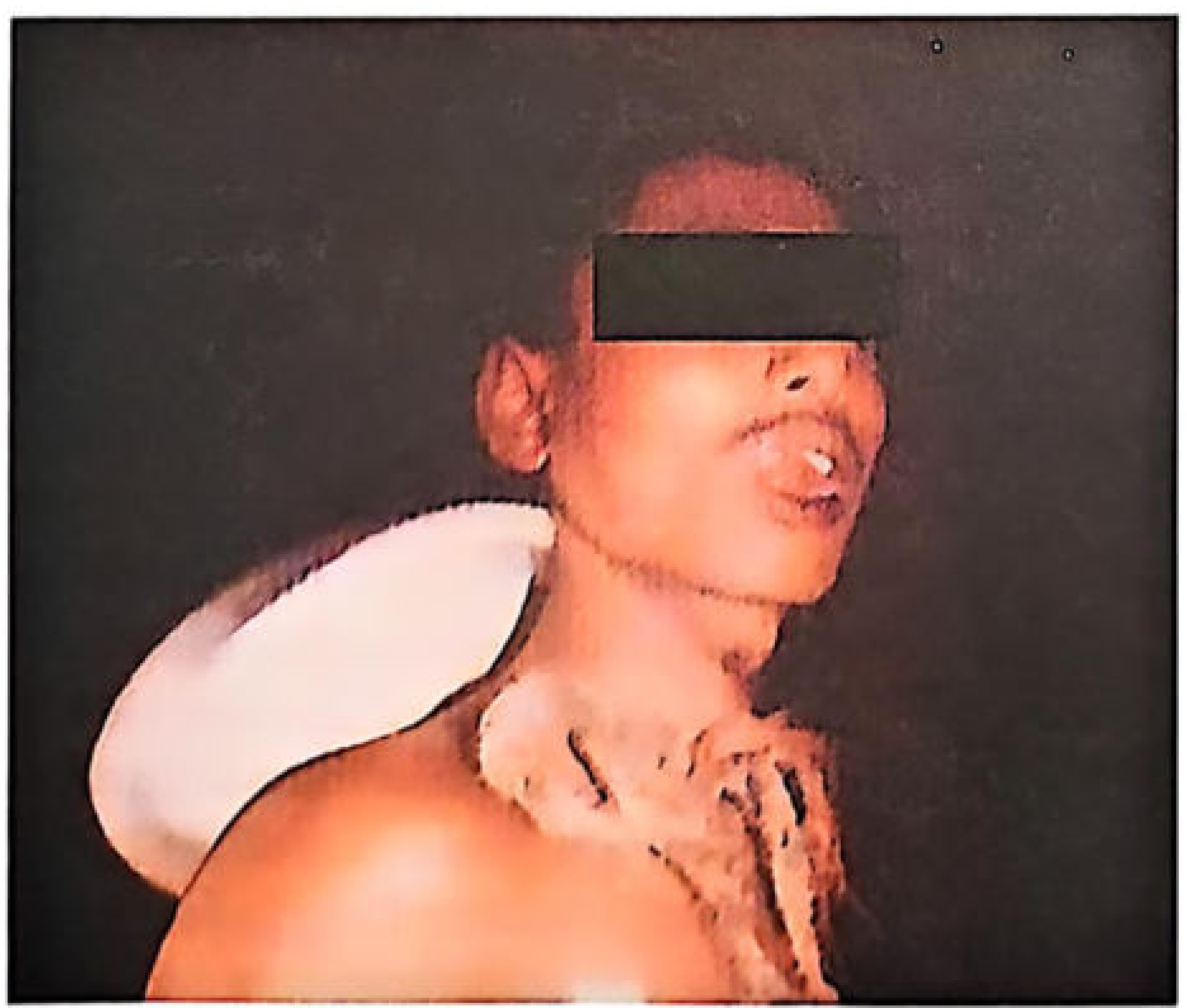
Fig: Case of hanging showing ligature mark and salivary staining on the chest (Essentials of FMT, 36th Ed.)
6. Head Position
- The neck is stretched and elongated due to the upward pull of the ligature.
- The head is tilted/inclined to the side opposite the knot, due to gravitational forces.
7. Petechiae
- In complete typical hanging, petechial hemorrhages of the face and conjunctivae are relatively uncommon or absent because both arteries and veins are fully occluded - there is no excess pressure to rupture capillaries in the head.
- Petechiae are characteristic of partial/incomplete suspension where venous return is blocked but vertebral arterial supply continues.
B. The Ligature Mark (Central Finding on the Neck)
The ligature mark is the single most important post-mortem finding and is unique to hanging. Its features in complete typical hanging are:
Position and Course
- Located above the level of the thyroid cartilage, between the larynx and chin.
- Does not run horizontally around the neck - instead it runs obliquely upward, directed along the line of the mandible toward the mastoid processes behind the ears (Figure 8.17, DiMaio).
- It does not completely encircle the neck - it fades out and is absent or least prominent at the back, where the two limbs of the noose converge at the knot.
- In typical hanging (knot occipital), the front and sides of the neck show the most prominent and deepest mark, while the nape may show little or no mark due to firm musculature and scalp hair.
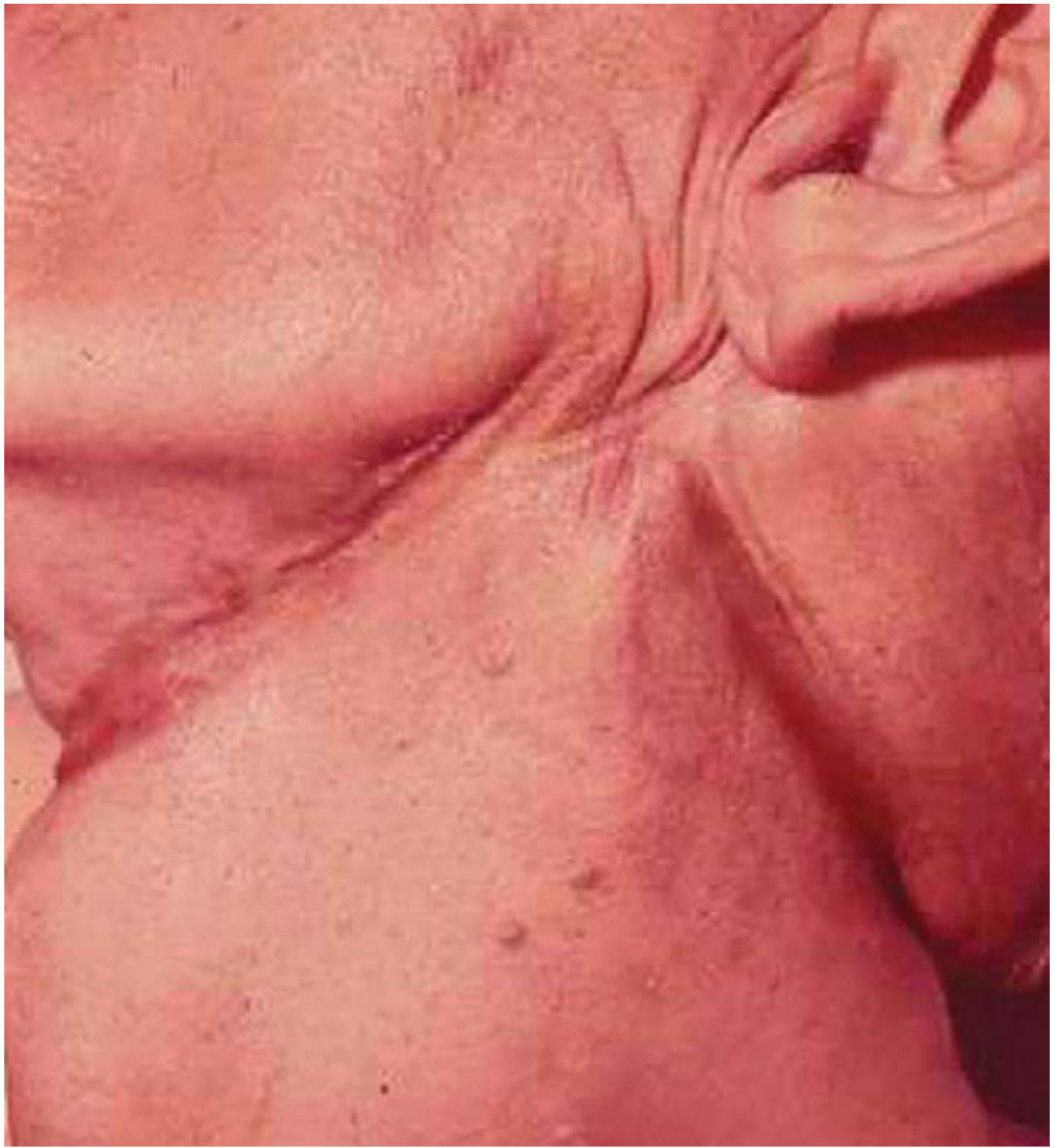
Fig: The ligature furrow in hanging, slanting obliquely upward toward the knot (DiMaio's Forensic Pathology, 3rd Ed.)
Shape
- Typically inverted V-shaped (or inverted U-shaped), with the apex of the V directed toward the knot (occiput in typical hanging).
- Impression of the knot may be found as a separate abrasion/indentation at the site.
Appearance of the Groove
- Fresh mark: appears pale, poorly defined.
- After several hours of drying: becomes yellowish-brown, dry, hard, and parchment-like - a leathery groove or furrow.
- The deepest portion of the mark is opposite the point of suspension (i.e., anteriorly in typical hanging).
- Along the edges: a thin line of congestion or ecchymosis may be seen above and below the groove at the deepest point.
- Abrasions with hemorrhage in the groove are strongly suggestive of antemortem hanging.
- Fibres from the ligature may be found adhering to the skin (useful for ligature material identification).
Width and Clarity - Correlation with Ligature Material
- Thin, hard ligature (wire, rope, cord): narrow, deep, distinct groove with mirror-image impression of the material's texture (e.g., twist pattern of rope reproduced on skin).
- Broad, soft ligature (dupatta, sari strip, towel): wide, shallow, ill-defined furrow.
- Fabric pulled tight: only the raised ridges contact the skin, producing a narrower mark than expected.
- A belt leaves two parallel furrows from its upper and lower edges.
Other Features
- A double furrow may be produced by: (a) a double loop, or (b) slipping of the ligature causing two impressions.
- If a knot is under the chin: an abrasion or indentation beneath the chin marks its site.
- Scratch abrasions above and below the ligature may be present in a minority of cases, made by the victim's fingernails trying to loosen the noose during the agonal period.
- Ligature marks resist putrefaction because the compressed vessels restrict access by putrefying bacteria - they can remain identifiable even in decomposed bodies.
- The mark may disappear if the ligature is removed soon after death and the body is observed before drying; it may also be reproduced if the body is suspended within 2 hours of death.
C. Internal Neck Findings (Dissection)
Technique
Neck dissection should be done in situ after draining blood from the cranial cavity, chest, and abdomen first (as recommended by Schrader 1940 and DiMaio), in a relatively blood-free field to avoid artefactual hemorrhages from venous seepage.
Findings
| Structure | Finding | Frequency |
|---|---|---|
| Subcutaneous tissue under groove | Dry, white, glistening; haemorrhage rare | Common |
| Strap muscles (sternomastoid, platysma) | Haemorrhage in muscle fibres; rupture in ~10-15% cases with considerable violence | Relatively common |
| Carotid arteries | Transverse intimal tears (most important vascular finding); in long-drop hangings, tears at multiple levels | Uncommon but diagnostically significant |
| Vertebral arteries | Rupture possible, particularly with long drop | Rare |
| Hyoid bone | Fracture in 15-20% of cases (more common >40 years of age, rare below 40 due to cartilage elasticity); typically at the greater horn at the junction of inner 2/3 and outer 1/3 | 15-20% |
| Thyroid cartilage | Fracture in 40-45% of cases; superior horn fracture is most common; thyrohyoid ligament may be torn | 40-45% |
| Cervical spine | Fracture is very rare in non-judicial hanging (<1-3%); seen only in obesity with advanced cervical osteoarthritis and sudden drop | Rare |
| Epiglottis/larynx/trachea | Petechial haemorrhages on visual inspection | Seen |
| Overall | No internal injuries in >50% of all hanging deaths | >50% |
- Fractures of the hyoid and thyroid cartilage are accepted as antemortem when there is blood at the fracture site (indicating vital reaction).
- Absence of internal injuries does not exclude antemortem hanging.
D. General Post-Mortem Findings in a Complete Hanging Case
| Finding | Explanation |
|---|---|
| Post-mortem lividity | Circumferential on dependent arms, forearms, hands, legs. Above the ligature on face/neck, lividity may be present in head - later shifts to the back when the body is laid down. |
| Tardieu spots | Punctate haemorrhages from hydrostatic rupture of vessels in the dependent lower limbs - an indicator of duration of suspension. |
| Genitalia | Penile engorgement from hypostasis; ejaculation/semen at meatus possible. |
| Sphincter relaxation | Urine and/or faeces may be expelled. |
| Clenched hands | Particularly in violent or prolonged hanging. |
E. Summary Correlation Table for a "Complete Typical Hanging" Case
| Feature | Expected Finding | Reason |
|---|---|---|
| Face colour | Pale | Complete carotid + vertebral occlusion |
| Facial petechiae | Absent or rare | No arterial pooling in head |
| Tongue | Protruding, dark brown/black | Lifted by noose + drying |
| Saliva | Dribbling from angle of mouth (side opposite knot) | Salivary gland stimulation - antemortem sign |
| Ligature mark course | Oblique, upward - inverted V - missing at occiput | Knot placed posteriorly in typical hanging |
| Deepest part of mark | Anteriorly (front of neck) | Opposite to occipital point of suspension |
| Ligature mark level | Above thyroid cartilage | Noose typically slips to below chin/larynx |
| Internal neck injuries | Absent in majority (>50%) | Relatively low force required |
| Hyoid fracture | 15-20% | More likely with age/force |
| Thyroid cartilage fracture | 40-45% | Superior horn, especially |
| Cervical spine fracture | Rare | Only in judicial or drop hangings |
Sources:
- DiMaio's Forensic Pathology, 3rd Ed. (pp. 265-270)
- The Essentials of Forensic Medicine and Toxicology, 36th Ed. (pp. 337-339)
- Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology (pp. 204-206)
- P.C. Dikshit - Textbook of Forensic Medicine and Toxicology (pp. 291-296)
Define hanging. Describe the types of hanging (complete vs. partial, typical vs. atypical, etc.) and enumerate the post-mortem features of each type.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed for a comprehensive, well-illustrated answer. Let me compile it.
Hanging: Definition, Classification, and Post-Mortem Features by Type
I. Definition
Hanging is a form of violent (mechanical) asphyxia caused by the suspension of the body by a ligature that encircles the neck, the constricting force being the weight of the body itself. The ligature constricts the neurovascular bundles of the neck and/or the upper airway. It is the most common method of suicide worldwide; homicidal hanging is extremely rare.
"Hanging is always suicidal in nature, unless the contrary is proved beyond reasonable doubt." - The Essentials of FMT, 36th Ed.
II. Classification of Hanging
Hanging is classified along four independent axes:
| Axis | Types |
|---|---|
| Degree of suspension | Complete vs. Partial |
| Position of knot | Typical vs. Atypical |
| Mode/circumstance | Suicidal, Homicidal, Accidental, Judicial, Autoerotic |
| Type of noose | Running noose (slip knot) vs. Fixed noose (binding knot) |
III. Classification by Degree of Suspension
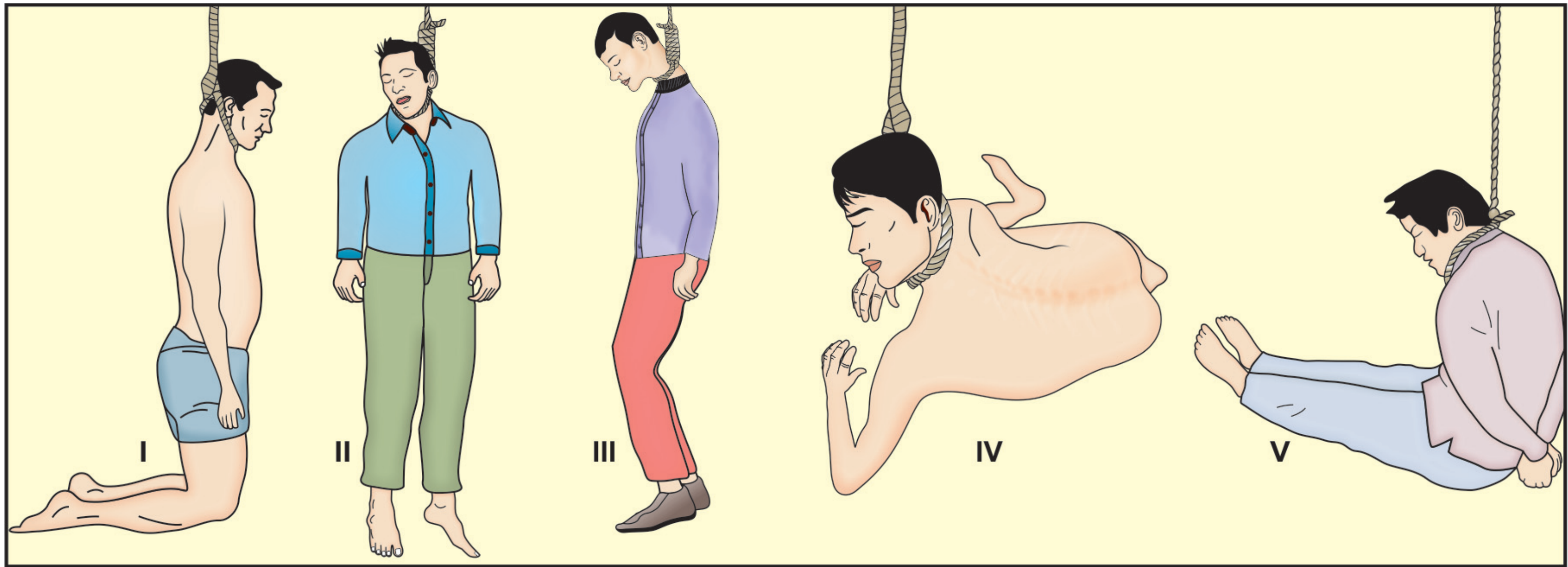
Fig: Positions in hanging — (I) kneeling/partial, (II) complete, (III) feet just touching, (IV) prone, (V) sitting. [Parikh's Textbook of MJ, FMT]
A. COMPLETE HANGING
Definition: The entire body is freely suspended in air, and the whole body weight (typically 60-80 kg) acts as the constricting force. No part of the body touches the ground.
Mechanism of death: Primarily cerebral ischaemia from simultaneous occlusion of both carotid arteries (occluded at ~3.5 kg) and jugular veins (occluded at ~2 kg). Because all cervical vessels - including vertebral arteries - are compressed by the full body weight, blood supply to the brain is completely cut off. Death follows within 3-5 minutes.
Post-Mortem Features of Complete Hanging
External - Face:
- Face is PALE (hallmark feature) - due to complete occlusion of both carotids and vertebral arteries; no blood pools in the head
- Petechial haemorrhages are ABSENT or minimal in the face and conjunctivae - because there is no residual arterial pressure to rupture capillaries in the head
- Eyeballs may be slightly prominent; pupils dilated
- Tongue - protruding, dark brown to black tip (drying), swollen base
- Lips and oral mucosa cyanosed
- Saliva dribbling from the angle of the mouth (side opposite the knot)
- Le facie sympathique may be present if knot compresses the cervical sympathetic
External - Neck:
- Neck stretched and elongated; head tilted away from the knot
- Ligature mark: Oblique, running upward toward knot; incomplete (absent/faint at the nape); deep and well-defined anteriorly; parchment-like yellow-brown colour; deepest portion opposite the knot
Post-mortem lividity:
- Absent on the face (blood drained away)
- Circumferential on the dependent forearms, hands, and lower legs
- Tardieu spots (petechial hemorrhages from hydrostatic vessel rupture) may develop in the lower limbs after several hours of suspension
Internal Neck:
- Tissues under the groove are dry, white, and glistening (no blood due to compression)
- Strap muscle haemorrhages in ~17-25% of cases
- No injuries in >50% of cases (the low forces needed mean the neck can be compressed fatally without structural damage)
- Hyoid bone fracture in ~15-20% (rare below age 40; more common at the greater horn)
- Thyroid cartilage fracture in ~40-45% (superior horns most commonly)
- Carotid artery intimal tears (5-10%) - antemortem indicator
- Cervical spine fracture: extremely rare in non-judicial hanging
B. PARTIAL (INCOMPLETE) HANGING
Definition: The body is only partly suspended. A part of the body - toes, feet, knees, buttocks, or the entire lower half - touches the ground. The constricting force is the weight of the head only (~5-6 kg) or head + chest.
Fig: Partial hanging - kneeling position [Dikshit's Textbook of FMT]
Variants:
- Partial standing (toes or feet just touching the ground)
- Sitting (body seated with neck in noose)
- Reclining / kneeling (lying prone with chest off the ground)
- Hanging from a bedpost, doorknob, or low fixture
Key physiological difference from complete hanging: In partial hanging, the constricting force is relatively small (5-6 kg), sufficient to occlude the carotid arteries (~3.5 kg) and jugular veins (~2 kg) but not the vertebral arteries (~16.6-30 kg). Therefore:
- Venous return from the head is blocked
- But the vertebral arteries continue to supply blood to the head
- This creates a net increase in intracranial pressure
Post-Mortem Features of Partial Hanging
External - Face (KEY DIFFERENCES from complete hanging):
- Face is CONGESTED, swollen, and cyanosed - dusky purple/plum colour (due to venous obstruction with continued vertebral arterial supply)
- Petechial haemorrhages are COMMON and prominent - on the face, eyelids, conjunctivae, and skin of the neck above the ligature
- The congested face may show periorbital oedema and facial puffiness; swelling often disappears when the body is cut down
- Eyes - prominent, firmly protruding, conjunctival haemorrhages
- Tongue - deeply cyanosed and protruding
- Decomposition sets in earlier in partial hanging due to the congested, blood-filled head
External - Neck:
- Ligature mark is less prominent, shallower, or even absent - because the constricting force is low
- Mark may be found at a lower level on the neck (below the thyroid cartilage) compared to complete hanging
- The oblique, upward, inverted-V pattern is preserved if the knot is posterior, but the mark may be faint or indistinct
- With soft materials (towel, dupatta), no mark may be visible at all
Post-mortem lividity:
- Present on the face and head (above the ligature)
- Also in the dependent lower limbs
- Tardieu spots more prominent in the lower limbs
Signs of asphyxia: Most marked in partial hanging; petechiae are much more frequent than in complete hanging.
IV. Classification by Position of the Knot
C. TYPICAL HANGING (Knot at the Occiput)
Definition: The knot (point of suspension) is situated at the central occipital region (back of the neck/nape). The ligature runs symmetrically upward from the midline of the front of the neck, along both sides, to meet at the occiput.
Physiology: With the knot at the occiput, maximum pressure is applied to the front and sides of the neck - directly over the carotid arteries and jugular veins, producing rapid carotid occlusion and cerebral ischaemia. Asphyxial changes are slight because both arterial and venous systems are occluded simultaneously.
Post-Mortem Features of Typical Hanging
Ligature mark (characteristic pattern):
- Runs obliquely upward from the front of the neck toward the mastoid processes behind each ear
- Directed along the line of the mandible
- Inverted V shape with the apex of the V pointing toward the occiput
- Mark is present on the front and both sides of the neck
- Absent or faintest at the nape (where the two limbs of the ligature converge at the knot and the firm neck muscles/hair intervene)
- Deepest and most prominent anteriorly (opposite to the knot)
- Level: Above the thyroid cartilage (in ~80% of cases; at the level in 15%; below in only 5%)
Face:
- Pale (in complete + typical hanging) - the combined occlusion of all cervical vessels including vertebrals
- Asphyxial signs are minimal
- Saliva dribbles from the angle of the mouth on the side opposite the knot (from the ligature compressing the ipsilateral salivary gland)
Internal: Tissues under the groove anteriorly are dry and white; fractures of hyoid/thyroid may be present as above.
D. ATYPICAL HANGING (Knot NOT at the Occiput)
Definition: The knot is situated anywhere other than the occiput - on the right side, left side, or front (chin) of the neck.
- Knot on one side (most common variant): The ligature mark is asymmetric. The mark is deepest on the side opposite the knot and is more oblique. The head tilts toward the side of the knot.
- Knot under the chin (anterior): The ligature runs horizontally around the neck; the mark may completely encircle the neck horizontally (resembling a ligature strangulation mark). This is the most important variant forensically because it can cause diagnostic confusion.
Post-Mortem Features of Atypical Hanging
Ligature mark:
- Knot on one side: Oblique course, but asymmetric - mark on the opposite side is deepest and best defined; site of knot shows an indentation or abrasion. Head inclined toward the knot. Conjunctival petechiae may be unilateral (on the side opposite the knot).
- Knot anteriorly (under chin): Mark runs more horizontally and may completely encircle the neck - this pattern mimics ligature strangulation. Differential diagnosis rests on: direction of mark (oblique = hanging; horizontal = strangulation), level of mark (hanging above thyroid cartilage; strangulation below thyroid), and scene findings.
Face:
- When the knot is in front, venous drainage may be predominantly blocked while arterial supply via vertebrals is maintained - producing more congestion and petechiae than typical hanging
- Conjunctival haemorrhages may be one-sided when the knot is over one ear
Medicolegal note: Atypical anterior hanging can be erroneously diagnosed as ligature strangulation. The scene findings (suspended body, type of knot) are critical.

Fig: Ligature mark of hanging after removal of ligature - note the oblique groove [Dikshit's Textbook of FMT]
V. Classification by Mode/Circumstance
E. SUICIDAL HANGING
Most common mode. Features:
- Any available ligature material used
- Point of suspension: ceiling fan, roof beam, window bars, door, tree
- Simple slip-knot (running noose) most common
- Room often bolted from inside; suicide note may be present
- Usually no other injuries; occasionally self-tied hands to prevent change of mind
- PM features as above (complete/typical combination most common)
F. ACCIDENTAL HANGING
- Most commonly in children caught in cribs, furniture, clothing
- In adults: autoerotic asphyxia (sexual hanging) - elaborate restraints, padded noose, evidence of sexual activity
- In autoerotic cases, soft padded noose may leave faint marks; position may be unusual
G. HOMICIDAL HANGING (Extremely Rare)
- Virtual impossibility between two healthy adults of equal strength unless victim is incapacitated (beaten, intoxicated, drugged)
- Possible in: children, very frail persons, unconscious victims
- Ligature mark may not show classic inverted-V; may be horizontal (victim hanged after strangulation)
- Other injuries of assault may be present
- Toxicological screen mandatory in all alleged suicides to rule out drug-facilitated hanging
H. JUDICIAL HANGING
- Involves a deliberate long drop (calculated based on body weight, typically ~5 meters)
- Knot placed on the left side of the jaw near the chin; trapdoor is released
Specific PM features distinct from civil hanging:
- Fracture-dislocation of cervical vertebrae - at C2-C3 level ("hangman's fracture"), or atlanto-occipital/atlanto-axial joint; this fracture is actually uncommon even in judicial hanging (most victims show no fracture at all on autopsy, per postmortem studies)
- Instantaneous loss of consciousness and death due to cord transection
- Neck markedly elongated; may be severed from the body if the fall is too great
- Neck vessels (carotids, vertebrals) torn transversely
- Multiple intimal tears of carotid arteries at different levels (due to the long-drop traction force)
- Muscular contractions, facial twitching, and limb convulsions occur at the moment of the drop
- Heart may continue to beat for 8-20 minutes after unconsciousness
- X-ray: bilateral fractures of pedicles or laminae of arch of C2/C3/C4 with dislocation
- Ligature mark: Horizontal (knot placed anteriorly under chin/jaw), well-defined, at the level of the upper neck; may completely encircle the neck
VI. Comparative Summary Table
| Feature | Complete + Typical | Partial Hanging | Atypical (Knot anterior) | Judicial Hanging |
|---|---|---|---|---|
| Face colour | Pale | Congested/purple | Congested (variable) | Pale |
| Petechiae (face/conjunctiva) | Rare/absent | Prominent, frequent | More common | Rare |
| Tongue | Protruding, black tip | Dark, swollen | Variable | Variable |
| Ligature mark course | Oblique upward, inverted-V | Oblique but faint | Horizontal, may encircle | Horizontal |
| Ligature mark level | Above thyroid cartilage | At or below thyroid | Upper neck | Upper neck |
| Mark at back of neck | Absent/faint (nape) | Present | Present | Present |
| Deepest part of mark | Anteriorly | Variable, faint | Posteriorly | Anteriorly |
| Asphyxial signs | Mild | Marked | Moderate-marked | Absent (rapid death) |
| Cervical fracture | Very rare | Very rare | Very rare | Present (C2-3) |
| Hyoid fracture | 15-20% | Rare | Variable | May be present |
| Thyroid fracture | 40-45% | Less common | Variable | Yes |
| Neck elongation | Yes | Less | Variable | Marked, may be severed |
| Carotid intimal tears | 5-10% | Rare | Variable | Multiple, at various levels |
| Lividity | Lower limbs | Face + lower limbs | Head + neck | Lower limbs |
| Mode | Usually suicidal | Suicidal/accidental | Suicidal (can mimic strangulation) | Execution |
VII. Ligature Mark - Factors Affecting Appearance (Common to All Types)
- Ligature material - hard/thin rope: deep, narrow, distinct; soft/broad cloth: shallow, wide, ill-defined
- Duration of suspension - longer suspension = deeper, more prominent groove
- Type of hanging - complete > partial in prominence
- Tightness - tighter = deeper mark
- Position of knot - deepest mark is always opposite the knot
- Slipping of ligature - may produce a double impression
- Presence of beard/hair/clothing - may prevent mark formation under it
- Post-mortem changes - mark resists putrefaction; disappears if ligature removed soon after death; fades in decomposition
Sources:
- The Essentials of Forensic Medicine and Toxicology, 36th Ed., pp. 334-345
- P.C. Dikshit - Textbook of Forensic Medicine and Toxicology, pp. 291-298
- Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology, pp. 204-210
- DiMaio's Forensic Pathology, 3rd Ed., pp. 263-275
Lightning Injury - mechanism, Death due to Lightning - autopsy; Lightning Fatalities
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive material from all major sources. Let me compose the full, detailed answer.
Lightning Injury: Mechanism, Death, Autopsy, and Fatalities
I. Definition and Physics of Lightning
Lightning is a natural electrical discharge from the atmosphere to the earth, occurring when sufficient potential difference builds between a charged thundercloud and the ground. The undersurface of a thundercloud is usually negatively charged; positively charged ions rising from the earth move upward and collide with the descending negative ions at about 30-40 feet above ground, producing the discharge.
Physical characteristics of a lightning bolt:
- Current: ~20,000 amperes (range: kiloampere range on direct strike)
- Voltage: 100 million to 1,000 million volts (100 MV - 1,000 MV)
- Duration: Approximately 1/1,000th of a second (30 microseconds average contact time)
- Polarity: ~95% are negative discharges; ~5% are positive discharges (more common in mountainous regions and more dangerous)
- Although a flash appears single, research shows multiple strikes occur in rapid succession, cloud-to-earth and earth-to-cloud, appearing as one
Lightning vs. human-generated electricity: Lightning involves vastly higher voltage but an extremely brief contact duration. This brevity fundamentally changes the injury pattern - most energy passes over the victim rather than through them (the "flashover effect"), making lightning paradoxically less destructive to internal tissues than lower-voltage industrial electrical accidents.
II. Mechanisms of Injury (Types of Lightning Strikes)
Lightning injures in five distinct ways:
1. Direct Strike
The victim is struck directly by the lightning discharge. Most lethal mechanism; amperage is in the kiloampere range. Death is almost certain with a head-on direct hit.
2. Side Flash (Side Splash / Ricochet)
Lightning strikes a nearby object (most commonly a tree) and then ricochets through the air to strike the person standing nearby. Side flashes may travel up to 30 metres and can injure multiple victims simultaneously (e.g., a group sheltering under a tree).
3. Contact Voltage (Conducted Strike)
The bolt strikes an object the victim is holding or touching (e.g., a golf club, umbrella, telephone, crane, fence). Current travels from the struck object through the person to ground. Produces burns at entry and exit points similar to high-voltage industrial injuries.
4. Ground Current (Stride Potential / Step Voltage)
Lightning strikes the ground and current radiates outward along the earth's surface. The foot closer to the strike point is at a higher electrical potential than the other foot. Current enters one foot, travels up one leg, through the torso, and exits the other leg - producing isolated neurovascular injury to the lower limbs. This mechanism causes mass cattle deaths in open pastures.
5. Upward Streamer (Rare)
A weak upward streamer from the victim does not complete connection to the downward lightning channel, but the electromagnetic energy is still sufficient to produce fatal injury. Recently implicated in fatal cases.
III. Four Factors Governing Lightning Injury
- Direct electrical effect - current passing through the body to earth
- Surface flash burns - discharge travelling over the body surface
- Mechanical (blast) effect - violent displacement of air by thermal expansion around the flash; produces a concussive blast wave
- Compression effect - the return wave of air causes additional pressure injury
IV. Mechanism of Tissue Injury
The Flashover Effect (Dominant Mechanism)
Lightning most commonly travels over the surface of the body rather than through it - a phenomenon called flashover. This explains:
- Why most victims (~70-90%) survive
- Why deep muscle necrosis is rare (unlike industrial electrical injury)
- Why wet skin paradoxically reduces internal injury - wet skin acts as a better external conductor, keeping current on the surface
Direct Internal Injury Mechanisms
- Blunt mechanical force from the blast
- Direct current flow through body causing cardiac depolarization and respiratory centre paralysis
- Induction of current - the massive current in lightning creates a pulsed magnetic field that induces current flow in a nearby person even without direct contact
- Thermal injury - steam from rapid vaporisation of skin moisture, resistance heating of metal objects on/in clothing, heating of deeper tissues
- Intense photic stimulation - may damage retina or produce cataracts
V. Clinical Effects and Specific Organ Injuries
Cardiac
- Immediate cardiac arrest from massive depolarisation of the entire myocardium producing asystole (not ventricular fibrillation as in low-voltage AC current)
- Cardiac automaticity may spontaneously return, but if respiratory arrest persists, secondary hypoxic cardiac arrest follows
- In survivors: hypertension, tachycardia, various dysrhythmias (atrial fibrillation, PVCs, bundle branch blocks, non-specific ST-T changes on ECG)
Respiratory
- Immediate respiratory arrest from depolarisation and paralysis of the medullary respiratory centre
- Both cardiac and respiratory arrest may be present without any external injury
- The respiratory centre may remain paralysed longer than the heart - aggressive prolonged CPR is warranted
Neurological - Keraunoparalysis (Lightning Paralysis)
A distinctive neurological syndrome unique to lightning:
- Transient, immediate paralysis predominantly of the lower limbs (greater than upper limb weakness)
- Associated with extreme vasoconstriction - limbs pale, cold, pulseless (mimicking arterial injury)
- Sensory abnormalities of extremities
- Autonomic dysfunction may produce pupillary dilation or anisocoria - these are NOT reliable indicators of brain injury in comatose lightning-strike victims; they have no prognostic significance
- Amnesia and neurotic/confused behaviour may persist
- Usually resolves within 1 hour to a few days
- Associated with successful resuscitation after cardiorespiratory arrest
Ear
- Tympanic membrane rupture in approximately 81% of lightning victims (from barotrauma - air expands when superheated by the strike)
- Haemorrhage into the middle ear
Eye
- Thermal or photic retinal damage
- Cataracts (may develop days to months later)
Skin
See Section VII (Autopsy findings) for full skin injury details.
Musculoskeletal
- Thrown by the blast - fractures from blunt trauma
- Scapular, humeral, femoral neck fractures from violent tetanic muscle contraction
- Vertebral fractures possible
VI. Cause of Death
Death from lightning can occur by any of the following mechanisms (in order of importance in non-judicial/civil lightning strikes):
- Cardiopulmonary arrest - the most common immediate cause; massive myocardial depolarization causes asystole; simultaneous respiratory centre paralysis means both fail together
- Direct electrothermal injury to vital structures from high-voltage direct current
- CNS injury - direct involvement of the brain stem with paralysis of the cardiac or respiratory centre; subarachnoid and intracerebral haemorrhage
- Asphyxia - secondary to sustained respiratory arrest (medullary centre paralysis)
- Delayed death may occur from: aspiration pneumonia, hypoxic encephalopathy, cerebral oedema, sepsis from burns, thrombotic vascular complications
With a direct hit, death from burns and respiratory centre damage is almost inevitable. With a close but indirect strike, survival is possible - most lightning-injured individuals do survive.
VII. Autopsy Findings in Lightning Fatalities
A. External Findings
1. Clothing and General Appearance
- Clothing is torn, burned, or may be completely stripped off the body and thrown some distance; this can create suspicion of criminal violence
- Clothes are typically burnt or torn at the points of entry and exit of current
- In exceptional cases, clothing may be undamaged even when the person is killed, or conversely, clothing may be burnt with no injury to the person
- Shoes burst open or torn, especially at the sole (exit point through the feet)
- Belt and boots may be ruptured
2. Burns
Three types of burns are characteristic:
(a) Linear Burns
- Zigzag or irregular linear burns, 3-30 cm or more in length, 0.3-2.5 cm in breadth
- Found preferentially in moist creases and skin folds (axillae, groin, popliteal fossae) because moist areas offer less resistance and conduct the surface current
- Also called filigree burns (filiform/thread-like pattern along skin)
- True superficial burns, often first-degree (erythema only)
(b) Arborescent / Filigree Burns - Lichtenberg Figures (PATHOGNOMONIC)

Fig: Lichtenberg figures / arborescent burns from lightning strike [DiMaio's Forensic Pathology, 3rd Ed.]

Fig: Filigree burns in a lightning strike case [Dikshit's Textbook of FMT]
- Pathognomonic (considered diagnostic) for lightning injury
- Superficial, thin, irregular and tortuous fern-like markings on the skin, resembling the branches of a tree or a fern leaf
- Appear within minutes to 1 hour of the incident
- Usually found over the shoulders, flanks, trunk, and chest
- Described as green in colour in some texts (due to copper-haemoglobin reaction)
- Mechanism: Produced by electron showers from the lightning, or by rupture of smaller superficial blood vessels giving ecchymoses in the arborescent pattern; boiling of intercellular fluid along fascial planes; haemoglobin from lysed RBCs staining the skin along the path of current. Possibly due to positive discharge flashover on the skin.
- They are not deep burns but rather areas of transient erythema / very superficial skin change
- Disappear within 1-2 days if the person survives - they must be documented immediately at autopsy as they fade rapidly
- Their relative rarity in autopsy is explained by: (a) they occur more with positive lightning discharges (only 5% of strikes), and (b) they fade quickly
(c) Surface Burns (Thermal Burns from Metal Objects)
- True thermal burns occurring beneath metallic objects worn or carried by the victim (rings, chains, spectacle frames, pen-knives, keys, watches, zip fasteners, belt buckles)
- These metal objects are superheated or even melted/fused by the flash
- Burns at these contact points are deeper and correspond in shape to the overlying metal
3. Entry and Exit Marks
- In cases where current enters and exits the body, entry marks (small, punched-out, charred) and exit marks (often larger, explosive-appearance) may be found
- Entry marks may be at the head (direct strike), point of contact with a conducted object
- Exit most commonly at the feet, causing burst shoes
4. Hair
- Hair is singed or seared at the point of entry; hair may be burnt off
- May form a characteristic pattern near the entry zone
5. Miscellaneous External
- Extensive ecchymoses of the trunk skin (from mechanical blast effect)
- Contusions, lacerations from being thrown or from blast injury
- Fractures (may be misinterpreted as assault)
- Ruptured tympanic membrane (found in ~81% of cases); bleeding from the ear
- Metallic objects fused or magnetised - ferrous metals (keys, coins, watches) on the body may be magnetised (diagnostic finding); nylon clothing may be melted
- Rigor mortis appears soon after death and passes off quickly

Fig: Burns due to lightning on the chest [Essentials of FMT, 36th Ed.]
B. Internal Findings
Internal findings are not very characteristic in lightning fatalities compared to the striking external findings. However:
Cardiovascular:
- Haemorrhages under the pleura and pericardium (petechial/ecchymotic)
- Blood vessels may be thrombosed or ruptured
- Lungs are congested and oedematous, exude bloody serum (signs of asphyxia)
Central Nervous System:
- Leptomeninges congested or lacerated
- Brain may be congested or oedematous
- Subarachnoid and intracerebral haemorrhage may occur
- The respiratory and cardiac centres in the medulla may show direct injury
Ear:
- Tympanic membrane rupture with haemorrhage in the middle ear
Neck and soft tissue under mark:
- Tissues under the lightning mark are dry and whitened (histological: epidermis separated from papillary dermis)
- Ecchymoses in adjacent muscles
Skeletal:
- Fractured bones (multiple sites - from blast, fall, or tetanic muscular contraction)
Pulmonary:
- Pulmonary haemorrhages and oedema
- Parenchymal necrosis
In survivors who die later:
- Internal vessels show clots and thrombi
- Affected organs show necrosis and gangrene
- Intense oedema at the point of current entry
VIII. Lightning Fatalities - Epidemiology and Medicolegal Aspects
Epidemiology
- Lightning causes approximately 500 injuries per year in the USA, with 20-50 deaths per year
- Approximately 70-90% of persons struck by lightning survive; however, up to three-quarters of survivors have permanent sequelae
- Less than 3% of weather-related deaths are due to lightning (heat and cold are more deadly)
- Most deaths occur in outdoor settings: open fields, under trees, on water (fishing, boating), golf courses, camping
- Fishermen are the most commonly affected occupational group
- Lightning can occur without rain in approximately 10% of cases (so-called "bolt from the blue")
- Less than half of persons struck by lightning in India are killed
High-Risk Situations
- Standing in open fields or on hilltops
- Taking shelter under isolated tall trees
- Carrying or wearing metal objects (golf clubs, umbrellas, jewellery)
- Near metal fences, bleachers, plumbing, power lines, metal-topped structures
- On open water (boat, swimming)
- Indoor use of telephone or other wired electronics during a storm (contact voltage through wiring)
- Taking shelter in a doorway or window with an open chimney
Medicolegal Importance
- Manner of death is always ACCIDENTAL - there are no recorded cases of homicidal or suicidal lightning death
- The appearances can closely resemble criminal violence - contusions, lacerations, disarranged and torn clothing, fractured bones. A body found in a field with torn clothing and multiple injuries may initially be thought to be a homicide victim
- Diagnosis rests on:
- History of a thunderstorm in the vicinity at the time of death
- Environmental evidence: damaged/burnt trees, dead cattle, scorched ground near the body
- Arborescent/filigree burns (pathognomonic) on the body
- Magnetised metallic objects on the victim's person
- Torn, burnt, or stripped clothing and burst shoes
- Burns beneath metal articles on the person
- Exclusion of all other causes of death at autopsy
- Persons in metal-bodied vehicles (cars, lorries) are generally safe - the charge travels over the metal surface rather than through the interior (Faraday cage effect)
- Persons in buildings are generally safe as lightning passes along the outside of a conductor; however, indoor deaths have occurred via chimneys, aerials, plumbing, and telephone wires
- Forensic pitfall: Magnetisation of ferrous objects and fusion of nylon or metal - these findings can help confirm lightning death and eliminate suspicion of foul play
Summary of Distinguishing Features of Lightning vs. Electrical Injury
| Feature | Lightning | Human-generated Electrical |
|---|---|---|
| Voltage | 100 MV - 1,000 MV | Variable (domestic: 240V; industrial: up to tens of kV) |
| Current | Kiloamperes (~20,000 A) | Lower |
| Duration | ~30 microseconds | Prolonged (seconds to minutes) |
| Current type | DC (direct) | Usually AC |
| Flashover | Common - protects victim | Absent |
| Deep muscle necrosis | Rare | Common |
| Entry/exit burns | May be present | Common (Joule burns) |
| Arborescent burns | Pathognomonic | Not seen |
| Magnetisation of metals | Present | Absent |
| Internal injuries | Less severe | Often severe |
| Survival | 70-90% survive | Variable, often lower |
| Manner of death | Always accidental | Accidental/suicidal/homicidal |
| Cause of cardiac arrest | Asystole (depolarisation) | VF (AC current) |
Sources:
- DiMaio's Forensic Pathology, 3rd Ed. (pp. 406-407)
- The Essentials of Forensic Medicine and Toxicology, 36th Ed. (pp. 326-329)
- P.C. Dikshit - Textbook of Forensic Medicine and Toxicology (pp. 246, 291)
- Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology (pp. 393-394)
- Tintinalli's Emergency Medicine, A Comprehensive Study (pp. 1311-1375)
- Rosen's Emergency Medicine, Concepts and Clinical Practice (pp. 3698-3710)
This is a shared conversation. Sign in to Orris to start your own chat.