Conventional/Unfractionated Heparin and Low Molecular Weight Heparin - differences
Reading File
Finding Sources
Searching PubMed
"unfractionated heparin" AND "low molecular weight heparin" AND comparison
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
I now have comprehensive data to compose a thorough comparison. Let me compile the full answer:
Unfractionated Heparin (UFH) vs. Low Molecular Weight Heparin (LMWH)
1. Source and Structure
| Feature | UFH | LMWH |
|---|---|---|
| Source | Porcine intestinal mucosa (biologic) | Depolymerized from UFH (biologic) |
| Molecular weight | 5,000-30,000 Da (mean ~15,000) | 1,000-10,000 Da (mean ~4,500-6,000) |
| Chain length | Long - nearly all chains can bridge AT to thrombin | Short - at least half are too short to bridge AT to thrombin |
| Structure | Heterogeneous mixture of sulfated polysaccharides | More uniform, shorter polysaccharide chains |
UFH is a heterogeneous mix of sulfated mucopolysaccharide chains. LMWH agents (enoxaparin, dalteparin, tinzaparin) are produced by controlled depolymerization of UFH, generating shorter, more uniform fragments.
2. Mechanism of Action
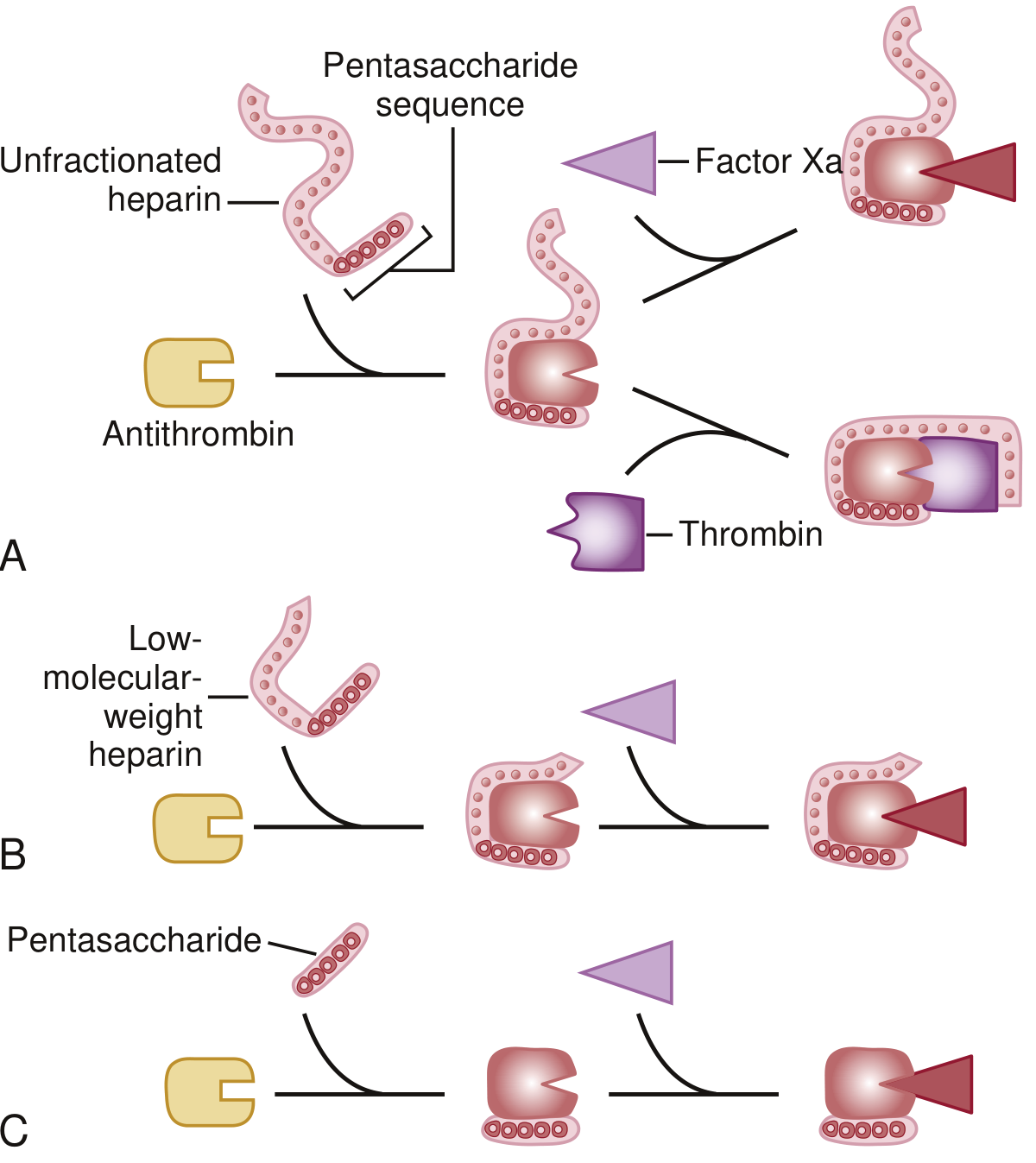
Both drugs work via antithrombin (AT) - a serine protease inhibitor synthesized in the liver. Both contain a unique pentasaccharide sequence that binds AT, inducing a conformational change in its reactive center loop that accelerates its inhibitory activity by at least 100-fold.
The key difference is chain length:
-
UFH - Mean MW ~15,000 Da. All chains are long enough (≥18 saccharide units) to simultaneously bind AT and thrombin, forming a ternary complex. UFH therefore inhibits both thrombin (IIa) and Factor Xa equally (anti-Xa:anti-IIa ratio = 1:1). It also inhibits factors IXa, XIa, and XIIa. Additionally, UFH causes release of tissue factor pathway inhibitor (TFPI) from the endothelium.
-
LMWH - Mean MW ~4,500-6,000. At least half of chains are too short to bridge antithrombin to thrombin. They can still accelerate inhibition of Factor Xa (via the pentasaccharide-AT conformational change), but cannot form the ternary complex needed to inhibit thrombin. Result: anti-Xa:anti-IIa ratio = 2:1 to 4:1 depending on the specific agent. Longer LMWH chains (e.g., tinzaparin) retain somewhat more anti-IIa activity.
Braunwald's Heart Disease, p. 1127; Katzung's Basic & Clinical Pharmacology, 16e, p. 959
3. Pharmacokinetics
| Parameter | UFH | LMWH |
|---|---|---|
| Bioavailability (SC) | ~30% (poor - large chains bind endothelium) | ~90% (excellent) |
| Half-life | 30-60 min (dose-dependent, non-linear) | ~4 hours (predictable, linear) |
| Clearance mechanism | Saturable - binds endothelial cells + macrophage degradation; dose-dependent | Primarily renal (fixed, non-saturable) |
| Plasma protein binding | Extensive (fibrinogen, vWF, PF4, acute-phase proteins) | Minimal |
| Response predictability | Unpredictable - variable due to protein binding | Predictable - weight-based dosing gives reliable levels |
UFH's dose-dependent clearance means its half-life is short at low doses (~30 min) and longer at higher doses (~60 min). The extensive binding to plasma proteins (including platelet factor 4 from activated platelets within thrombi) reduces its effective activity - this is a major pharmacokinetic limitation.
Braunwald's Heart Disease, p. 1127-1128
4. Monitoring
| UFH | LMWH | |
|---|---|---|
| Routine monitoring | Mandatory - aPTT (target 2-3x control, ~60-100 sec) | Not routinely required |
| Alternative monitoring | Anti-Xa levels (0.3-0.7 IU/mL) | Anti-Xa levels (0.5-1.0 IU/mL peak) when needed |
| When to monitor LMWH | N/A | Renal insufficiency, obesity, pregnancy |
| Test used for LMWH when needed | N/A | Anti-Xa levels (NOT aPTT) |
Because LMWH has minimal anti-IIa activity, aPTT is not a useful monitor for LMWH. Up to 25% of patients on UFH are "heparin resistant," requiring >35,000 units/day to achieve a therapeutic aPTT - in these patients, anti-Xa levels may be therapeutic even when aPTT is subtherapeutic (due to elevated acute-phase reactants shortening the aPTT).
Braunwald's Heart Disease, p. 1128; Katzung, p. 960
5. Administration
| UFH | LMWH | |
|---|---|---|
| Routes | IV infusion (preferred for treatment) or SC | SC only (enoxaparin also approved IV in some ACS protocols) |
| Dosing frequency | Continuous IV infusion or SC 2-3x/day (prophylaxis) | SC once or twice daily |
| Dose titration | Required - nomogram-guided | Fixed weight-based (e.g., enoxaparin 1 mg/kg SC q12h) |
| Hospital setting | IV infusion requires inpatient monitoring | SC dosing allows outpatient treatment |
6. Reversal
| UFH | LMWH | |
|---|---|---|
| Antidote | Protamine sulfate - complete reversal (1 mg neutralizes ~100 units UFH) | Protamine sulfate - partial reversal only (~60-75% of anti-Xa activity) |
| Why partial? | Protamine binds long chains well | Short LMWH chains bind protamine poorly |
This is clinically important: if a patient on LMWH has major bleeding or needs emergency surgery, protamine only partially reverses anticoagulation. Andexanet alfa (recombinant modified Factor Xa) has been studied as a reversal agent for anti-Xa agents but is most established for oral Factor Xa inhibitors.
7. Side Effects and Complications
Heparin-Induced Thrombocytopenia (HIT)
| UFH | LMWH | |
|---|---|---|
| HIT incidence | <5% (up to 3-5% in surgical patients) | <1% |
| Mechanism | IgG antibodies against heparin-PF4 complexes → platelet activation → thrombocytopenia + paradoxical thrombosis | Same mechanism, but less antigen formation due to shorter chains |
| Cross-reactivity | - | LMWH antibodies cross-react with UFH; cannot simply substitute LMWH if HIT occurs |
HIT typically presents as platelet count falling to 50,000-70,000/mm³ within 5-15 days of starting heparin. Despite thrombocytopenia, the hallmark is thrombosis (paradoxical pro-thrombotic state). Immediate discontinuation and switching to a direct thrombin inhibitor (argatroban, bivalirudin) is required.
Osteoporosis
- Prolonged use of UFH (>1 month) causes osteoporosis by inhibiting osteoblasts and activating osteoclasts. Fracture risk is clinically meaningful.
- LMWH has lower risk of osteoporosis - preferred for anticoagulation in pregnancy requiring long-term therapy.
Bleeding
- Most common side effect of both. Higher doses = higher risk.
- Concomitant antiplatelet agents or fibrinolytics increase risk.
Elevated transaminases
- Mild AST/ALT elevations occur with both; not usually clinically significant.
8. Biophysical Limitations of UFH (not shared by LMWH to the same extent)
From Braunwald's Heart Disease (Table 95.4):
| Limitation | Mechanism |
|---|---|
| Poor SC bioavailability | Long chains bind endothelial cells at injection site |
| Dose-dependent clearance | Endothelial cell binding saturates at high doses |
| Variable anticoagulant response | Binds many plasma proteins; levels vary between patients |
| Reduced activity near thrombus | Neutralized by PF4 from activated platelets |
| Cannot inhibit clot-bound thrombin or prothrombinase-bound Xa | Steric limitations of the heparin-AT complex |
LMWH's lower protein binding means it does not suffer from these limitations to the same degree - this underlies its more predictable dose-response.
9. Quick-Reference Comparison Table
| Feature | UFH | LMWH |
|---|---|---|
| Molecular weight | 5,000-30,000 (mean 15,000) | 1,000-10,000 (mean ~5,000) |
| Anti-Xa:Anti-IIa ratio | 1:1 | 2:1 to 4:1 |
| Bioavailability (SC) | ~30% | ~90% |
| Half-life | 30-60 min | ~4 hours |
| Clearance | Extrarenal (dose-dependent) | Renal (linear) |
| Monitoring | aPTT (mandatory) | Not routinely needed |
| Antidote | Protamine (complete) | Protamine (partial) |
| HIT risk | <5% | <1% |
| Osteoporosis risk | Significant (long-term) | Lower |
| Dosing | IV infusion or SC 2-3x/day | SC once or twice daily |
| Outpatient use | No (IV infusion) | Yes |
| Use in renal failure | Safe (extrarenal clearance) | Caution - accumulation |
| Use in pregnancy | Safe (does not cross placenta) | Safe (preferred over UFH) |
10. Clinical Indications
When to prefer UFH:
- Need for rapid reversal (surgery, bleeding) - protamine fully reverses
- Severe renal impairment (CrCl <30 mL/min) - LMWH accumulates
- Cardiac surgery / CPB (LMWH cannot be reliably monitored intraoperatively)
- Hemodynamically unstable PE or massive PE (IV UFH allows tight titration)
- When rapid discontinuation may be needed
When to prefer LMWH:
- Outpatient DVT/PE treatment
- VTE prophylaxis
- Pregnancy (preferred; lower HIT and osteoporosis risk)
- ACS (enoxaparin has strong evidence in NSTE-ACS)
- Bridging therapy in patients on warfarin
- Patients where daily monitoring is not feasible
Sources:
- Braunwald's Heart Disease, 2-Vol Set (Tables 95.3 & 95.4, pp. 1126-1129)
- Katzung's Basic and Clinical Pharmacology, 16th Ed (pp. 959-961)
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Goldman-Cecil Medicine
Recent evidence note: A 2025 systematic review/meta-analysis (PMID 40352202) compared LMWH vs UFH for bridging in mechanical heart valve patients undergoing non-cardiac surgery, finding comparable outcomes - supporting guideline-based individualized selection rather than a universal preference for one over the other in this specific setting.
This is a shared conversation. Sign in to Orris to start your own chat.