antibodies do for myasthenia gravis
Reading File
Finding Sources
Searching PubMed
"myasthenia gravis" AND "antibodies" AND pathophysiology
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a complete, textbook-grounded answer:
Antibodies in Myasthenia Gravis
Myasthenia gravis (MG) is a postsynaptic autoimmune disorder of the neuromuscular junction (NMJ) in which autoantibodies attack key proteins needed for muscle activation. There are three main antibody types, each with distinct mechanisms and clinical profiles.
1. Anti-AChR Antibodies (~80-85% of generalized MG)
These are directed against the α1 subunit of the nicotinic acetylcholine receptor (AChR) on the postsynaptic muscle membrane. They damage the NMJ through three distinct mechanisms:
A. Complement-mediated destruction (most important mechanism overall)
"Binding" antibodies activate the complement cascade, causing lysis of the postsynaptic membrane, destruction of the junctional folds, and direct loss of AChRs. This results in a simplified, flattened postsynaptic region with far fewer receptors available to respond to acetylcholine.
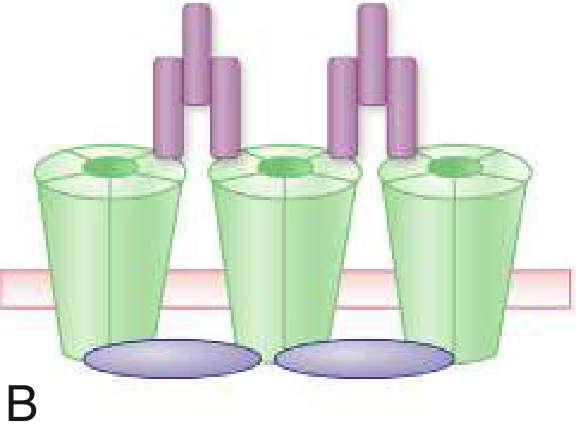
B. Accelerated internalization and degradation ("modulating" antibodies)
Divalent antibodies cross-link adjacent AChR subunits, causing the receptors to be pulled inside the cell (internalized) and degraded at an accelerated rate. This reduces surface receptor density even without immediate structural damage. Modulating antibodies are particularly associated with thymoma-related MG.
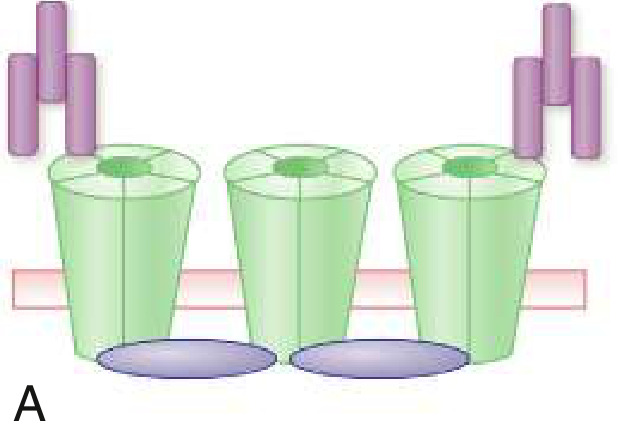
C. Direct blocking of ACh binding ("blocking" antibodies)
Some antibodies bind directly to the ACh-binding site on the AChR α-subunit, physically preventing acetylcholine from attaching and triggering ion channel opening. These occur in fewer than 1% of MG patients without measurable binding antibodies and have limited diagnostic value on their own.
Net result: Reduced number of functional AChRs → reduced amplitude of end-plate potentials → failure to reach action potential threshold → fatigable muscle weakness.
Seropositivity rates:
- Generalized MG: ~85%
- Ocular MG: ~50%
- Thymomatous MG: nearly 100%
2. Anti-MuSK Antibodies (~5-8% of generalized MG)
Directed against muscle-specific tyrosine kinase (MuSK), a receptor on the postsynaptic membrane that works with agrin (released from the nerve terminal) to cluster AChRs during NMJ formation and maintenance.
- Predominantly IgG4 subclass - these do not activate complement effectively; the mechanism is primarily blocking MuSK signaling, which prevents proper AChR clustering and NMJ organization
- Found in up to 50% of generalized MG patients who are seronegative for AChR-abs
- Thymus is normal in appearance (unlike AChR-MG)
- Clinical profile: more prominent facial, bulbar, and neck weakness; greater risk of severe weakness and muscle atrophy; can be confused with motor neuron disease
- Onset typically under 40 years; female predominance
3. Anti-LRP4 Antibodies (~1-3% of all MG)
Directed against lipoprotein receptor-related protein 4 (LRP4), which is the receptor for agrin. Agrin binds LRP4, which then activates MuSK, triggering AChR clustering - so LRP4 antibodies disrupt the same agrin-LRP4-MuSK signaling pathway as MuSK antibodies.
- IgG4 subclass predominantly
- Associated with milder symptoms (mild to moderate weakness)
- Marked female predominance; selective oropharyngeal, facial, and respiratory weakness in some patients
- Age of onset typically 30-50 years
4. Antistriational Muscle Antibodies (Titin and Ryanodine)
These are not the primary pathogenic antibodies but are important clinical markers:
- Anti-titin and anti-ryanodine receptor antibodies are found in thymoma-associated MG and are associated with severe disease
- Patients with thymoma often have both AChR antibodies AND these antistriational antibodies
- They react with contractile elements of skeletal muscle
5. "Seronegative" MG
About 10-15% of generalized MG patients test negative for all three main antibodies. Many of these patients have:
- Low-affinity AChR antibodies detectable only by cell-based assays (not routine RIA)
- Antibodies against agrin or cortactin
- Their response to immunotherapy is similar to AChR-positive MG, implying an antibody-driven mechanism still exists
Summary Table
| Antibody | Target | Mechanism | Frequency | Clinical Feature |
|---|---|---|---|---|
| Anti-AChR | AChR α1 subunit | Complement lysis, internalization, direct block | 80-85% (gen.) | Classic MG pattern |
| Anti-MuSK | MuSK | Blocks AChR clustering (IgG4, no complement) | 5-8% | Bulbar/facial predominant |
| Anti-LRP4 | LRP4 | Blocks agrin-LRP4-MuSK axis | 1-3% | Mild-moderate disease |
| Anti-titin/ryanodine | Muscle contractile proteins | Marker (not primary pathogen) | Thymoma-MG | Severe/thymoma-associated |
Sources: Bradley and Daroff's Neurology in Clinical Practice, pp. 2772-2775 | Robbins & Kumar Basic Pathology, p. 809 | Goldman-Cecil Medicine, Figure 3.9-2 | Harrison's Principles of Internal Medicine 22e
This is a shared conversation. Sign in to Orris to start your own chat.