


Find the abnormality
shoulder X-ray anterior dislocation glenohumeral
glenohumeral dislocation X-ray findings Hill-Sachs Bankart
Findings: Anterior Glenohumeral Dislocation
Key Abnormality: Anterior Subcoracoid Dislocation of the Glenohumeral Joint
| Finding | Description |
|---|---|
| Humeral head position | Displaced inferiorly and medially, lying beneath the coracoid process — classic subcoracoid anterior dislocation |
| Loss of joint congruity | The humeral head is no longer seated in the glenoid fossa; the normal "ball-in-socket" relationship is lost |
| Empty glenoid sign | The glenoid fossa appears vacant on the AP view |
| Humerus axis | The shaft of the humerus is typically abducted and externally rotated |
Associated Injuries to Assess
- Hill-Sachs lesion — posterolateral humeral head compression fracture (impaction against the glenoid rim); look for a vertical dense line/notch on the superolateral humeral head
- Bony Bankart lesion — fracture of the anteroinferior glenoid rim
- Greater tuberosity fracture — occurs in ~15–35% of anterior dislocations, especially in older patients (this patient is 57 — higher risk)
Per Bailey & Love's Surgery, 28th Ed. (p. 522): West Point axillary and Stryker notch views are specifically helpful for evaluating Bankart fractures and Hill-Sachs lesions respectively. CT ± 3D reconstruction is recommended when glenoid bone loss is suspected; MRI for soft-tissue injuries (rotator cuff tear, HAGL, labral pathology).
Clinical Priorities
- Closed reduction (Cunningham, Milch, or FARES technique) after adequate analgesia/sedation
- Post-reduction X-ray to confirm relocation and rule out iatrogenic fracture
- Neurovascular check — axillary nerve injury is the most common nerve complication (test deltoid sensation and strength)
- Imaging post-reduction — MRI shoulder to assess rotator cuff (cuff tears are common in patients >40 years with first-time dislocation)
Find abnormalities
Systematic Radiological Analysis — Right Shoulder AP Views
1. 🔴 PRIMARY ABNORMALITY: Anterior Glenohumeral Dislocation
- The humeral head is displaced anteromedially, lying beneath the coracoid process (subcoracoid type — most common, ~65% of all shoulder dislocations)
- The glenoid fossa is empty — no ball-in-socket relationship visible
- The humeral shaft is abducted and externally rotated
- The finger points precisely to the inferiorly and medially displaced humeral head
2. 🔴 CRITICAL ADDITIONAL FINDING: Pseudo-widening / Soft Tissue Opacity at Humeral Neck
Probable fracture-dislocation — the humeral head appears somewhat separated from the shaft, raising concern for a 2-part surgical neck fracture with anterior dislocation
3. 🟡 Hill-Sachs Lesion (Likely)
- A posterolateral humeral head compression defect is suggested by the contour irregularity of the humeral head — the classic impaction fracture from the humeral head striking the anterior glenoid rim during dislocation
- Confirmed only on Stryker notch or axillary lateral view
4. 🟡 Greater Tuberosity — Assess Carefully
- In a 57-year-old, greater tuberosity avulsion fracture occurs in up to 30–40% of anterior dislocations
- The greater tuberosity contour appears mildly irregular on the first image — cannot be fully excluded on AP alone
- May only become apparent post-reduction
5. 🟡 Acromioclavicular (AC) Joint
- The AC joint appears intact with no obvious step deformity or widening
6. 🟡 Visible Chest / Lung Field
- Partially visible right lung field shows no obvious pneumothorax or hemothorax in the visible portions
- Full chest X-ray should be performed if high-energy trauma
Summary Table
| Structure | Finding | Significance |
|---|---|---|
| Glenohumeral joint | Anterior (subcoracoid) dislocation | PRIMARY diagnosis |
| Humeral surgical neck | Possible fracture-dislocation | Neer 2-part — changes management |
| Humeral head posterolateral | Probable Hill-Sachs lesion | Instability risk |
| Greater tuberosity | Contour irregularity — possible avulsion | Check post-reduction |
| Axillary nerve | Not visible on X-ray | Clinically examine — most common nerve injury |
| AC joint | Intact | No additional injury |
Management Implications
- If isolated dislocation → Closed reduction under sedation + post-reduction X-ray
- If fracture-dislocation → Do NOT attempt blind closed reduction — risk of displacing fracture fragments; requires orthopedic surgeon, possible open reduction
- Axillary view / CT scan urgently recommended before reduction to characterize the fracture pattern
- Post-reduction: MRI to assess rotator cuff (very high rate of cuff tears in patients >40 years)
mark the dislocated part on c ray
A medical X-ray annotation diagram of a right shoulder AP view showing anterior glenohumeral dislocation. The image should look like a real X-ray with a bright white circle or arrow clearly marking and labeling the dislocated humeral head that is displaced inferiorly and medially below the coracoid process, away from the empty glenoid fossa. Include clear annotation labels: "Dislocated Humeral Head" with a red arrow pointing to it, "Empty Glenoid Fossa" labeled, and "Coracoid Process" labeled. Style: medical radiology educational annotation on dark X-ray background with white bone structures.
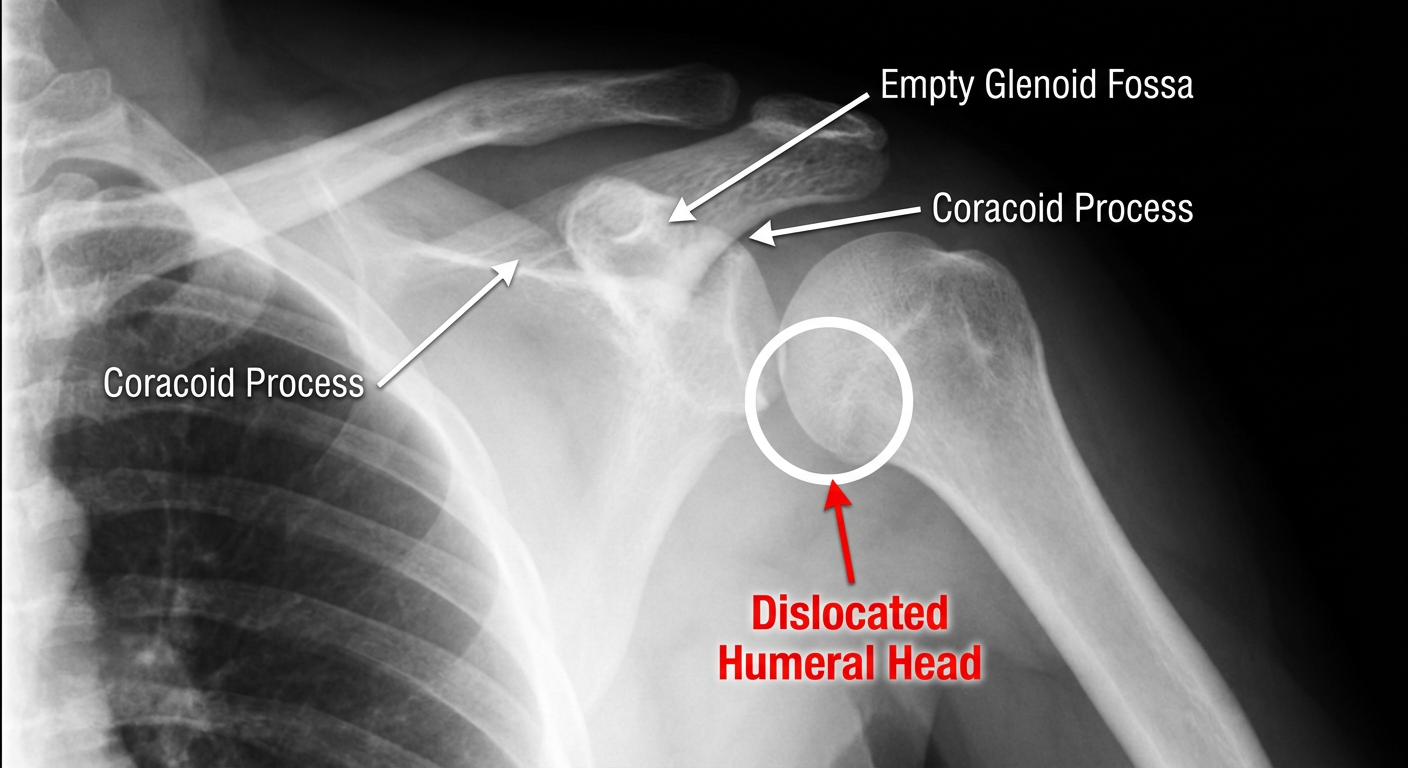
| Label | Location on X-ray |
|---|---|
| 🔴 Dislocated Humeral Head | The large round opacity sitting below and medial to where it should be — beneath the coracoid, where the finger is pointing |
| ⬜ Empty Glenoid Fossa | The socket area that appears vacant — no humeral head sitting in it |
| 🟡 Normal position | Humeral head should sit squarely against the glenoid, forming a smooth joint space |
Note: I cannot directly draw on your uploaded X-ray images, but the reference diagram above illustrates exactly where to look on your films.