Contractility of cardiac muscle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full response.
Contractility of Cardiac Muscle
Definition
Contractility (also called inotropy) is the intrinsic ability of the myocardium to generate force and shorten, independent of preload (EDV) and afterload (arterial resistance). It provides a way to distinguish a better-performing heart from a poorly performing one without changing ventricular filling or outflow conditions.
- Medical Physiology (Boron & Boulpaep), p. 771
Molecular Basis: Excitation-Contraction Coupling
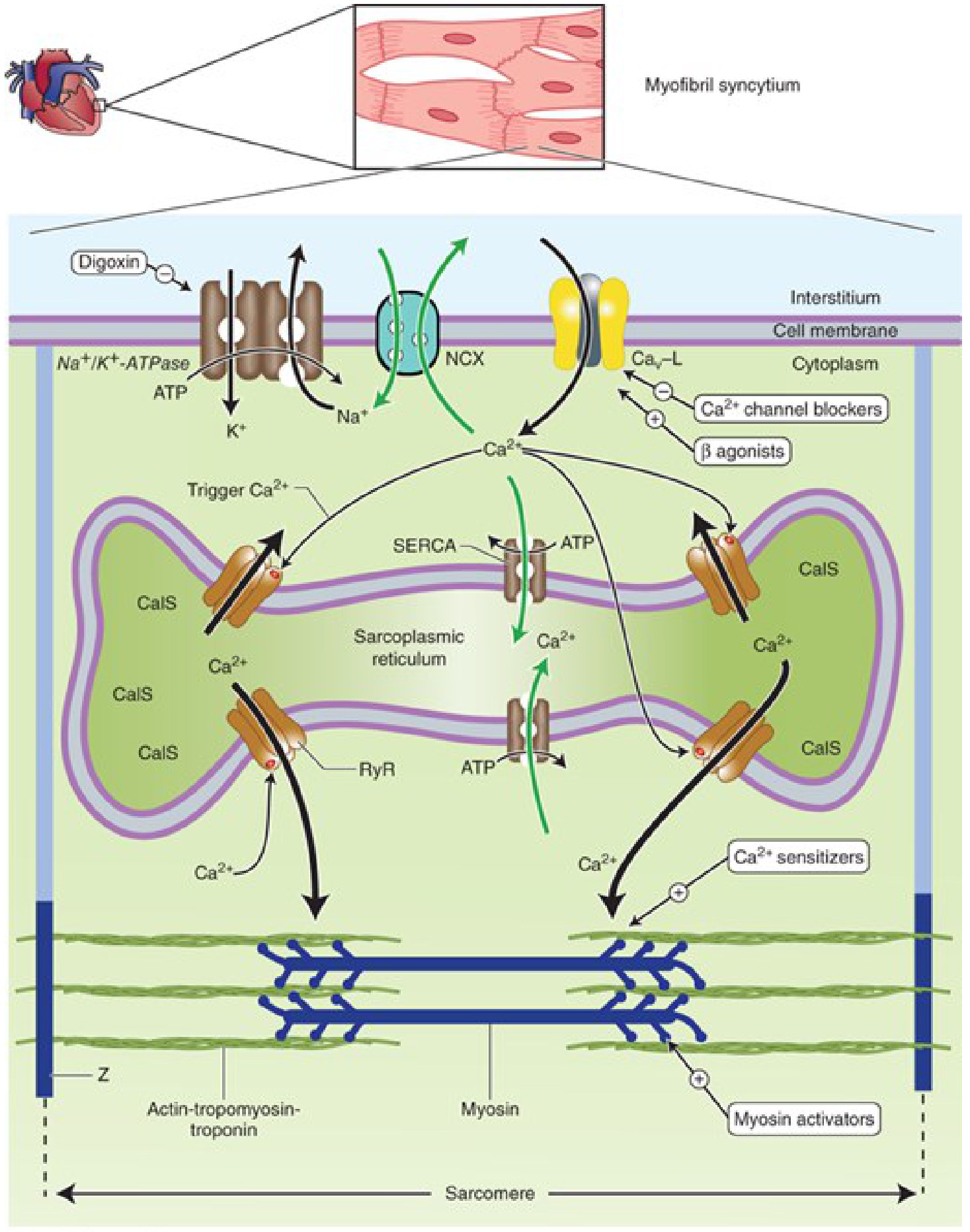
The cellular mechanism linking membrane depolarization to force generation is calcium-mediated excitation-contraction coupling:
- Action potential spreads along the sarcolemma and into T-tubules (which are 5x wider in cardiac vs. skeletal muscle, providing a large Ca²+ reservoir).
- L-type (Ca_v-L) voltage-gated calcium channels in the T-tubule membrane open, allowing a small "trigger Ca²+" influx.
- Trigger Ca²+ activates RyR2 (ryanodine receptor 2) channels on the sarcoplasmic reticulum (SR) membrane - this is calcium-induced calcium release (CICR).
- A large surge of Ca²+ floods the cytoplasm from SR stores (calsequestrin-bound Ca²+).
- Cytoplasmic Ca²+ binds troponin C, displacing tropomyosin and exposing actin active sites.
- Actin-myosin cross-bridge cycling begins, producing shortening and force.
Unlike skeletal muscle, cardiac muscle is critically dependent on extracellular Ca²+ - a calcium-free solution stops the heart quickly because cardiac SR stores are less developed.
- Guyton & Hall Textbook of Medical Physiology, p. 125
- Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 332
Determinants of Contractility
Katzung's identifies five key determinants:
| Factor | Effect on contractility |
|---|---|
| A. Ca²+ sensitivity of contractile proteins | Troponin C affinity for Ca²+; altered by drugs like levosimendan |
| B. Ca²+ released from SR | Proportional to SR Ca²+ store and RyR2 response to trigger Ca²+ |
| C. Ca²+ stored in SR | Governed by SERCA pump activity (inhibited by phospholamban; phospholamban inactivated by PKA) |
| D. Trigger Ca²+ entering cell | Depends on extracellular [Ca²+], L-channel availability, and their open duration |
| E. NCX activity and intracellular [Na+] | NCX extrudes 1 Ca²+ using 3 Na+ gradient; intracellular [Na+] is the key variable |
- Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 332-333
Relaxation (Lusitropy)
Contraction ends when Ca²+ is removed from the cytoplasm:
- SERCA pumps ~70% of Ca²+ back into the SR (inhibited basally by phospholamban; activated by beta-receptor stimulation via PKA)
- NCX extrudes ~30% Ca²+ out of the cell
- Phospholamban phosphorylation by PKA not only boosts SERCA but also speeds relaxation (positive lusitropic effect of sympathetic stimulation)
Regulation of Contractility
Positive Inotropes (increase contractility)
| Agent | Mechanism |
|---|---|
| Catecholamines (NE, Epi, dobutamine) | β1-receptor → Gs → adenylyl cyclase → ↑cAMP → PKA activation → phosphorylates L-channels (↑Ca²+ entry), phospholamban (↑SERCA, ↑SR Ca²+ load), troponin I (faster relaxation) |
| Cardiac glycosides (digoxin) | Inhibit Na+/K+-ATPase → ↑intracellular Na+ → reduces NCX driving force → ↑intracellular Ca²+ → ↑SR Ca²+ loading |
| PDE inhibitors (milrinone, enoximone) | Prevent cAMP degradation → same downstream effects as β-agonists |
| Ca²+ sensitizers (levosimendan) | Increase affinity of troponin C for Ca²+; may also inhibit PDE |
| Myosin activators (omecamtiv mecarbil) | Shift myosin from weak to strong actin-binding state; increase efficiency |
| Xanthines (caffeine, theophylline) | Inhibit cAMP breakdown → positively inotropic |
Negative Inotropes (decrease contractility)
| Agent | Mechanism |
|---|---|
| Calcium channel blockers | Block L-type channels → ↓trigger Ca²+ → ↓SR release |
| Vagal stimulation / ACh | M2 receptors → ↓cAMP → negative inotropic (especially atria) |
| Beta-blockers | Block β1-receptor → ↓cAMP signaling |
| Ryanodine | Plant alkaloid that blocks RyR2 channels - potent negative inotrope |
- Ganong's Review of Medical Physiology, 26th Ed., p. 546-547
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 677
Force-Frequency Relationship (Bowditch Effect)
Contractility also increases as heart rate increases - this is the Treppe (staircase) phenomenon or Bowditch effect. At higher rates, cumulative Ca²+ influx per unit time increases SR Ca²+ loading, resulting in larger releases and stronger contractions. Ventricular extrasystoles similarly cause postextrasystolic potentiation - the beat after an extrasystole is stronger due to increased intracellular Ca²+ availability, independent of ventricular filling.
- Ganong's Review of Medical Physiology, 26th Ed., p. 547
Clinical Assessment of Contractility
Contractility is difficult to measure in isolation because most clinical parameters also reflect preload or afterload. Several indexes are used:
- Ejection fraction (EF) - most common clinically (normal >60%); influenced by preload, so imperfect
- dP/dt (rate of pressure rise) - rate of LV pressure development during isovolumetric contraction; correlates with velocity of shortening; sensitive to inotropic interventions
- Velocity of ejection - similarly load-sensitive but useful
- End-Systolic Pressure-Volume Relationship (ESPVR) - the slope of the line connecting end-systolic pressure-volume points at varying preloads is a load-independent index of contractility. A steeper ESPVR slope = greater contractility. This is the most physiologically rigorous measure.
- Medical Physiology (Boron & Boulpaep), p. 771-774
Key Summary
- Contractility = intrinsic myocardial performance, independent of preload and afterload
- The central trigger is intracellular Ca²+ - anything that raises peak systolic [Ca²+] or sensitizes myofilaments to Ca²+ increases contractility
- The β1-adrenergic / cAMP / PKA pathway is the dominant physiological positive inotropic mechanism
- Digoxin works indirectly via Na+/K+-ATPase inhibition → ↑Na+ → ↓NCX → ↑Ca²+
- Clinical measurement is approximated by EF, dP/dt, and most accurately by the ESPVR slope
This is a shared conversation. Sign in to Orris to start your own chat.