Troponins in acute coronary syndrome
Reading File
search_medical_text
troponin biomarker acute coronary syndrome diagnosis
search_medical_text
high-sensitivity troponin assay NSTEMI STEMI serial testing
GradeResponse
GradeResponse
search_medical_image
troponin rise and fall kinetics ACS myocardial infarction
search_medical_text
troponin elevation causes non-ischemic cardiac injury false positive
GradeResponse
Troponins in Acute Coronary Syndrome (ACS)
What Are Cardiac Troponins?
Troponins are regulatory proteins of the actin-myosin contractile apparatus. Three isoforms exist: troponin I (cTnI), troponin T (cTnT), and troponin C. Only cTnI and cTnT have cardiac-specific isoforms, making them the preferred biomarkers for myocardial injury. They are released into the bloodstream when cardiomyocyte membrane integrity is disrupted.
Role in ACS Diagnosis
Troponins — alongside ECG and clinical presentation — form the diagnostic triad for ACS. They are the preferred biomarkers for detecting myocardial necrosis (Bailey & Love's, p. 969):
| ACS Subtype | Troponin Finding |
|---|---|
| STEMI | Elevated (diagnosis primarily ECG-based; troponins confirm necrosis) |
| NSTEMI | Elevated above 99th percentile URL with a rising/falling pattern |
| Unstable Angina | Normal (no myocardial necrosis) |
Troponin Kinetics in Acute MI
The rise-and-fall pattern is the hallmark of acute, ischemic myocardial injury and distinguishes it from chronic myocardial injury (where levels are persistently, stably elevated above the 99th percentile):
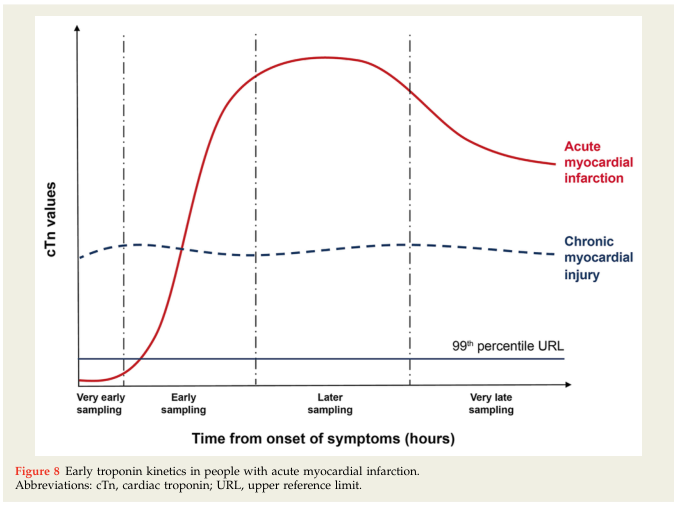
Typical timeline for conventional troponin:
- Detectable: ~3–6 hours after symptom onset
- Peaks: ~12–24 hours
- Normalizes: 5–14 days (cTnI faster; cTnT may persist longer)
High-Sensitivity Troponin (hs-cTn) Assays
hs-cTn assays have transformed ACS workup by detecting troponin elevations earlier and at lower concentrations. The ESC guidelines recommend the 0h/1h or 0h/2h algorithm for rapid rule-out and rule-in of NSTEMI (Management of ACS, p. 22):
Three pathways based on hs-cTn results at 0h and 1h/2h:
| Pathway | Criteria | Action |
|---|---|---|
| Rule-Out | Very low 0h value, OR low 0h + no significant 1h/2h delta | Discharge / low-risk pathway |
| Rule-In | High 0h value, OR large 1h/2h delta | NSTEMI confirmed → invasive strategy |
| Observe | Neither rule-out nor rule-in criteria met | Repeat hs-cTn at 3h ± echo |
Key point: Cut-offs are assay-specific and must meet pre-defined sensitivity/specificity thresholds. The 0h/1h algorithm is only applicable if chest pain onset was >3 hours prior to initial measurement.
The 99th Percentile Upper Reference Limit (URL)
- Definition: The 99th percentile of hs-cTn in a healthy reference population — this is the diagnostic threshold for myocardial injury.
- Elevation above the URL + a rising/falling pattern = acute myocardial injury.
- Values above URL without dynamic change = chronic myocardial injury (e.g., heart failure, CKD, LVH).
Causes of Troponin Elevation (Beyond ACS)
Troponin elevation is a marker of myocardial injury, not necessarily ischemia. Other causes include:
Cardiac (non-ACS):
- Myocarditis, pericarditis
- Heart failure (acute decompensation)
- Hypertensive emergency
- Takotsubo cardiomyopathy
- Arrhythmias (e.g., SVT, AF with rapid ventricular rate)
- Cardiac contusion
- Post-cardioversion
Non-Cardiac:
- Pulmonary embolism
- Sepsis / critical illness
- Stroke, subarachnoid haemorrhage
- Renal failure (reduced clearance)
- Rhabdomyolysis
- Burns, chemotherapy toxicity
Practical Clinical Points
- Serial testing is mandatory — a single value is insufficient; the kinetic pattern (rising/falling) is what defines acute MI.
- Clinical context is essential — elevated troponin + chest pain + ECG changes = ACS until proven otherwise; elevated troponin alone in a septic patient likely reflects demand ischemia or direct injury.
- hs-cTn detects smaller infarcts and elevates earlier, improving sensitivity but reducing specificity — this makes context and delta changes more important.
- cTnI vs. cTnT: Both are cardiac-specific. cTnT may remain elevated longer (useful for late presentations); cTnI may clear faster. Assays are not interchangeable.
- Gender differences: Women have lower baseline hs-cTnI levels; some guidelines recommend sex-specific cut-offs.
Other Cardiac Biomarkers (Comparison)
| Biomarker | Rise | Peak | Normalization | Advantage |
|---|---|---|---|---|
| hs-cTnI/T | 1–3 h | 12–24 h | 5–14 days | Earliest, most sensitive/specific |
| CK-MB | 3–6 h | 12–24 h | 48–72 h | Useful for re-infarction detection |
| Myoglobin | 1–3 h | 6–9 h | 24 h | Early marker, not cardiac-specific |
| BNP/NT-proBNP | Hours | Variable | Variable | Risk stratification, heart failure |
Troponins remain the cornerstone biomarker in ACS. The shift to hs-cTn assays and the ESC 0h/1h/2h algorithms has enabled faster, more accurate triage — but clinical judgment integrating symptoms, ECG, and serial values remains indispensable.
This is a shared conversation. Sign in to Orris to start your own chat.