Advanced neonatal resuscitation
Reading File
Finding Sources
Searching PubMed
"neonatal resuscitation" advanced
Reading File
Reading File
Reading File
Reading Article
PMID: 41122887
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
I now have rich, comprehensive content from multiple authoritative textbooks plus the 2025 AHA/AAP guideline update. Let me compile the full response.
Advanced Neonatal Resuscitation
Overview
Approximately 10% of newborns require some form of resuscitative assistance at birth; fewer than 1% require advanced measures such as chest compressions or medications. Because the most common cause of neonatal depression is intrauterine asphyxia, the entire emphasis is on restoring ventilation and oxygenation first. The 2025 AHA/AAP Neonatal Resuscitation Guidelines (PMID 41122887) now incorporate deferred cord clamping, updated oxygen titration targets, and a refined chain of care from prenatal counseling to post-resuscitation follow-up.
The Neonatal Resuscitation Algorithm
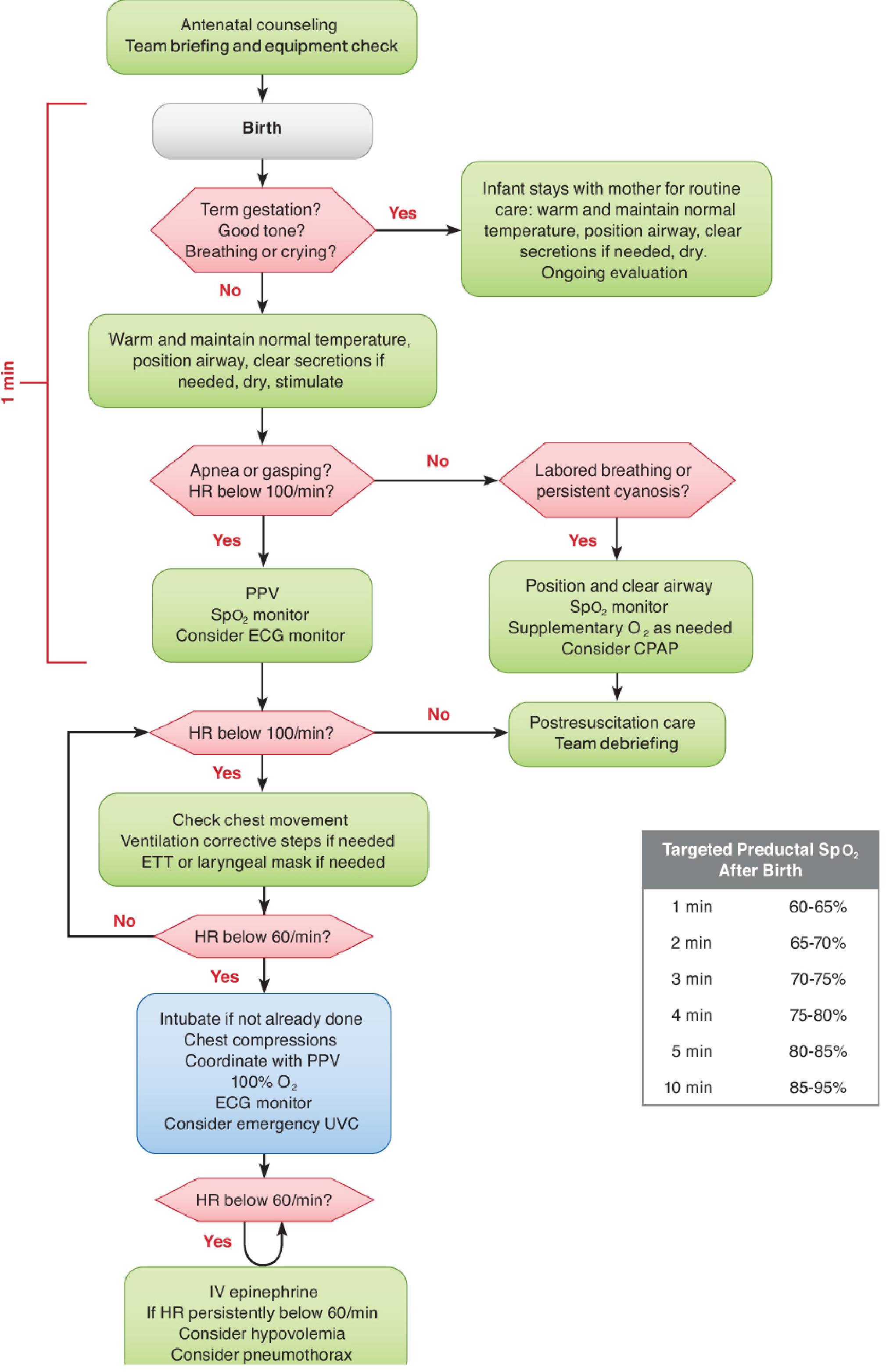
AHA Neonatal Resuscitation Algorithm - Barash Clinical Anesthesia, 9e
Step 0 - Rapid Initial Assessment (First 30 seconds - the "Golden Minute")
Three questions determine if the infant can stay with the mother:
- Term gestation?
- Good muscle tone?
- Breathing or crying?
If all three = Yes: routine care (warm, dry, position, monitor). If any = No: move to radiant warmer and begin the resuscitation sequence.
Ongoing assessment uses three parameters: heart rate (HR), respirations, and SpO2 - all within the first 30 seconds. Three-lead ECG is more accurate for HR than pulse oximetry or umbilical pulse palpation, which both tend to underestimate the true HR. - Rosen's Emergency Medicine, 10e
Pre-Resuscitation Preparation
Equipment checklist (Box 159.2, Rosen's EM):
- Radiant warmer, warm blankets, polyethylene wrap (for premature infants)
- Suction: bulb syringe + mechanical suction catheters (5, 8, 10 Fr); wall suction set to <100 mmHg
- BVM: self-inflating 450/750 mL or flow-inflating 250/450 mL with premature/newborn/infant masks
- Laryngoscope with straight Miller blades (00, 0, 1)
- ETTs (2.5, 3.0, 3.5, 4.0 mm), uncuffed with stylets
- Pediatric CO2 detector / colorimetric capnography
- Umbilical catheters (3.5 and 5 Fr) + catheterization supplies
- Meconium aspirator
ETT Size by Weight/Gestational Age:
| Birth Weight | Gestational Age | ETT Size |
|---|---|---|
| <1 kg | <28 weeks | 2.5 mm |
| 1-2 kg | 28-34 weeks | 3.0 mm |
| 2-3 kg | 34-38 weeks | 3.5 mm |
| >3 kg | >38 weeks | 3.5-4.0 mm |
Maternal history to obtain:
- Gestational age, multiple gestation?
- Meconium present?
- Maternal fever or infections?
- Medications or drugs taken?
- Prenatal care / prenatal ultrasound abnormalities?
Step 1 - Warming and Initial Stabilization
- Place under radiant warmer; dry and stimulate (rub back, flick soles of feet)
- Goal temperature: normothermia; axillary target 36.5°C
- Polyethylene wrap (from neck down) or warm blankets prevent evaporative heat loss. Beanies reduce head heat loss
- Hypothermia is an independent risk factor for neonatal mortality worldwide; hyperthermia causes neonatal encephalopathy
- Controlled therapeutic hypothermia is only appropriate in tertiary centers for infants with hypoxic-ischemic encephalopathy (HIE), initiated within hours of birth - never in the delivery room as a default
Airway - sniffing position:
- Avoid both under-extension and hyperextension (both obstruct)
- A 1-inch towel roll under the shoulders helps maintain proper positioning
- Deep/routine suctioning is not recommended - it causes vagal bradycardia and reduces cerebral blood flow. Suction only if obvious airway obstruction exists, or if a non-vigorous infant has meconium
Step 2 - Positive Pressure Ventilation (PPV)
Indications:
- Apnea or gasping respirations
- HR < 100 beats/min
- Persistent central cyanosis despite free-flow O2
Rate: 30-60 breaths/min ("breathe - two - three, breathe - two - three...")
Initial pressure: Up to 40 cmH2O may be needed for the first breath; thereafter keep ≤30 cmH2O
Assessment: Auscultation + visible chest rise
Oxygen Targets - Key 2020/2025 NRP Change
| Population | Initial FiO2 | Escalation |
|---|---|---|
| Term (≥35 weeks) | 21% (room air) | Titrate to SpO2 targets |
| Preterm (<35 weeks) | 21-30% | Titrate to SpO2 targets |
| If HR <60/min or chest compressions needed | 100% | After HR recovers, wean |
Preductal SpO2 targets (right hand probe):
| Time after birth | Target SpO2 |
|---|---|
| 1 min | 60-65% |
| 2 min | 65-70% |
| 3 min | 70-75% |
| 4 min | 75-80% |
| 5 min | 80-85% |
| 10 min | 85-95% |
Restoring ventilation is almost always more beneficial than simply increasing FiO2. - Miller's Anesthesia, 10e
Step 3 - Endotracheal Intubation
Indications:
- Tracheal suctioning for meconium in non-vigorous infants
- BMV ineffective or prolonged
- Chest compressions are being performed
- Extremely low birth weight infants
- Anatomic anomalies (diaphragmatic hernia, tracheoesophageal fistula)
Technique: Miller 00, 0, or 1 blade. Both traditional direct laryngoscopy and video laryngoscopy are acceptable; video-assisted techniques provide better views but slightly longer intubation times. - Rosen's EM, 10e
Confirmation of placement: Colorimetric CO2 detector / capnography (gold standard for acute confirmation). Plain chest X-ray remains the standard for definitive position. Ultrasound can assess ETT position in term infants.
LMA: Effective for ventilating full-term newborns when ETT intubation is technically difficult. Limited data in preterm infants (<2000 g or <34 weeks), meconium aspiration syndrome, or during active CPR.
If the Intubated Infant Deteriorates - DOPE + MR SOPA
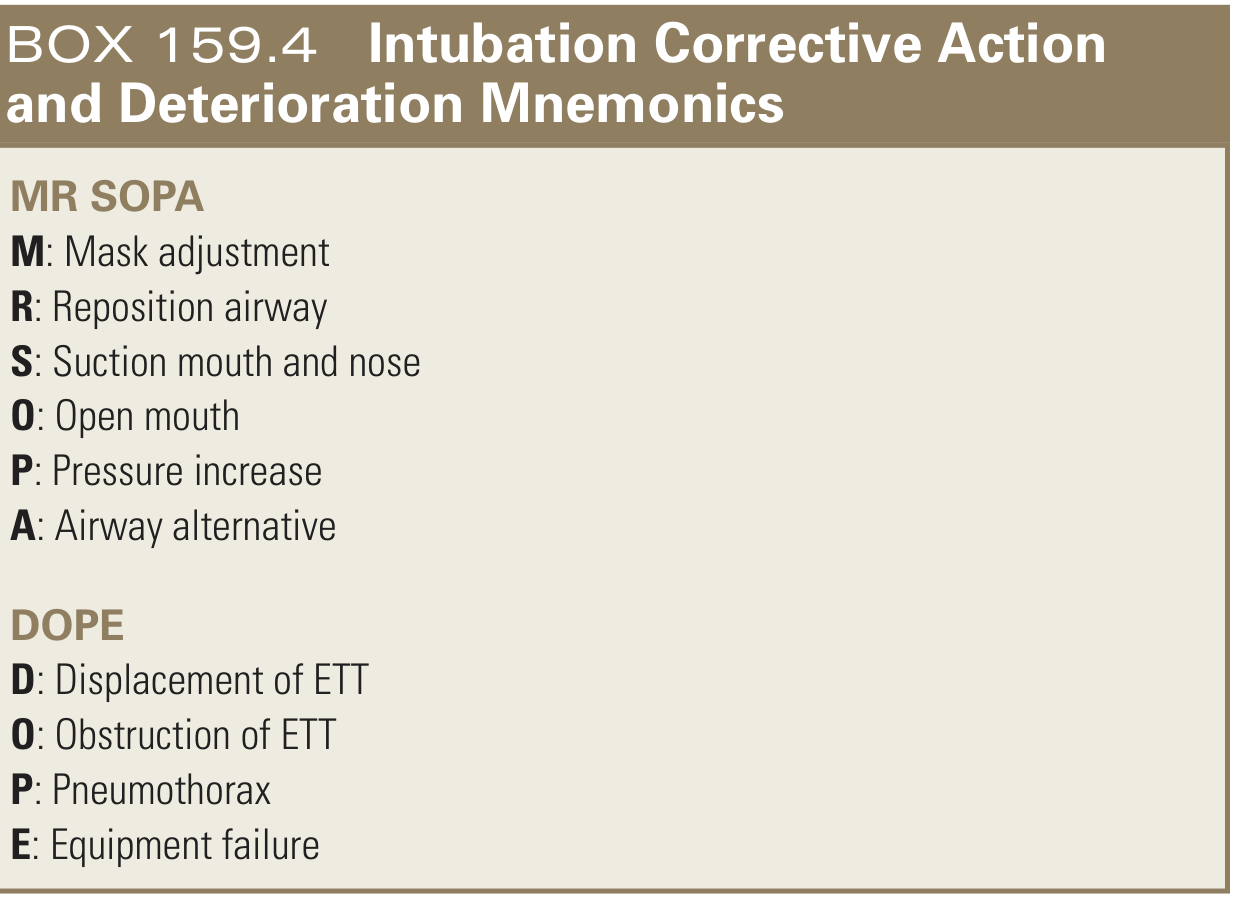
- DOPE = Displacement of ETT, Obstruction, Pneumothorax, Equipment failure
- MR SOPA = Mask adjustment, Reposition airway, Suction, Open mouth, Pressure increase, Airway alternative
If no obvious cause: extubate and ventilate with BMV while you reassess. Consider needle thoracentesis if pneumothorax suspected (unequal breath sounds, high ventilatory pressures, failure to improve).
Step 4 - Chest Compressions
Threshold: HR < 60 beats/min despite adequate ventilation (good chest rise) with oxygen for at least 30 seconds.
Technique - Two Thumbs-Encircling Hands (preferred):
- Both hands encircle the chest, fingers support the back
- Thumbs placed side-by-side (or one over the other) just below the nipple line on the sternum
- This method generates higher peak systolic pressure and is preferred when two providers are present
- Depth = one-third of the anteroposterior chest diameter
Rate and ratio:
- 90 compressions/min + 30 breaths/min = 120 events/min
- Compression:ventilation ratio = 3:1 (neonates - asphyxia-first physiology)
- If primary cardiac cause is certain: 15:2 ratio may be considered
Assessment: Every 30 seconds. A color change to yellow on the colorimetric CO2 monitor or rise in ETCO2 often precedes HR recovery - use it when available. Continue until HR ≥60 beats/min.
Step 5 - Vascular Access
Umbilical Vein Catheter (UVC) - first choice:
- Easiest, fastest access in the delivery room
- Insert 3.5 Fr (for <3.5 kg) or 5 Fr catheter to approximately 5 cm - until blood return is obtained
- Remove once infant is stabilized and alternative access is secured (risk: portal vein thrombosis, infection)
Intraosseous (IO):
- Faster to place than UVC in simulated resuscitations (~1 min faster even for skilled providers)
- Preferred sites: distal femur (midline, ~1 cm above superior border of patella) or proximal tibia (~2 cm below tuberosity)
- Caution in premature infants due to bone fragility and small IO space
Endotracheal route: Can be used for epinephrine when IV/IO access is unavailable, but is less reliable and requires higher doses.
Step 6 - Medications
Epinephrine
- Indication: Asystole or persistent HR < 60 beats/min despite effective ventilation + ongoing chest compressions
- IV/IO dose: 0.01-0.03 mg/kg (0.1-0.3 mL/kg of 0.1 mg/mL solution) - IV is the preferred route
- ETT dose (if no IV access): 0.05-0.1 mg/kg - higher dose required; efficacy is less certain
- Repeat: Every 3-5 minutes
- Unlike adult resuscitation, there is no minimum dose - strict weight-based dosing applies
Volume Expansion
- When: Suspected hypovolemia - pallor, weak pulse, failure to respond to other measures; maternal/fetal hemorrhage, placental transection, early cord clamping
- Fluid: Normal saline, Lactated Ringer's, or O-negative packed RBCs
- Dose: 10 mL/kg IV over 5-10 minutes; may repeat as needed
- Full-term infants: higher boluses (20 mL/kg) can be used
- Premature infants: avoid rapid volume expansion - increases risk of intraventricular hemorrhage (IVH)
Glucose (D10W)
- Concomitant hypoglycemia is common in depressed neonates
- Treat glucose <40 mg/dL with symptoms: 2-4 mL/kg D10W IV, then continuous infusion at 80-100 mL/kg/day
- Avoid higher concentrations (D25W, D50W) - risk of cerebral osmotic injury
Sodium Bicarbonate
- Not routinely recommended in acute neonatal resuscitation
- May be considered in NICU when ventilation is known to be adequate and metabolic acidosis is documented
Antibiotics (post-resuscitation)
- Not indicated during acute resuscitation phase
- If sepsis suspected after stabilization: ampicillin (100 mg/kg IV) + gentamicin (4 mg/kg)
- Cefotaxime preferred over ceftriaxone (ceftriaxone raises risk of kernicterus)
Special Situations
Meconium-Stained Amniotic Fluid (MSAF)
- Most meconium aspiration occurs in utero, so routine intubation + suctioning is no longer recommended for all MSAF infants
- Vigorous infants with MSAF: No routine tracheal suctioning; provide routine care
- Non-vigorous infants with MSAF (poor tone, poor respiratory effort, HR <100 after 1 minute of PPV): consider laryngoscopy + ETT suctioning via meconium aspirator attachment
- Overly vigorous oropharyngeal suctioning itself causes bradycardia - be judicious
Premature Infants (<35 Weeks)
- Depressed neonates are predominantly very low birth weight (<1500 g)
- Requires 2+ providers (airway + compressions) + a third for IV access/medications
- Polyethylene bag/wrap from neck down is particularly important - they lose heat rapidly
- Initial FiO2: 21-30%, titrate carefully to avoid hyperoxia (associated with IVH, retinopathy)
- Avoid rapid volume infusion (IVH risk)
- Lower IO bone threshold: bone fragility limits IO placement
Congenital Anomalies to Consider When Resuscitation Fails
- Pneumothorax (1% incidence) - unequal breath sounds, high peak pressures
- Tracheoesophageal fistula (1:3,000-5,000 births)
- Congenital diaphragmatic hernia (1:2,000-4,000 births)
- Choanal atresia, laryngeal webs
Cord Clamping (2025 AHA Update)
- Deferred cord clamping for at least 60 seconds is now recommended for most newborns proceeding to normal transition
- Benefits: increased blood volume, reduced IVH in preterms, improved hematologic outcomes
Discontinuing Resuscitation
- If no signs of life (no HR) after 10 minutes of complete and adequate resuscitative efforts, it is appropriate to consider discontinuing
- Factors favoring continuation: potentially reversible cause (e.g., hypothermia), uncertain gestational age
- Survival with good outcome becomes increasingly unlikely after 10 minutes of asystole; this is a shared decision with the team and family
Apgar Score at a Glance
| Score | 0 | 1 | 2 |
|---|---|---|---|
| Appearance (color) | Blue/pale | Blue extremities | Pink |
| Pulse | Absent | <100 | ≥100 |
| Grimace | None | Grimace | Cry |
| Activity (tone) | Limp | Some flexion | Active |
| Respirations | Absent | Slow/irregular | Good/crying |
Practical resuscitation guidance by 1-min Apgar:
- 5-7: Stimulation + blow-by O2 (mildly asphyxiated)
- 3-4: Temporary bag-mask PPV (moderate depression)
- 0-2: Immediate intubation + possible chest compressions (severe depression)
Post-Resuscitation Care
- Transfer to NICU with continuous monitoring (HR, SpO2, glucose, temperature)
- Avoid hyperthermia
- Therapeutic hypothermia for HIE: 33.5-34.5°C for 72 hours, in tertiary centers only, initiated within 6 hours of birth
- Team debriefing after every resuscitation event
2025 AHA/AAP Key Updates (PMID 41122887)
- Deferred cord clamping ≥60 seconds for most newborns
- Skin-to-skin contact prioritized for all stable infants
- Room air (21%) for term infants; 21-30% for preterm
- 100% O2 only when HR <60 or compressions are in progress
- Chest compression threshold re-examined - 2025 systematic review (PMID 40360699) questions the precise HR cutoff for initiating compressions, noting evidence gaps for the 60 bpm threshold
Sources: Rosen's Emergency Medicine (10e) | Miller's Anesthesia (10e) | Morgan & Mikhail's Clinical Anesthesiology (7e) | Barash Clinical Anesthesia (9e) | AHA/AAP 2025 Guidelines (PMID 41122887)
This is a shared conversation. Sign in to Orris to start your own chat.