Difficult airway algorithm
difficult airway algorithm ASA flowchart
Difficult Airway Algorithm
Definition
Step 1 — Pre-procedure Assessment
| Problem | Assessment Tools |
|---|---|
| Difficult mask ventilation | MOANS mnemonic |
| Difficult supraglottic airway placement | RODS mnemonic |
| Difficult laryngoscopy / intubation | LEMON, SMART assessment |
| Difficult surgical airway access | SHORT mnemonic |
| Patient cooperation / consent | Clinical judgment |
- Awake intubation vs. intubation after induction of general anesthesia
- Non-invasive vs. invasive initial approach
- Video-assisted laryngoscopy as the initial approach
- Preservation vs. ablation of spontaneous ventilation
ASA Difficult Airway Algorithm (2022)
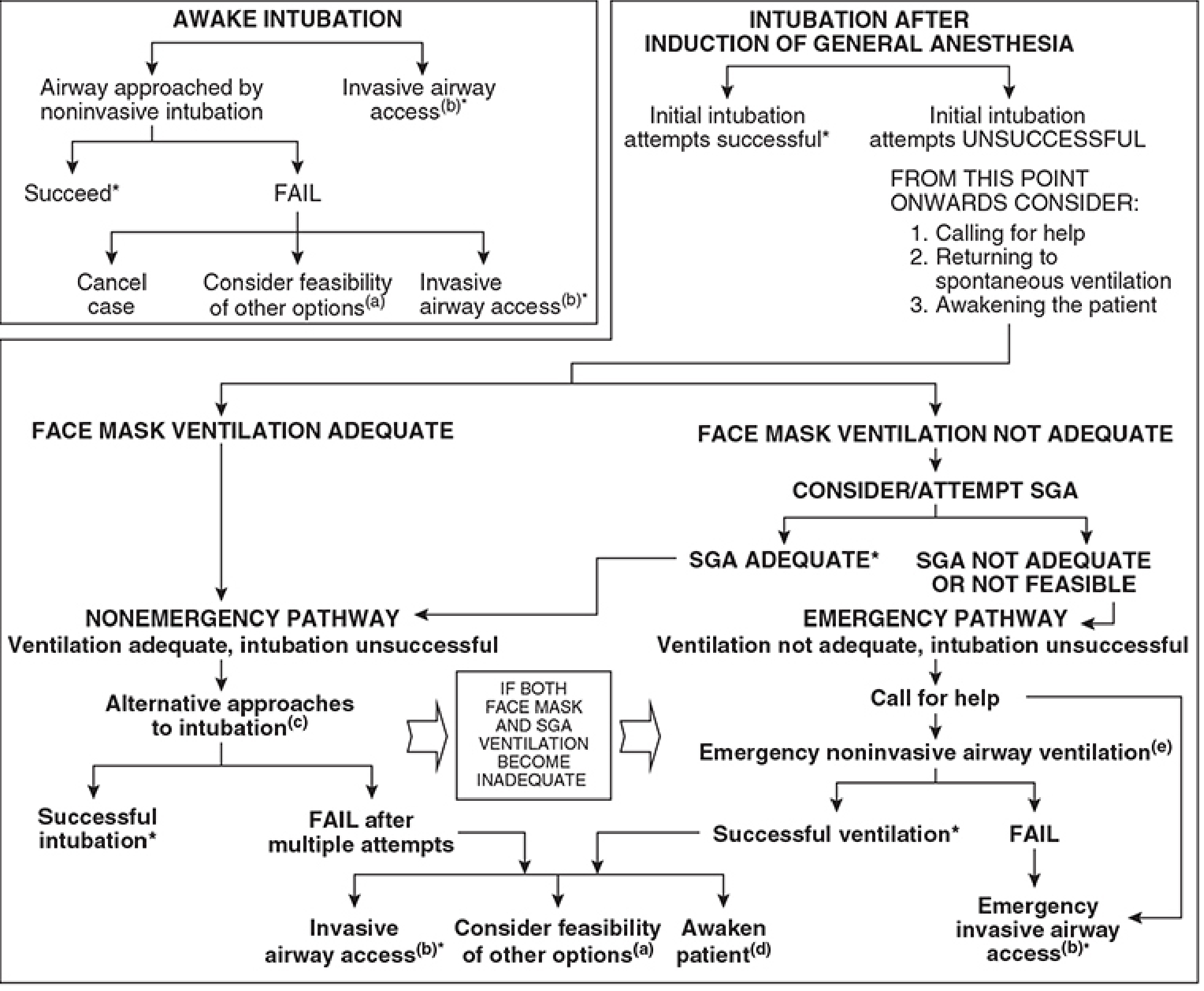
Arm 1 — Predicted Difficult Airway → Awake Intubation
- Airway approached by noninvasive intubation (fiberoptic, video laryngoscopy)
- If fails → Cancel case or consider other options or invasive airway access
- Invasive airway access (a) is always an option
Arm 2 — Intubation After Induction (Non-emergency Pathway)
- Call for help; consider returning to spontaneous ventilation; consider awakening the patient
- Alternative approaches to intubation (see note c below)
- If multiple attempts fail → Invasive airway access OR consider other options OR awaken patient
Arm 3 — Emergency Pathway (CICV)
- Face mask ventilation NOT adequate → Attempt SGA
- SGA adequate → "Stop and Think" (nonemergency pathway)
- SGA NOT adequate → Emergency pathway: call for help → Emergency noninvasive airway ventilation (SGA attempt) → If fails → Emergency invasive airway access
DAS Algorithm 2015 — Unanticipated Difficult Intubation in Adults
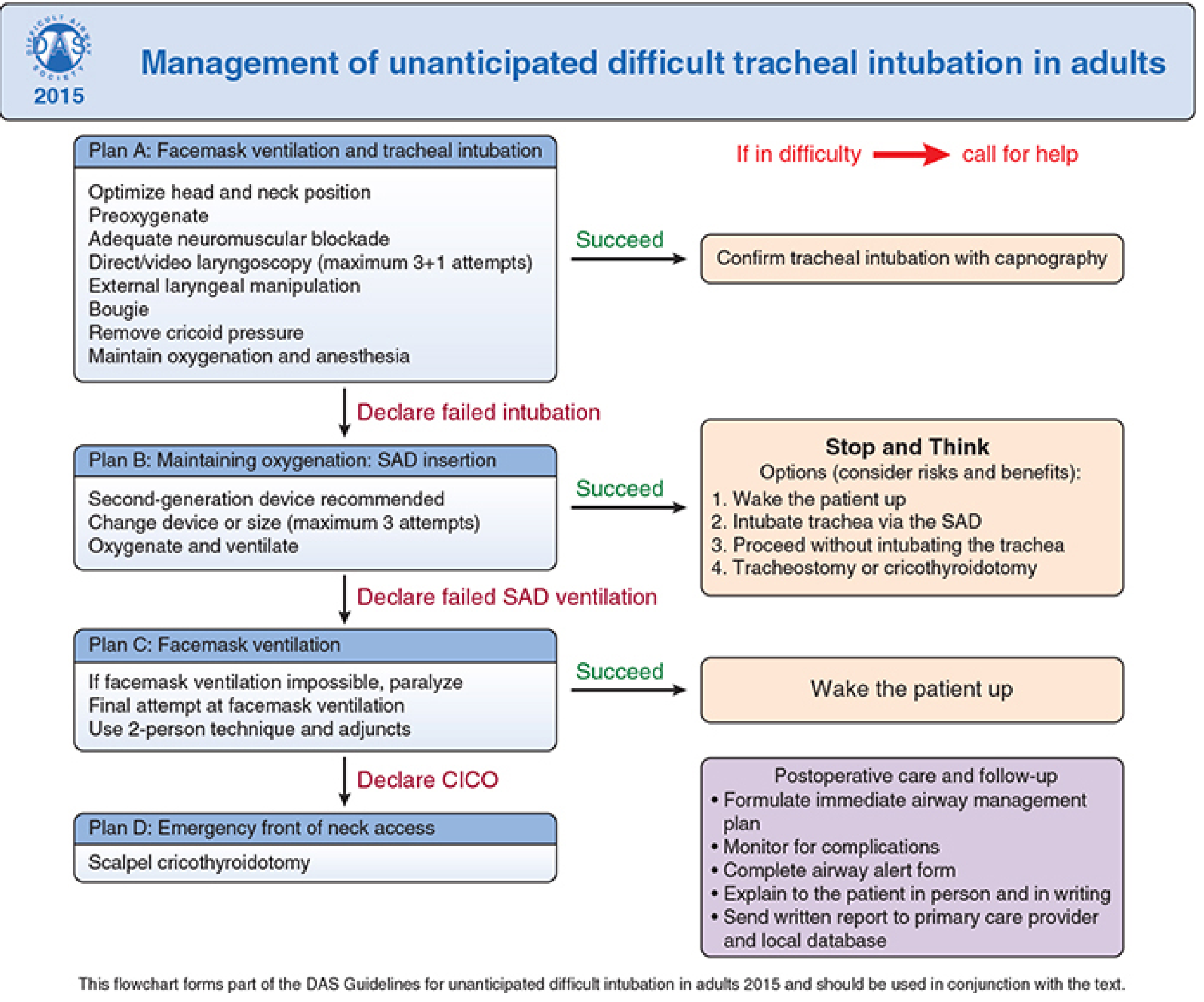
| Plan | Focus | Max Attempts |
|---|---|---|
| Plan A | Facemask ventilation + tracheal intubation | 3+1 (direct/video laryngoscopy) |
| Plan B | SAD (supraglottic airway device) insertion | 3 attempts, prefer 2nd-generation |
| Plan C | Facemask ventilation rescue | 2-person technique + adjuncts |
| Plan D | Front-of-neck access (FONA) — scalpel cricothyrotomy | Definitive |
- Palpable CTM: transverse stab incision → turn blade 90° → bougie via blade → railroad 6-mm cuffed tube → confirm with capnography
- Impalpable CTM: 8–10 cm vertical skin incision → blunt dissection → identify larynx → proceed as above
Algorithm Notes (Footnotes)
| Note | Content |
|---|---|
| (a) Other options | Surgery under face mask/SGA anesthesia, regional/local anesthesia — limited value once emergency pathway reached |
| (b) Invasive airway | Surgical or percutaneous cricothyrotomy, tracheostomy, jet ventilation, retrograde intubation |
| (c) Alternative intubation | Videolaryngoscopy, alternate blades, SGA as intubation conduit (±fiberoptic), fiberoptic intubation, intubating stylet/tube changer, light wand, blind oral/nasal |
| (d) Re-prepare | Consider re-preparation for awake intubation or case cancellation |
| (e) Emergency noninvasive | SGA (preferred), rigid bronchoscope, transtracheal jet ventilation |
Oxygen Delivery — Continuously Throughout
- Preoxygenation with 100% O₂ (8 breaths of VC or 3–5 min tidal breathing)
- Apneic oxygenation (high-flow nasal O₂ at 15 L/min) to extend safe apnea time
- Confirm ventilation/intubation/SGA placement with exhaled CO₂ at every step
Emergency Department Context (Rosen's)
- Patient is rapidly deteriorating (anaphylaxis with angioedema, severe status asthmaticus, premature extubation)
- Impending arrest or complete obstruction within seconds to minutes
- No time for awake intubation preparation
Other International Algorithms
| Organization | Key Features |
|---|---|
| DAS (UK, 2015) | Plans A–D; scalpel cricothyrotomy as FONA standard |
| CAFG (Canada) | Emphasizes awake technique for anticipated difficulty |
| SFAR (France) | Similar stepwise approach |
| NAP4 data | Human factors contribute to adverse outcomes in >40% of cases |
- Do not repeat the same failed technique
- Awake intubation for the anticipated difficult airway
- SGA as rescue for difficult mask ventilation
- Emergency invasive access (FONA) for CICO
- Limit intubation attempts (typically ≤3 + 1 by a senior colleague)
Post-incident Follow-up
- Document clearly in the medical record
- Complete an airway alert form
- Explain to the patient in person and in writing
- Send written report to the primary care provider and local database
- Urgent review of any cricothyrotomy site
Which is the most recent DAS guidelines
Difficult Airway Society DAS guidelines most recent update 2024 2025
Difficult Airway Society guidelines
DAS 2025 guidelines unanticipated difficult tracheal intubation adults key changes British Journal Anaesthesia
"difficult airway society" AND "unanticipated difficult" AND intubation
PMID: 41203471
DAS 2025 guidelines key changes from 2015 Plan A B C D videolaryngoscopy eFONA summary
site:trucorp.com OR site:nysora.com DAS 2025 guidelines Plan A videolaryngoscopy HFNO physiologically difficult airway eFONA recommendations
DAS 2025 intubation guidelines 65 recommendations "physiologically difficult" obesity HFNO eFONA scalpel details
DAS 2025 Guidelines — Summary
What's Retained from 2015
| Plan | Focus |
|---|---|
| A | Tracheal intubation (optimised) |
| B | Supraglottic airway device (SAD) ventilation |
| C | Facemask ventilation rescue |
| D | Emergency front-of-neck airway (eFONA) |
Key Changes / New Emphases in 2025
1. Shift in Philosophy — "Maximise Success, Not Just Manage Failure"
2. Plan A — Videolaryngoscopy as the Default
- Videolaryngoscopy (VL) is now integrated early in Plan A, not just as an alternative — reflecting strong evidence that it improves glottic view and reduces failed intubation rates vs. direct laryngoscopy.
- Emphasis on: optimised patient positioning, adequate neuromuscular blockade, bougie use, and skilled VL technique.
3. Continuous Oxygenation / "Peroxygenation"
- High-flow nasal oxygen (HFNO) now explicitly recommended throughout airway management to extend safe apnoea time.
- Term "peroxygenation" used to describe oxygen delivery throughout the procedure (pre-, during, and post-attempt), not just pre-oxygenation.
4. The Physiologically Difficult Airway — New Dedicated Section
- Explicit recognition that physiological derangement (haemodynamic instability, severe hypoxaemia, metabolic acidosis, right heart failure) increases airway risk as much as anatomical difficulty.
- Specific guidance on how to optimise physiology before intubation in these patients.
- Awake tracheal intubation (ATI) is a priority in the physiologically compromised patient.
5. Obesity — Specific Recommendations
- Obesity elevated from a footnote to a distinct clinical phenotype with dedicated guidance.
- Early use of a second-generation SAD (better seal, intubation conduit option).
- ATI considered a physiological priority in complex obese patients.
6. Plan D — eFONA (Emergency Front-of-Neck Airway)
- Scalpel cricothyrotomy remains the preferred technique (over needle/cannula) for adults.
- Updated technical details: scalpel held in dominant hand, incisions made away from non-dominant hand.
- The vertical eFONA technique is largely unchanged from 2015; alternative scalpel–bougie–tube techniques also acceptable.
- Acknowledges ongoing debate around impalpable cricothyroid membrane management.
7. New Topic Areas (Not in 2015)
| New Area | Key Points |
|---|---|
| Rapid Sequence Induction (RSI) | Dedicated recommendations for RSII |
| Point-of-care ultrasound (POCUS) | For pre-procedural airway assessment and CTM identification |
| Human factors | Explicit recommendations on cognitive load, team communication, CRM |
| Documentation | Standardised documentation requirements post-event |
| Education & training | Structured, simulation-based, multidisciplinary airway training |
| Post-intubation care | Handover, waveform capnography, monitoring requirements |
8. Waveform Capnography — Mandatory at Every Step
9. Team-Based Approach Formalised
- Pre-procedure team briefing mandatory.
- Airway strategy must be communicated with the anaesthetic assistant.
- History of previous difficulty must guide planning.
Other Current DAS Guidelines (Full Suite)
| Guideline | Year |
|---|---|
| Unanticipated difficult tracheal intubation in adults | 2025 |
| Awake tracheal intubation (ATI) | 2020 |
| Extubation guidelines | 2012 (under review) |
| Videolaryngoscopy | Separate guidance |
| Obstetric airway | Separate guidance |
| Paediatric airway | Separate guidance |
Extubation criteria
Extubation Criteria
The Two Core Questions
- Can the patient maintain a patent upper airway and protect it?
- Can the patient sustain adequate oxygenation and ventilation independently?
I. Criteria for Extubation — Post-operative / Routine Anesthesia
Neurological / Level of Consciousness
| Criterion | Detail |
|---|---|
| Follows commands | Opens eyes, squeezes hand on request |
| Purposeful movement | Spontaneous or to stimulation |
| Airway protective reflexes | Intact cough and gag |
| Pain adequately controlled | Prevents splinting/agitation post-extubation |
| Non-combative | Able to cooperate with positioning |
Respiratory
| Criterion | Detail |
|---|---|
| Spontaneous ventilation | Adequate rate and depth |
| Tidal volume | > 5 mL/kg |
| Respiratory rate | < 25 breaths/min |
| Negative inspiratory force (NIF) | More negative than −20 cmH₂O |
| Vital capacity | > 10 mL/kg |
| Minute ventilation | < 10 L/min |
| FiO₂ requirement | < 0.50 to maintain adequate SpO₂ |
| Neuromuscular blockade | Fully reversed (TOF ratio ≥ 0.9) |
Haemodynamic / Systemic
| Criterion | Detail |
|---|---|
| Haemodynamic stability | No active vasopressor dependence for extubation |
| Adequately resuscitated | No ongoing haemorrhage, fluid deficit corrected |
| Normothermic | Shivering impairs gas exchange and increases O₂ demand |
| No signs of sepsis | Ongoing sepsis impairs respiratory reserve |
| Low likelihood of urgent return to OR | Ensures airway won't need to be re-secured imminently |
II. ICU Extubation — Weaning & Liberation Protocol
Step 1 — Daily Screening (Pass all of the following)
| Screening Criterion | Threshold |
|---|---|
| PaO₂/FiO₂ ratio | > 200 |
| PEEP | ≤ 5 cmH₂O |
| FiO₂ | ≤ 0.40–0.50 |
| Cough and airway reflexes | Intact |
| No continuous vasopressor infusion | Or weaning |
| Minimal/no sedation | Or pass SAT (Spontaneous Awake Trial) |
| Cause of respiratory failure | Resolving or resolved |
Step 2 — Spontaneous Breathing Trial (SBT)
- PSV 5–8 cmH₂O + PEEP 5 cmH₂O, or
- T-piece (CPAP 5 cmH₂O), or
- Pressure support 7 cmH₂O / PEEP 5 cmH₂O
Note: Any level of pressure support underestimates the resistance a patient will encounter after extubation, because post-extubation supraglottic work is approximately equal to endotracheal tube resistance. For borderline patients, a brief T-piece trial with zero support is more stringent. — Fishman's Pulmonary Diseases, p. 2617
| Failure Criterion |
|---|
| RR > 35/min for > 5 minutes |
| SpO₂ < 90% |
| HR > 140/min or ≥ 20% change from baseline |
| SBP < 90 mmHg or > 180 mmHg |
| Increased agitation, anxiety, or diaphoresis |
Rapid Shallow Breathing Index (RSBI)
- RSBI = RR (breaths/min) ÷ Tidal Volume (litres)
- RSBI < 105 is classically used as a predictor of successful extubation
- Caution: recent meta-analyses show only moderate sensitivity and poor specificity — do not use in isolation — Sabiston Textbook of Surgery
Other Respiratory Mechanics (ancillary)
| Parameter | Target |
|---|---|
| NIF (MIP) | More negative than −20 cmH₂O |
| Tidal Volume | > 5 mL/kg |
| Vital Capacity | > 10 mL/kg |
| Minute Ventilation | < 10 L/min |
| SBT oxygenation | PaO₂ > 80 mmHg on FiO₂ 0.4 + CPAP 5 cmH₂O |
III. Cuff Leak Test
- Deflate ETT cuff → measure volume/audible leak on ventilation
- Expected leak: 10–20% of ventilated tidal volume
- No cuff leak → suggests airway oedema → risk of post-extubation stridor/obstruction
- Management if no leak: IV dexamethasone (e.g. 0.1–0.2 mg/kg), reassess in 24 hours
- A persistent absent cuff leak over multiple days is not an absolute contraindication — extubation can proceed with preparations for reintubation in place
IV. Awake vs Deep Extubation
| Feature | Awake Extubation | Deep Extubation |
|---|---|---|
| Airway reflexes | Intact | Suppressed |
| Coughing/straining | More likely | Minimised |
| ICP/IOP/BP response | Increased | Reduced |
| Laryngospasm risk | Lower (reflexes intact) | Higher (intermediate depth) |
| Aspiration risk | Lower | Higher |
| Preferred in | Difficult airway, full stomach, OSA, neurosurgery, thoracic surgery | Airway surgery where coughing risks haemostasis or bronchospasm |
| Contraindications to deep | Copious secretions, difficult airway, OSA, high aspiration risk, inadequately trained PACU staff | — |
V. DAS Extubation Guidelines (2012, under revision)
| Category | Description |
|---|---|
| Low risk | Normal airway, no complicating factors |
| At-risk | Difficult intubation history, airway surgery, obesity, aspiration risk, obstructive pathology, reduced conscious level |
- Optimise the patient before extubation
- Formulate a plan for failure (airway exchange catheter, senior backup present)
- Perform extubation in a controlled, senior-supervised environment
- Have a post-extubation management plan ready
VI. Post-Extubation Management
| Intervention | Indication |
|---|---|
| High-flow nasal oxygen (HFNO) | Prevention of post-extubation failure in low-risk; after prolonged ventilation |
| NIV / BiPAP immediately post-extubation | High-risk patients: age > 65, COPD, cardiac disease, chronic hypercapnia, >24h intubation — start before ARF develops |
| NIV for rescue | Once post-extubation ARF develops, evidence is weak — may delay reintubation and worsen mortality (Esteban trial) |
| Prompt reintubation | If any doubt — do not delay with failed NIV rescue |
10–20% of patients who pass an SBT fail extubation. Mortality among reintubated patients is >6 times higher than those who tolerate extubation — likely reflecting underlying severity of illness, not the reintubation itself. — Fishman's Pulmonary Diseases
VII. Failure to Wean — Causes to Exclude
- Residual neuromuscular blockade
- Critical illness myopathy/polyneuropathy
- Acid-base disturbance (metabolic alkalosis → blunted drive; non-AG acidosis → compensatory tachypnoea)
- Delirium, anxiety, PTSD
- Unresolved sepsis or infection
- Nutritional depletion (diaphragm weakness)
- Small ETT (increased resistance)
I want the extubation criteria solely from Millers
Extubation — Miller's Anesthesia, 10e
General Preparations for Extubation
- Adequate reversal or recovery from neuromuscular blockade
- Haemodynamic stability
- Normothermia
- Adequate analgesia
- Preoxygenate with 100% FiO₂
- Consider alveolar recruitment manoeuvres
- Suction the pharynx (and trachea if indicated)
- Remove throat packs
- Place a bite block (rolled gauze between molars — not an OPA)
- Inspect pilot balloon to confirm complete cuff deflation before removal (inflated cuff can cause vocal cord injury or arytenoid dislocation)
- If high-pressure mask ventilation was used → pass orogastric tube and suction to reduce aspiration risk
Box 62.11 — Criteria for OR or PACU Extubation of the Trauma Patient
Mental Status
- Resolution of intoxication
- Able to follow commands
- Non-combative
- Pain adequately controlled
Airway Anatomy and Reflexes
- Appropriate cough and gag
- Ability to protect airway from aspiration
- No excessive airway oedema or instability
Respiratory Mechanics
- Adequate tidal volume and respiratory rate
- Normal motor strength
- Required FiO₂ < 0.50
Systemic Stability
- Adequately resuscitated
- Small likelihood of urgent return to OR
- Normothermic, without signs of sepsis
Complications Associated with Extubation (Box 40.5)
- Laryngospasm and bronchospasm
- Upper airway obstruction
- Hypoventilation
- Respiratory drive failure (residual anaesthetic, decreased CO₂/O₂ response)
- Hypoxia (atelectasis)
- Vocal fold obstruction (laryngospasm, oedema, paralysis)
- Tracheal obstruction (subglottic oedema, tracheomalacia)
- Aspiration
- Hypertension, tachycardia
- Increased ICP / IOP / pulmonary artery pressure
- Increased bronchial stump pressure (post-pulmonary resection)
Awake vs Deep Extubation
| Awake | Deep | |
|---|---|---|
| Airway reflexes | Intact — better airway maintenance | Suppressed |
| Coughing/haemodynamic response | Present | Avoided |
| Risk | Laryngospasm on ETT removal | Upper airway obstruction, hypoventilation |
- Stage II anaesthesia (excitatory phase) must be avoided — highest risk of laryngospasm
- The Bailey manoeuvre (exchange ETT for SGA under deep anaesthesia) is an alternative
Position for extubation:
- Sniffing position — standard; optimal for airway rescue if needed
- Head-up — preferred in morbid obesity and high aspiration risk
- Lateral decubitus — when aspiration risk is high
Extubation of the Difficult Airway (Box 40.6)
- Known difficult airway
- Airway deterioration (bleeding, oedema, trauma)
- Restricted airway access
- Obesity and obstructive sleep apnoea
- Aspiration risk
- Cardiovascular disease
- Respiratory disease
- Preferred technique: Airway Exchange Catheter (AEC)
- Placed through ETT before extubation, kept in situ until reintubation risk has passed
- Can connect to capnograph for respiratory monitoring
- Oxygen insufflation is possible but carries significant barotrauma risk — if used in emergency, limit to 2 L/min as a temporising measure only
- Smaller AECs (11 Fr) are well-tolerated by awake patients — secure with tape, label clearly
- Extubation plan must always include a reintubation strategy formulated in advance
"Although considerable emphasis is placed on the problems that can arise during induction and intubation, the risk of complications can potentially be higher during extubation of the trachea." — Miller's Anesthesia, 10e, p. 5962
Please include what commands he should be following
Commands & Clinical Tests for Extubation Readiness — Miller's Anesthesia, 10e
Commands / Clinical Tests (in an Awake Patient)
| Test | What to Ask/Do | Significance per Miller's |
|---|---|---|
| Open eyes widely | "Open your eyes" | Possible at TOF ~0.6, but NMB still significant |
| Stick out your tongue | "Stick out your tongue" | Possible at TOF ~0.6 |
| Lift legs off the bed | "Lift your legs" | General motor strength assessment |
| 5-second head lift | "Lift your head off the pillow and hold it" | Historically the gold standard — correlates with TOF ~0.60; insensitive — should NOT be used alone |
| Grip strength | "Squeeze my fingers" | Still ~60% of normal at TOF 0.70–0.75 — unreliable in isolation |
| Bite against a tongue depressor | Oppose incisor teeth against depressor | Most reliable clinical indicator of pharyngeal muscle tone; correlates with TOF ratio ~0.85 — preferred over head lift |
Important Caveats from Miller's
- None of these tests alone are sufficient to confirm adequate NMB reversal. Objective quantitative TOF monitoring is required:
- TOF ratio ≥ 0.9 (MMG/EMG) or ≥ 1.0 (AMG) to exclude residual block
- The 5-second head lift, despite being the "gold standard," is remarkably insensitive — patients can perform it at a TOF ratio as low as 0.60, at which point pharyngeal and upper oesophageal function remains impaired
- Opposing incisor teeth against a tongue depressor correlates with a TOF ~0.85 and is a more reliable indicator of airway-protective muscle tone than the head lift
- At TOF ≤ 0.4: patient is unable to lift the head or arm at all
- At TOF ~0.6: patient can open eyes, stick out tongue, and lift head for 3 seconds — but vital capacity and inspiratory force are still reduced
- At TOF 0.7–0.75: can cough and sustain head lift for 5 seconds, but grip strength still ~60% of normal
- At TOF ≥ 0.8: vital capacity and inspiratory force return to normal — but diplopia, blurred vision, and facial weakness may persist
"The ability to strongly oppose the incisor teeth against a tongue depressor is a more reliable indicator of pharyngeal muscle tone... correlating with an average TOF ratio of 0.85 as opposed to 0.60 for the sustained head lift." — Miller's Anesthesia, 10e, p. 11569