Indications for sentinel lymph nodes biopsy in breast cancer
Reading File
Finding Sources
Searching PubMed
"sentinel lymph node biopsy" AND "breast cancer" AND indications
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative surgical textbooks. Here is a thorough answer:
Sentinel Lymph Node Biopsy (SLNB) in Breast Cancer: Indications
SLNB has replaced axillary lymph node dissection (ALND) as the standard axillary staging procedure for most breast cancer patients. It identifies the first-echelon ("sentinel") node draining the breast, thereby predicting the nodal status of the entire axilla while sparing women the morbidity of full ALND (lymphedema: ~8% vs. ~14-75% with ALND).
INDICATIONS (SLNB Recommended)
Based on ASCO Clinical Practice Guidelines and the 2022 NCCN guidelines:
1. Early invasive breast cancer (standard indication)
- T1 or T2 tumors (up to 5 cm) - the core indication
- Possibly T3 tumors (>5 cm) in select cases
- Clinically node-negative (cN0) disease - no palpable or imaging-detected nodal involvement
2. Either sex
- SLNB is appropriate in both female and male patients with cN0 disease
3. Unicentric or multicentric disease
- Multifocal/multicentric breast cancer with clinically negative nodes is an accepted indication
4. DCIS (ductal carcinoma in-situ) - specific circumstances
- When mastectomy is planned (re-operative SLNB would not be feasible later)
- When high-risk features exist that raise concern for invasive disease on final pathology:
- High-grade tumors
- ER/PR-negative tumors
- Large-size tumors
- Mass-forming tumors
5. After prior breast surgery
- SLNB is feasible (though may have altered lymphatic drainage patterns; preoperative lymphoscintigraphy may help)
6. After neoadjuvant chemotherapy (NACT) - the expanding frontier
- Originally cN0 patients undergoing NACT: SLNB after NACT is acceptable
- Originally cN1-2 patients downstaged to ycN0 following NACT (Targeted Axillary Dissection [TAD]):
- Three landmark trials (ACOSOG Z1071, SENTINA, SN-FNAC) demonstrated feasibility
- FNR is reduced to <10% when: (a) dual-tracer technique is used, AND (b) ≥3 sentinel nodes are retrieved, AND (c) the biopsy-proven clipped node is excised alongside SLNB
- cN1 patients with ≤1 suspicious node before NACT, or when all suspicious nodes are marked and retrieved via TAD
7. Patients with 1-2 positive SLNs (to avoid completion ALND)
Under ACOSOG Z0011 criteria, ALND can be omitted (SLNB alone is adequate treatment) if:
- cT1-T2, cN0
- 1-2 positive SLNs (macrometastasis, no gross extranodal extension)
- Breast-conserving surgery with whole-breast adjuvant radiotherapy
- No neoadjuvant chemotherapy
- Updated 2022 NCCN: also extends to mastectomy patients if adjuvant axillary nodal radiotherapy is given (AMAROS/OTOASAR trial support)
8. Micrometastasis (N1mi) in SLNs
- Patients with micrometastasis (≤2 mm) found on SLNB do not require completion ALND; SLNB alone yields equivalent outcomes
SLNB NOT RECOMMENDED (Contraindications)
| Situation | Reason |
|---|---|
| T4 tumors (skin ulceration / chest wall invasion) | Advanced local disease |
| Inflammatory breast cancer | Lymphatic obstruction makes mapping unreliable |
| Clinically positive axilla (cN+) without NACT | Direct ALND indicated |
| Recurrent axillary disease | Prior surgery disrupts lymphatics |
| Prior axillary surgery (ALND already done) | No functional sentinel node remains |
| More than "limited" nodal involvement (several level I/II nodes, beyond level I/II) | Extensive disease |
| Pregnancy before 30 weeks | Blue dye: risk of anaphylaxis and fetal concerns; technetium-99m: limited safety data before 30 weeks (methylene blue is also contraindicated in pregnancy) |
Summary Table
| Category | SLNB Status |
|---|---|
| cT1-T2 cN0 (any histology) | Standard indication |
| cT3 cN0 | Possible/acceptable |
| DCIS + mastectomy planned | Indicated |
| DCIS + high-risk features | Indicated |
| Multicentric disease, cN0 | Indicated |
| Male breast cancer, cN0 | Indicated |
| Originally cN1, downstaged to ycN0 post-NACT (TAD) | Indicated with precautions |
| Inflammatory breast cancer | Contraindicated |
| T4 disease | Contraindicated |
| cN+ without NACT | Contraindicated |
| Pregnancy <30 weeks | Relatively contraindicated |
Key landmark trials informing these indications:
- ACOSOG Z0011 - established SLNB alone (omitting ALND) for 1-2 positive SLNs in breast conservation
- ACOSOG Z1071, SENTINA, SN-FNAC - established feasibility of SLNB/TAD after NACT in downstaged cN1 patients
- NSABP B-32 - confirmed equivalence of SLNB vs. ALND in cN0 disease for overall survival
Sources: Current Surgical Therapy 14e (Box 1, ASCO Guidelines); Fischer's Mastery of Surgery 8e; Bailey & Love's Short Practice of Surgery 28e; Mulholland & Greenfield's Surgery 7e
Ducta ectasia
Finding Sources
Searching PubMed
"duct ectasia" AND breast
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is a full overview:
Ductal Ectasia (Mammary Duct Ectasia)
Definition
Ductal ectasia is a benign, non-proliferative disorder of the breast defined as dilatation of the major (subareolar) milk ducts. It is classified under the ANDI (Aberrations of Normal Development and Involution) framework as a disorder of involution, not a premalignant condition.
- Second most common cause of nipple discharge after intraductal papilloma (accounts for 17-36% of cases)
- Typically affects women in the fifth or sixth decade of life (perimenopausal/postmenopausal); also occurs in multiparous women
- Unlike periductal mastitis/Zuska disease, it is NOT associated with cigarette smoking
Pathogenesis
Two competing theories exist:
Haagensen's theory (primary ductal event):
Dilated ducts → stagnation and inspissation of secretions → epithelial ulceration → leakage of chemically irritating fatty acids into periductal tissue → local inflammatory reaction → periductal fibrosis → nipple retraction
Alternative theory (primary periductal mastitis):
Periductal inflammation is primary → weakening of duct walls → secondary ductal dilatation
Both processes likely occur and together explain the wide clinical spectrum.
Pathology (Morphology)
- Ectatic, dilated ducts filled with inspissated (thickened) secretions and numerous lipid-laden macrophages
- Duct rupture triggers a periductal and interstitial chronic inflammatory reaction - lymphocytes, macrophages, and variable numbers of plasma cells (hence the older term "plasma cell mastitis")
- Granulomas may form around cholesterol deposits and secretions
- Subsequent fibrosis produces an irregular periareolar mass with skin and nipple retraction
Clinical Features
| Feature | Details |
|---|---|
| Nipple discharge | Thick, toothpaste-like, multicolored: brown, green, muddy, or black; from multiple ducts; can be bloodstained |
| Periareolar mass | Palpable, often tender - from periductal fibrosis |
| Nipple retraction/inversion | Due to periductal fibrosis and scarring (acquired inversion in 5th-6th decade) |
| Pain/tenderness | Periareolar, but pain and erythema are relatively uncommon in pure duct ectasia |
| Age | Typically peri- or postmenopausal women; multiparous |
Important: Clinical and radiologic findings of duct ectasia can closely mimic carcinoma (irregular mass, skin retraction, nipple inversion) - this is its principal clinical significance. Carcinoma accounts for 5-20% of acquired nipple retraction cases.
Investigations (Triple Assessment)
1. Ultrasound (first-line imaging)
- Dilated major milk ducts >3 mm in diameter in the subareolar region
- Useful for initial assessment, particularly in younger women
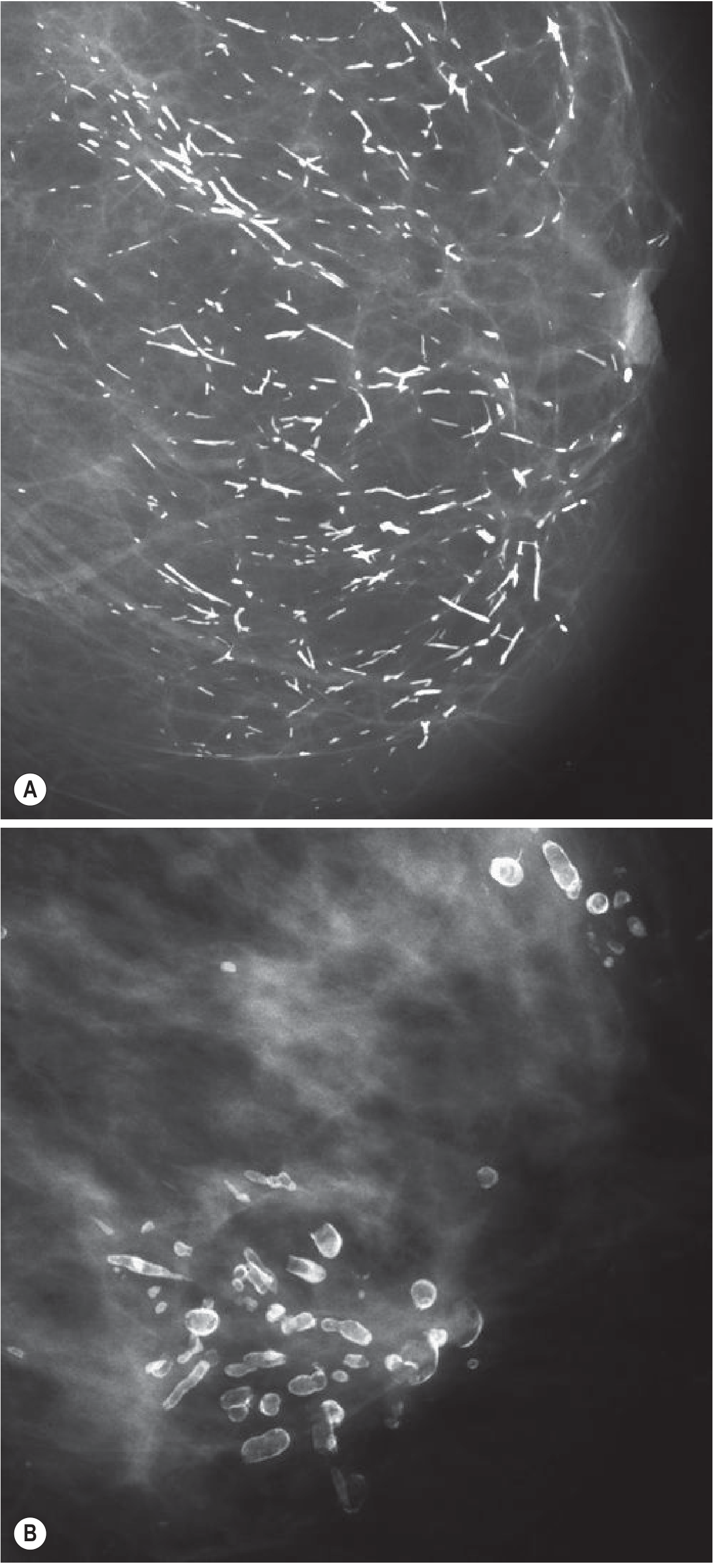
2. Mammography
- Coarse rod-shaped and branching calcifications due to calcification of inspissated debris within dilated ducts
- Described as having a "broken needle" appearance (characteristic)
- Typically bilateral and symmetrical
- Debris extruding from ducts may cause fat necrosis and a "lead-pipe" appearance
- In some cases, biopsy is required if calcifications are unilateral or focal
3. Core needle biopsy / excision biopsy
- Required if triple assessment is inconclusive or if malignancy cannot be excluded
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Invasive carcinoma | Malignant cells on biopsy; irregular spiculated mass; malignant calcifications |
| Periductal mastitis / Zuska disease | Associated with smoking; squamous metaplasia of ducts; recurrent subareolar abscess; fistula to areolar edge |
| Intraductal papilloma | Single duct bloody/serous discharge; most common cause of nipple discharge |
| Breast abscess | Acute inflammation, fever, lactating women |
Key distinction from periductal mastitis (Zuska disease):
- Duct ectasia: NOT associated with smoking; plasma cells dominate; discharge is multicolored/thick
- Periductal mastitis: >90% are smokers; squamous metaplasia of duct epithelium; keratin plugging leads to abscess and areolar fistula
Nipple Discharge Colour Guide
| Discharge Type | Likely Cause |
|---|---|
| Bloodstained (single duct) | Intraductal papilloma, intraductal carcinoma, duct ectasia |
| Bloodstained (multiple ducts) | Carcinoma, duct ectasia |
| Black, green, muddy, brown | Duct ectasia (classic) |
| Purulent | Periductal mastitis |
| Milky | Galactorrhoea (prolactinoma, drugs) |
| Serous/sticky | Papilloma, ductal hyperplasia, duct ectasia |
Management
Conservative (most cases):
- Triple assessment (clinical exam + imaging + biopsy if needed) to exclude malignancy
- Antibiotics if inflammation/infection is present:
- Co-amoxiclav, flucloxacillin, or ciprofloxacin + metronidazole or tinidazole (anti-anaerobic cover) for 2-3 weeks
Surgical:
- Major mammary duct excision (Hadfield's operation) - indicated for:
- Profuse or persistent nipple discharge
- Subareolar abscess formation
- Failure to respond to antibiotics
- When malignancy cannot be excluded
Note: Reassurance with ongoing clinical surveillance is adequate if the full workup is normal (especially in cases of nipple retraction without a mass).
Cancer Risk
Duct ectasia is classified as a nonproliferative disorder - it carries NO increased risk of breast cancer. This contrasts with proliferative lesions (with or without atypia) which do confer elevated risk.
Sources: Bailey & Love's Short Practice of Surgery 28e; Robbins, Cotran & Kumar Pathologic Basis of Disease; Schwartz's Principles of Surgery 11e; Berek & Novak's Gynecology; Grainger & Allison's Diagnostic Radiology; Current Surgical Therapy 14e
This is a shared conversation. Sign in to Orris to start your own chat.