Malunion of distal end of radius
Reading File
Finding Sources
Finding Sources
Searching PubMed
"distal radius" AND "malunion" AND treatment
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here is the complete overview:
Malunion of the Distal End of Radius
Definition
Malunion occurs when a fracture heals in an unacceptable position. For the distal radius, no universally accepted single definition exists, but the following radiographic parameters are used to define a clinically significant malunion (Rockwood & Green's, 2025):
| Parameter | Malunion Threshold |
|---|---|
| Radial inclination | < 10 degrees |
| Volar tilt | > 20 degrees (volar) or > 20 degrees (dorsal tilt) |
| Radial height | < 10 mm |
| Ulnar variance | > +2 mm |
| Intra-articular incongruity/diastasis | > 2 mm |
Normal values for reference: radial inclination 22-23°, radial height 11-12 mm, volar tilt 11-12°.
Incidence and Risk Factors
Malunion is common, particularly in elderly patients managed nonoperatively. Contributing factors include:
- Failure to achieve or maintain adequate reduction
- Inadequate duration/type of immobilization
- Marked comminution (especially intra-articular fractures)
- Severe osteoporosis
- Disruption of distal radioulnar ligaments
The risk of symptomatic malunion requiring corrective osteotomy is highest in the fourth and fifth decades of life.
Types of Malunion
Distal radius malunions are classified by morphology:
- Dorsally displaced malunion - most common symptomatic type; typically dorsally angulated AND shortened; associated with DRUJ incongruity and type IV carpal instability non-dissociative (DISI pattern)
- Volarly displaced malunion (Smith fracture type) - limits wrist extension; may produce volar intercalated segment instability (VISI) pattern; reduces pronation/supination (supination most affected)
- Intra-articular malunion - articular surface incongruity; may warrant earlier intervention before degeneration sets in
Clinical Features
Patients present with one or more of:
- Pain - localized to radiocarpal joint, DRUJ, or midcarpal joint
- Stiffness - decreased flexion (dorsal malunion), decreased extension (volar malunion), decreased radial/ulnar deviation, decreased pro/supination
- Weakness - reduced grip strength (from altered wrist mechanics + pain)
- Cosmetic deformity - visible wrist angulation ("dinner fork" or reverse dinner fork deformity)
- Median nerve compression symptoms - dorsal tilt increases carpal tunnel pressure
- Attritional tendon ruptures - EPL is most commonly affected; FPL less frequently
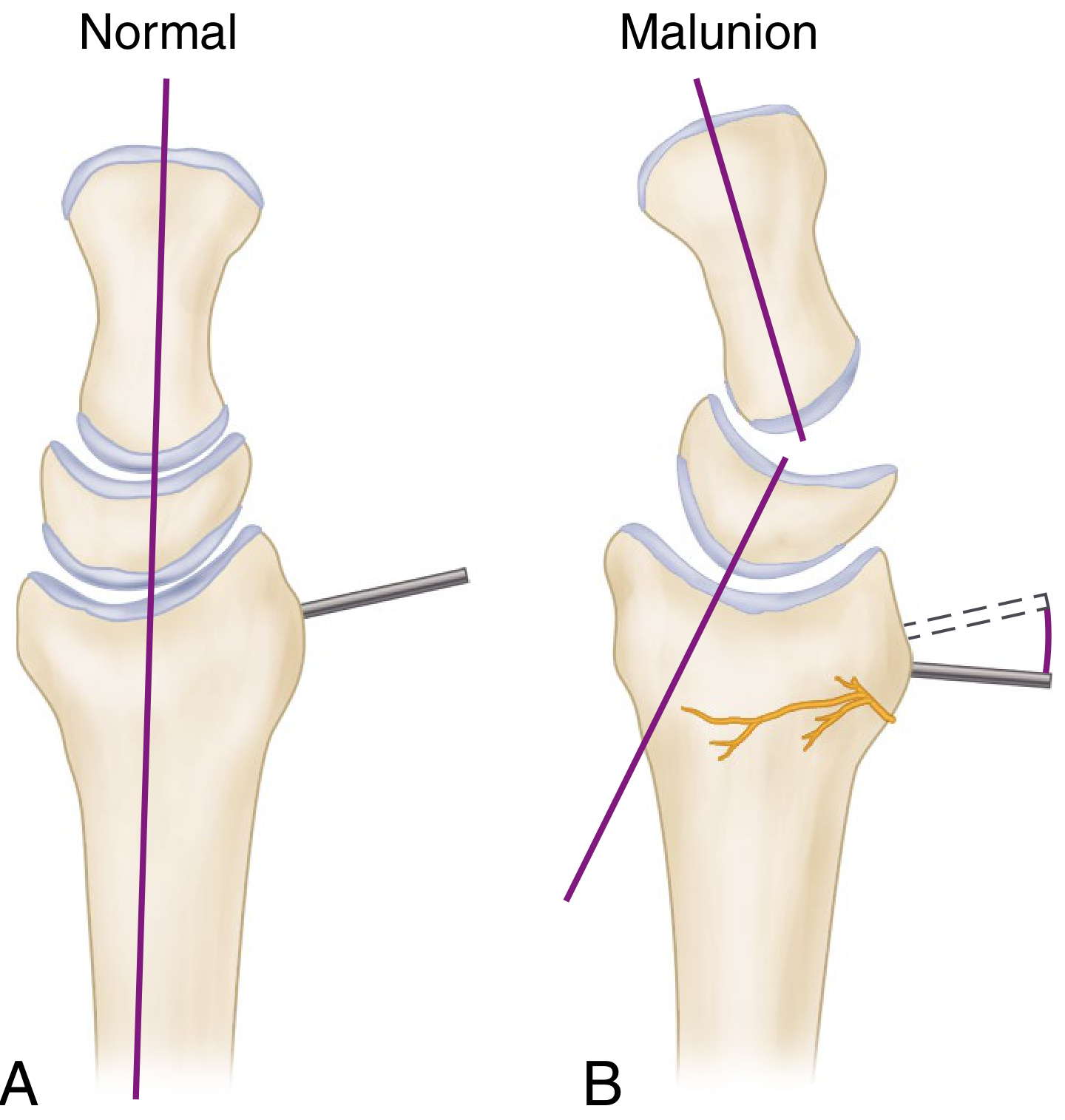
Normal radiocarpal alignment (A) vs dorsal malunion (B) showing carpal collapse pattern resembling DISI without interosseous ligament disruption - Campbell's Operative Orthopaedics, 15th ed.
Radiographic Evaluation
Plain X-rays (AP + lateral of both wrists in neutral rotation):
- Measure radial inclination, radial height, volar tilt, ulnar variance
- Detect carpal subluxation and instability patterns
- Contralateral wrist serves as a template for surgical planning
Parameters associated with poor functional outcome (Graham's criteria):
- Intra-articular incongruity > 2 mm (radiocarpal)
- Step-off at DRUJ > 1-2 mm
- Dorsal angulation > 20 degrees
- Radial inclination < 10 degrees
- Loss of sagittal tilt of 20-30 degrees
- Radial shortening > 6 mm (causes DRUJ dysfunction)
- Fractures with > 25-30 degrees angulation or > 6 mm shortening are more likely to become symptomatic
CT scan: Evaluates DRUJ congruity (axial views), articular surface, ulnar styloid malunion; 3D CT models assist in osteotomy planning
MRI/arthrography: Evaluates TFCC integrity and intercarpal ligaments
Radiological X-ray showing Distal Radius Malunion and Corrective Osteotomy
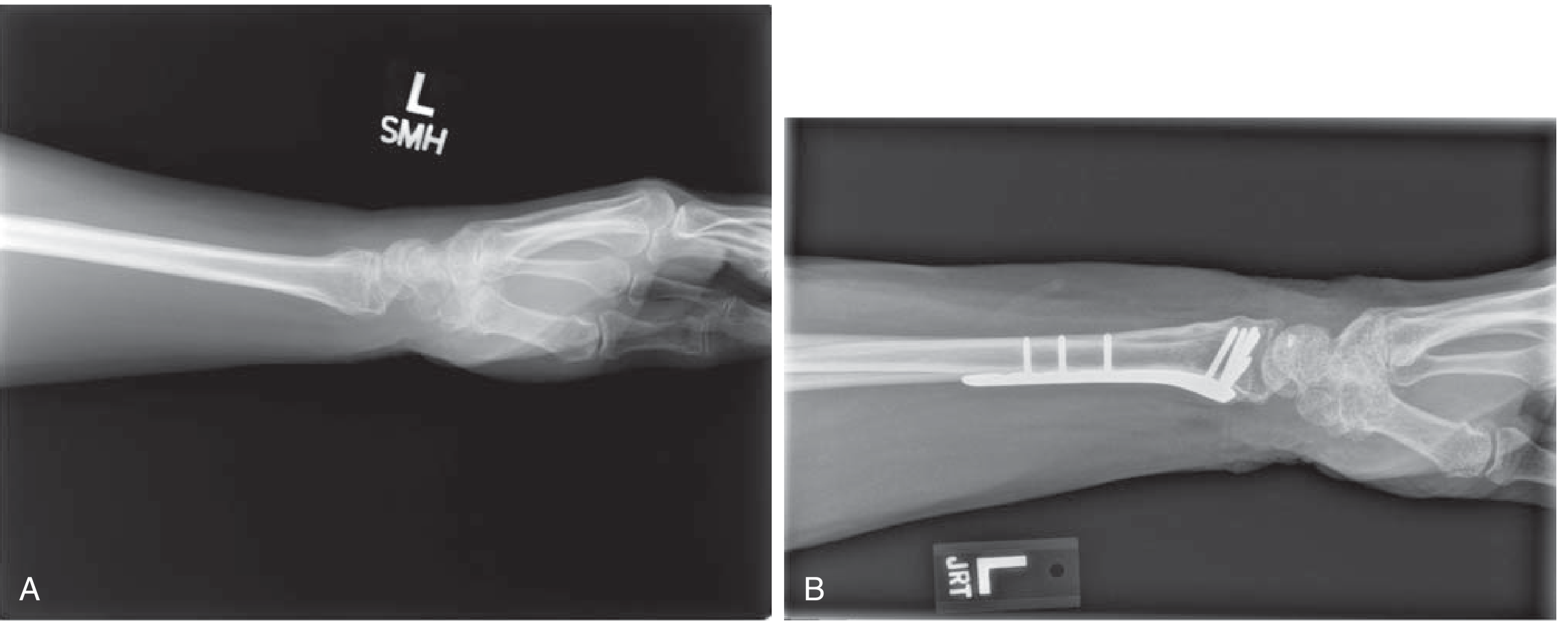
(A) Lateral radiograph showing distal radius malunion with dorsal tilt. (B) Post-corrective osteotomy using a volar locking plate - Miller's Review of Orthopaedics, 9th ed.
Treatment
Non-operative
Observation is appropriate for:
- Elderly patients with low functional demands
- Minimally symptomatic patients despite radiographic deformity
- Patients with active CRPS (must be treated first before any surgery)
Treatment focuses on the symptomatic patient, not radiographic appearance alone.
Operative - Corrective Osteotomy
Indications:
- Pain and functional deficits interfering significantly with daily activities
- Deformity of distal radius or DRUJ on radiographs
- Young active patient (< 40 years) with deformity likely to become symptomatic (articular step-off > 2 mm, carpal instability, > 20-30° dorsal angulation, incongruent DRUJ)
Contraindications:
- Active reflex sympathetic dystrophy / CRPS (must be treated first)
Timing: Traditionally deferred until fracture consolidation, but more recent data support early intervention (as early as 6 weeks) - technically easier and associated with shorter overall disability period.
Techniques by malunion type:
| Malunion Type | Surgical Approach |
|---|---|
| Dorsal displacement (most common) | Opening wedge osteotomy - dorsal or volar approach; volar locked plating avoids need for large corticocancellous graft |
| Severe shortening | Corrective osteotomy for sagittal deformity + ulnar shortening osteotomy to restore DRUJ congruency |
| Volar displacement / intra-articular | No single technique proven superior; goal is to restore radiocarpal and DRUJ congruency |
| Intra-articular malunion | Intraoperative arthroscopy may improve accuracy of reduction |
Computer-assisted 3D planning using CT models is increasingly used for complex deformity correction.
Salvage Procedures
When corrective osteotomy is not feasible (e.g., arthritic changes, elderly patients), salvage options include:
- Darrach procedure (distal ulna resection)
- Sauvé-Kapandji procedure (DRUJ fusion + ulnar pseudarthrosis)
- Wrist arthrodesis (severe radiocarpal arthritis)
Prognosis / Expected Outcomes
Corrective osteotomy rarely restores a normal wrist. Patients should be counseled that:
- Radiographic parameters and functional scores (DASH, Michigan Hand Outcomes Questionnaire) do improve
- Range of motion and grip strength deficits typically persist
- Grip strength rarely exceeds 70% of the contralateral limb even after successful correction
Complications of Corrective Osteotomy
- Infection
- Nonunion / delayed union (higher in distraction-type vs. hinge-type osteotomies; one study reported 50% complication rate after extraarticular osteotomy)
- Loss of reduction
- Implant failure
- Nerve injury
- Tendon injury
- CRPS / Reflex sympathetic dystrophy
Recent Evidence (2024-2026)
A 2024 meta-analysis (Essa et al., J Hand Surg Eur Vol) compared anterior vs. dorsal osteotomy/plating for distal radial malunions. A systematic review (Laane et al., Hand, 2024) examined isolated ulnar shortening osteotomy techniques after distal radius malunion, providing guidance on the optimal surgical technique for DRUJ-related symptoms.
Sources: Rockwood and Green's Fractures in Adults, 10th ed. (2025) | Campbell's Operative Orthopaedics, 15th ed. (2026) | Miller's Review of Orthopaedics, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.