Pulmonary tuberculosis radiology pg answer from standard radiology textbooks high yield everything i need to know for radiology pg Military tb 10 mark
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Pulmonary tuberculosis radiology pg answer from standard radiology textbooks high yield everything i need to know for radiology pg Military tb 10 mark
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from the textbooks and excellent images. Let me compile the full, high-yield radiology PG answer.
Pulmonary Tuberculosis - Radiology PG High-Yield Answer
Sources: Murray & Nadel's Textbook of Respiratory Medicine, Goldman-Cecil Medicine, Harrison's Principles of Internal Medicine, Fishman's Pulmonary Diseases
CLASSIFICATION OF PULMONARY TB (Radiological Perspective)
| Type | Synonyms | Timing | Key Radiological Pattern |
|---|---|---|---|
| Primary TB | Ghon focus disease | First infection | Lower/mid zone opacity + hilar adenopathy |
| Progressive Primary TB | Post-primary in children | Persistent primary | Cavitation, lobar consolidation |
| Reactivation TB | Post-primary, secondary TB | Remote reinfection | Apical/upper lobe cavitation + fibrosis |
| Miliary TB | Disseminated TB | Hematogenous spread | Innumerable 1-3 mm random nodules |
1. PRIMARY TUBERCULOSIS - Radiological Features
Chest X-Ray Findings
The classic "Ranke complex" = Ghon focus + calcified hilar node
- Ghon focus: Focal parenchymal opacity, typically middle or lower lung zone (subpleural)
- Hilar/mediastinal lymphadenopathy: Ipsilateral hilar enlargement is characteristic (right > left)
- Pleural effusion: May be present on the affected side
- Combination of parenchymal opacity + lymphadenopathy = Ghon complex (or primary complex)
- Atelectasis may occur if enlarged nodes compress adjacent bronchi
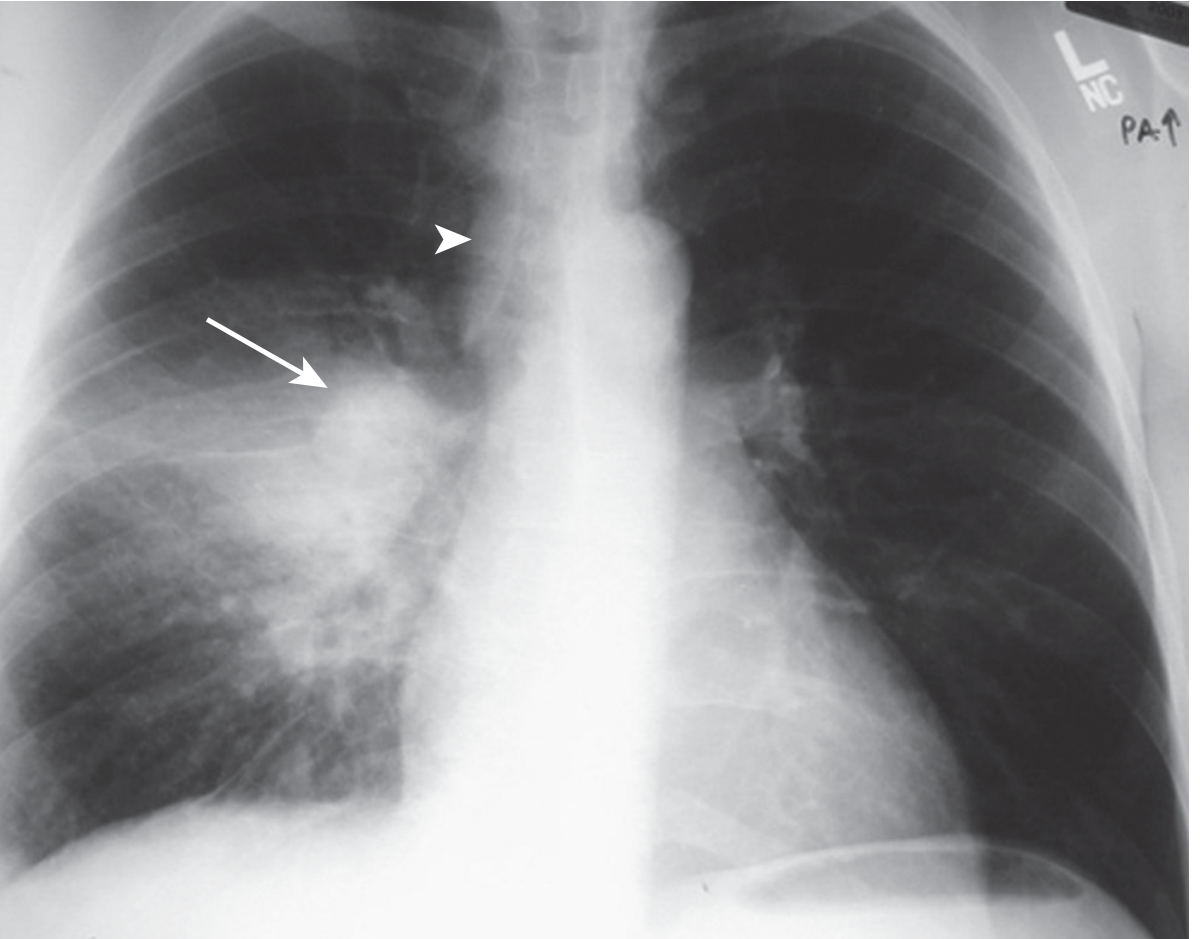
Primary TB: Lower lobe consolidation with hilar adenopathy - Murray & Nadel Fig. 53.1
CT Findings in Primary TB
- Ghon focus: Focal parenchymal opacity with ipsilateral lymphadenopathy
- CT clearly demonstrates lymph node enlargement (more sensitive than CXR)
- Central necrosis in nodes appears as low-density center with rim enhancement
- Air bronchograms visible in areas of consolidation
2. REACTIVATION (POST-PRIMARY) TUBERCULOSIS
Classic Radiological Features - "The Upper Lobe Disease"
Most frequent sites (memorize order):
- Apical and posterior segments of RIGHT upper lobe (most common)
- Apical-posterior segment of LEFT upper lobe
- Superior segments of lower lobes (less common)
Key rule: Anterior segments of upper lobes are rarely involved in reactivation TB - this is a classic exam point.
CXR Pattern Progression
| Stage | Findings |
|---|---|
| Early | Patchy, poorly defined opacity in upper lobes |
| Active/Progressive | Coalescent consolidation, cavity formation |
| Spreading | Tree-in-bud opacities (bronchogenic spread), satellite nodules |
| Healing | Fibrosis, volume loss, calcification |
| Healed | Fibrocavitary scarring, calcified nodules, pleural thickening |
Cavitation in Reactivation TB
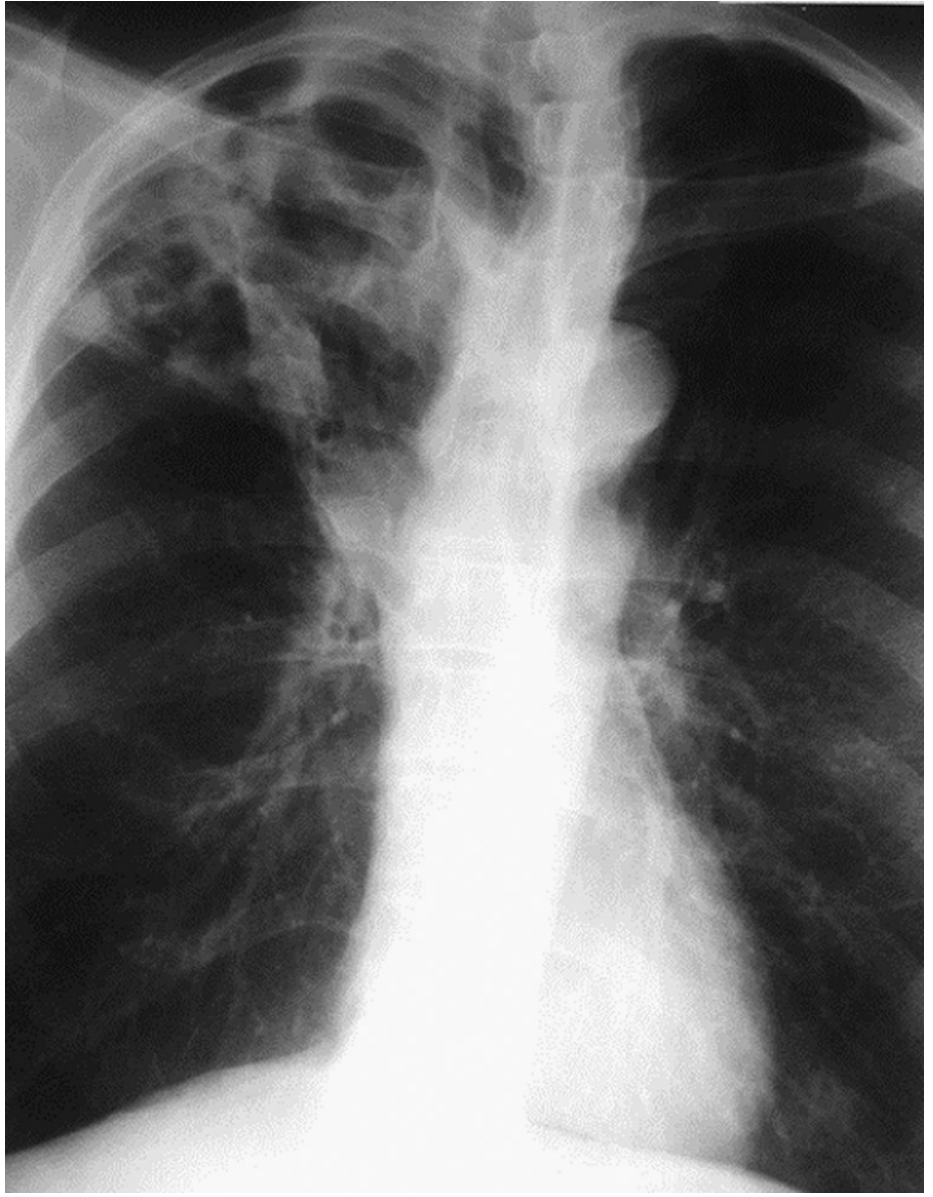
Cavitary TB: Right upper lobe cavitation - Murray & Nadel Fig. 53.2
- Cavities form by liquefaction necrosis and drainage into airways
- Typically thick-walled initially, thin-walled in chronic/healed state
- Air-fluid levels may be present (superimposed infection)
- Rasmussen aneurysm: Dilated vessels in cavity wall - cause of hemoptysis
- Aspergilloma (fungus ball) may colonize old cavities - "crescent sign" / air crescent sign
CT Features of Reactivation TB (HIGH YIELD)
- Tree-in-bud pattern: Centrilobular nodules with branching linear densities = bronchogenic spread (HIGHLY specific sign)
- Nodular opacities in upper lobes
- Cavities with thick or thin walls
- Air bronchograms within consolidation
- CT is superior to CXR: sensitivity 96% vs 48% for active TB
- CT better demonstrates bronchogenic spread characteristic of reactivation TB
3. MILIARY TUBERCULOSIS (10-Mark Answer)
Definition and Pathogenesis
- The term "miliary" comes from the resemblance of lesions to millet seeds
- Results from hematogenous dissemination of M. tuberculosis
- Occurs when a tuberculous focus (primary or reactivation) erodes into a blood vessel or lymphatic, seeding the entire pulmonary vasculature simultaneously
- Grossly: 1-2 mm yellowish nodules that are granulomas on histology
- Can occur in both primary and reactivation settings; more common in immunocompromised
Classic CXR Features of Miliary TB
The "snowstorm" or "millet seed" pattern:
| Feature | Details |
|---|---|
| Size | 1-3 mm nodules (size of millet seeds) |
| Distribution | Bilateral, diffuse, symmetric - all lung zones equally affected |
| Pattern | Random distribution - no zonal or bronchovascular predilection |
| Number | Innumerable (too numerous to count) |
| Margins | Well-defined, sharply marginated |
| Density | Uniform soft tissue density |
- CXR abnormal in 85-90% of miliary TB cases at diagnosis
- Classic miliary pattern seen in 50-90% of disseminated TB patients
- Nodules appear 2-3 weeks after hematogenous seeding (CXR may initially be normal!)
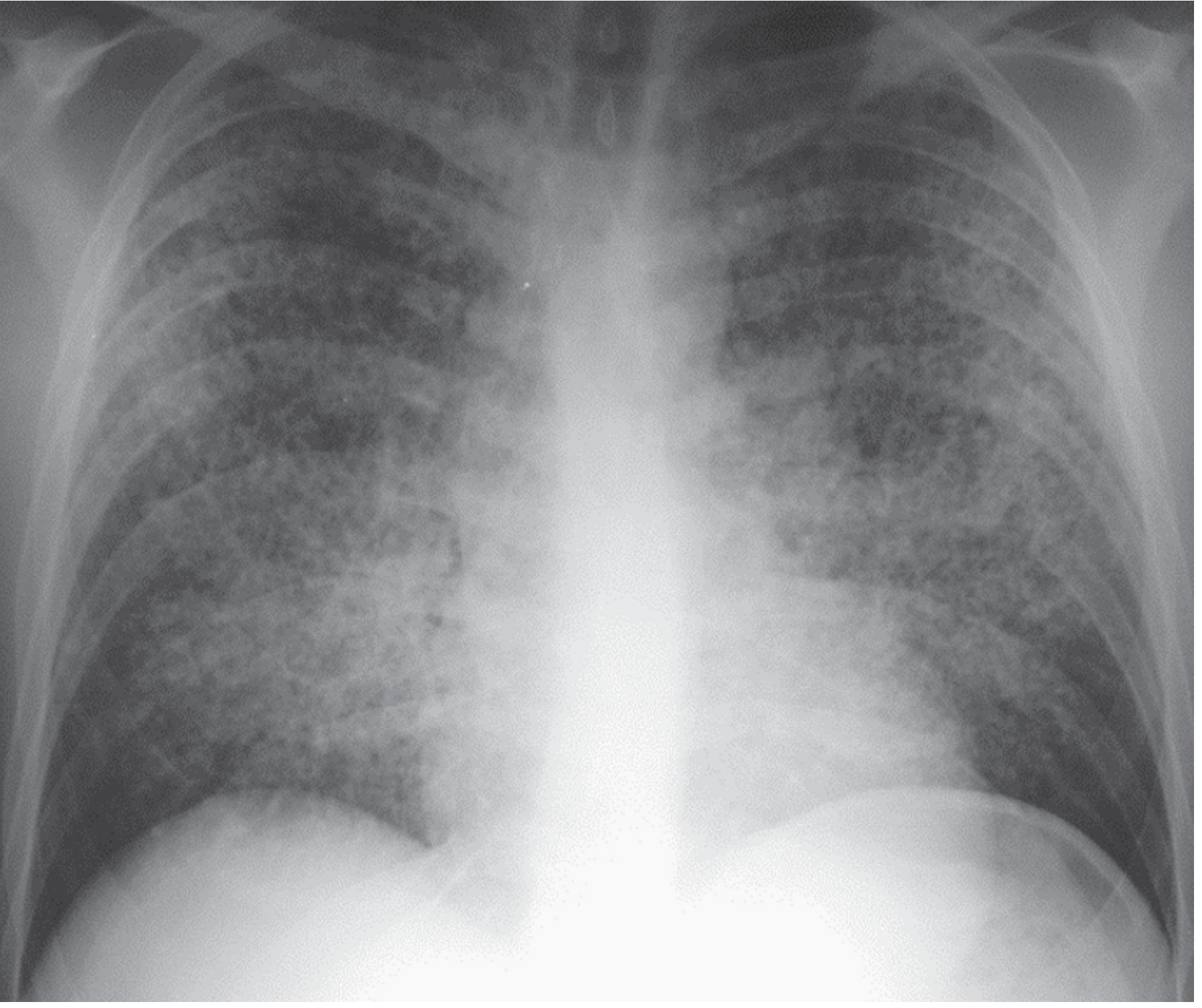
Miliary TB: Classic "snowstorm" pattern - Bilateral random nodules. Murray & Nadel eFigure 123.4
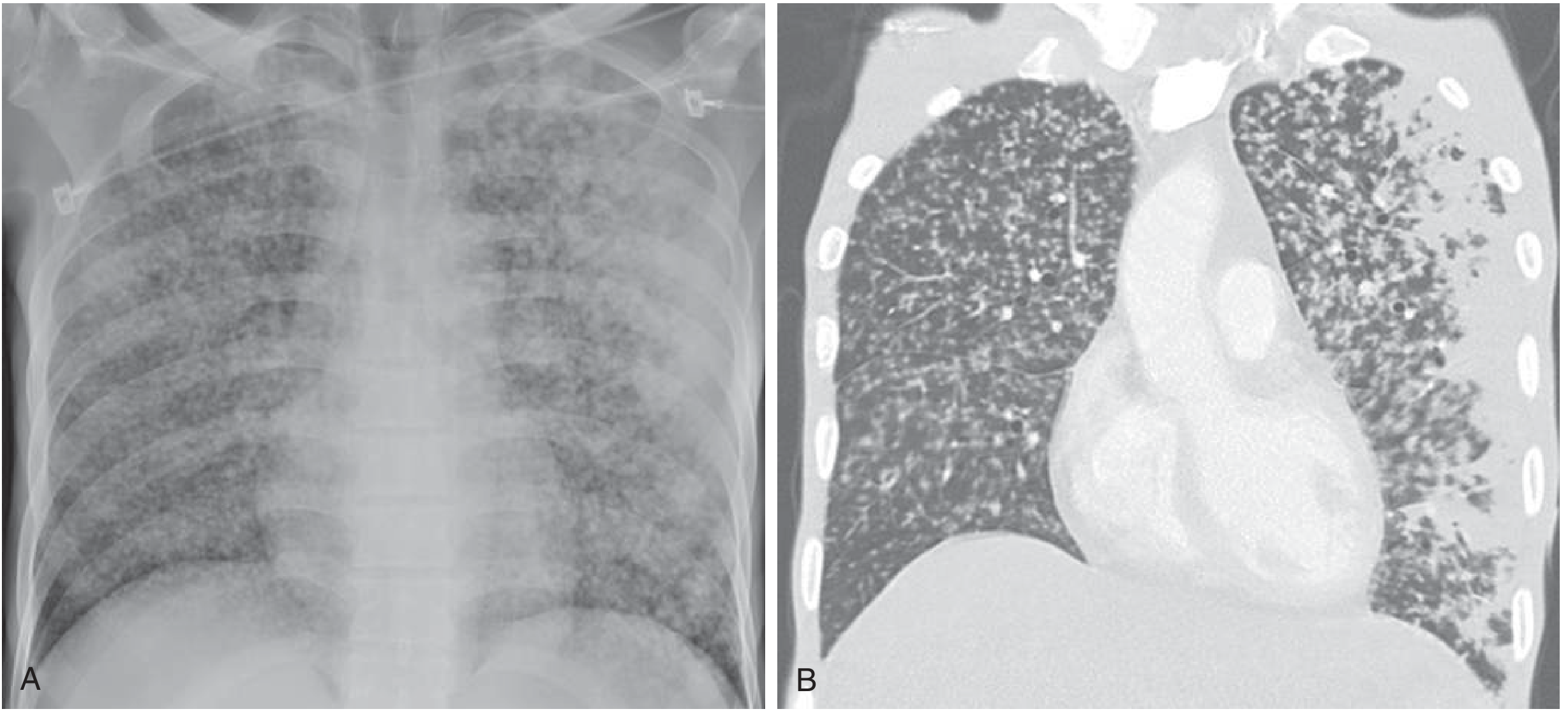
Miliary TB: (A) CXR - diffuse bilateral micronodules; (B) Coronal CT - random distribution with peripheral confluent areas. Goldman-Cecil Fig. 295-6
CT Features of Miliary TB
- Random distribution (not perilymphatic, not centrilobular) - this is the KEY CT pattern
- Nodules 1-3 mm, bilateral, diffuse
- Equal distribution in upper, middle, and lower zones
- Nodules are distributed randomly relative to secondary pulmonary lobule structures
- No zonal predilection - unlike reactivation TB which favors upper zones
- May see ground-glass opacity surrounding nodules ("halo sign")
- Additional findings: upper lobe opacities with/without cavitation, pleural effusion, pericardial effusion
CT Nodule Distribution Patterns - PG Exam Comparison Table
| Pattern | Distribution | Diseases |
|---|---|---|
| Random | Uniform, all zones | Miliary TB, hematogenous metastases, fungal infection |
| Perilymphatic | Septal/bronchovascular/subpleural | Sarcoidosis, lymphangitic carcinomatosis, pulmonary edema |
| Centrilobular | Around bronchioles, spares subpleura | Endobronchial TB (tree-in-bud), hypersensitivity pneumonitis |
Exam Tip: Miliary TB = RANDOM distribution. This is THE classic teaching point separating it from sarcoidosis (perilymphatic) and endobronchial TB (centrilobular tree-in-bud).
Atypical Presentations (in HIV/Immunosuppression)
- CXR may appear normal early in disease
- Granuloma formation is impaired; instead of discrete nodules, may show diffuse uniform opacification
- Intrathoracic lymphadenopathy more prominent (unlike immunocompetent patients)
- Cavitation less common with advanced HIV (CD4 < 200)
- Lower lobe/diffuse opacities instead of upper lobe predominance
- Pattern may resemble lobar pneumonia (Klebsiella-like appearance)
Miliary TB - Differential Diagnosis
| Condition | Key Differentiating Feature |
|---|---|
| Miliary fungal infection (histoplasma, cryptococcus) | Clinically indistinguishable; geographic history important |
| Hematogenous metastases | Known primary malignancy; nodules may be larger, non-uniform sizes |
| Sarcoidosis | Perilymphatic distribution (not random); upper lobe > lower |
| Pneumoconiosis (silicosis/CWP) | Occupational history; upper lobe predominance; egg-shell calcification of nodes |
| Langerhans cell histiocytosis | Cystic + nodular; upper > lower; spares costophrenic angles |
Organs Involved in Miliary TB (Autopsy Data)
Most frequent organs affected in order: Liver > Lungs > Bone marrow > Kidneys > Adrenal glands > Spleen (any organ can be affected)
4. TB-RELATED COMPLICATIONS - Radiological Findings
Pleural TB
- Unilateral exudative pleural effusion (lymphocyte predominant)
- Rarely bilateral; rarely large
- Empyema necessitans - TB empyema eroding through chest wall
- Bronchopleural fistula with hydropneumothorax
Endobronchial TB
- Bronchial stenosis leading to lobar/segmental atelectasis
- Obstructive pneumonitis distal to stenosis
- Air trapping on expiratory CT
Bronchogenic Spread
- Tree-in-bud pattern on CT: centrilobular branching opacities
- Ill-defined centrilobular nodules
- Patchy consolidation in dependent portions of lung
- Sign of active, highly infectious disease
Calcified Ghon Complex / Ranke Complex
- Calcified Ghon focus + calcified ipsilateral hilar node = Ranke complex
- Indicates healed primary TB
5. TB IN HIV - Radiological Spectrum (High-Yield Table)
| CD4 Count | Typical Radiological Pattern |
|---|---|
| CD4 > 350 (early HIV) | Similar to immunocompetent: upper lobe cavitation, typical reactivation pattern |
| CD4 200-350 | Mixed pattern |
| CD4 < 200 (advanced HIV) | Lower zone/diffuse opacities, lymphadenopathy, no cavitation, miliary pattern |
| CD4 < 50 | Miliary pattern, lobar consolidation mimicking bacterial pneumonia, normal CXR possible |
6. IMAGING MODALITY COMPARISON
| Modality | Role | Sensitivity for Active TB |
|---|---|---|
| CXR | Screening, initial evaluation | 48% |
| CT Chest | Characterization, bronchogenic spread, lymphadenopathy | 96% |
| MRI | Pleural assessment, caseous necrosis; pregnant/children | Comparable to CT for consolidation/adenopathy; lower for nodules |
| PET-CT | Monitoring treatment response, differentiating active vs inactive | High; increasing evidence |
QUICK-FIRE HIGH-YIELD POINTS FOR PG EXAM
- Primary TB: Lower/mid zone opacity + ipsilateral hilar adenopathy
- Reactivation TB: Apical and posterior segments of RUL (most common site)
- Anterior segment of upper lobe is spared in TB (unlike most other conditions)
- Miliary TB: 1-3 mm nodules, bilateral, symmetric, RANDOM distribution, all zones equal
- Tree-in-bud = bronchogenic spread = centrilobular distribution = active endobronchial TB
- Ranke complex = calcified Ghon focus + calcified hilar node = healed primary TB
- Rasmussen aneurysm: Dilated vessel in cavity wall - cause of massive hemoptysis
- Aspergilloma in old TB cavity: "crescent sign" (Monod sign)
- HIV + TB: More adenopathy, less cavitation, more lower zone/diffuse disease
- CXR may be normal in miliary TB for first 2-3 weeks (nodules too small)
- CT has 96% sensitivity vs 48% for CXR in active TB
- Miliary TB = RANDOM nodule pattern (differential: sarcoid = perilymphatic)
- 85-90% of miliary TB patients have abnormal CXR at diagnosis
- Snowstorm appearance on CXR = miliary TB
References: Murray & Nadel's Textbook of Respiratory Medicine; Goldman-Cecil Medicine International Edition; Harrison's Principles of Internal Medicine 22E; Fishman's Pulmonary Diseases and Disorders. Radiographic classification based on Restrepo CS et al., Radiologic Clinics of North America, 2016; 54: 453-473.
This is a shared conversation. Sign in to Orris to start your own chat.