Fatty liver disease
Reading File
Finding Sources
Searching PubMed
"nonalcoholic fatty liver disease" OR "MASLD" AND treatment
Searching the Web
MASLD NAFLD fatty liver disease 2025 guidelines treatment
Reading File
Reading File
Reading File
Loading Image
Now I have comprehensive information to provide a thorough answer. Let me compile everything:
Fatty Liver Disease (MASLD / NAFLD)
Terminology Update (2023-2026)
The field has moved away from the term NAFLD (non-alcoholic fatty liver disease). The updated nomenclature now groups conditions under Steatotic Liver Disease (SLD):
- MASLD (Metabolic dysfunction-Associated Steatotic Liver Disease) - replaces NAFLD
- MASH (Metabolic dysfunction-Associated Steatohepatitis) - replaces NASH
- MetALD - a new subcategory for MASLD patients with moderate alcohol use
- ALD (Alcohol-associated Liver Disease) remains separate
The 2024 European guidelines and 2025 AGA clinical care pathway both use this framework.
What Is It?
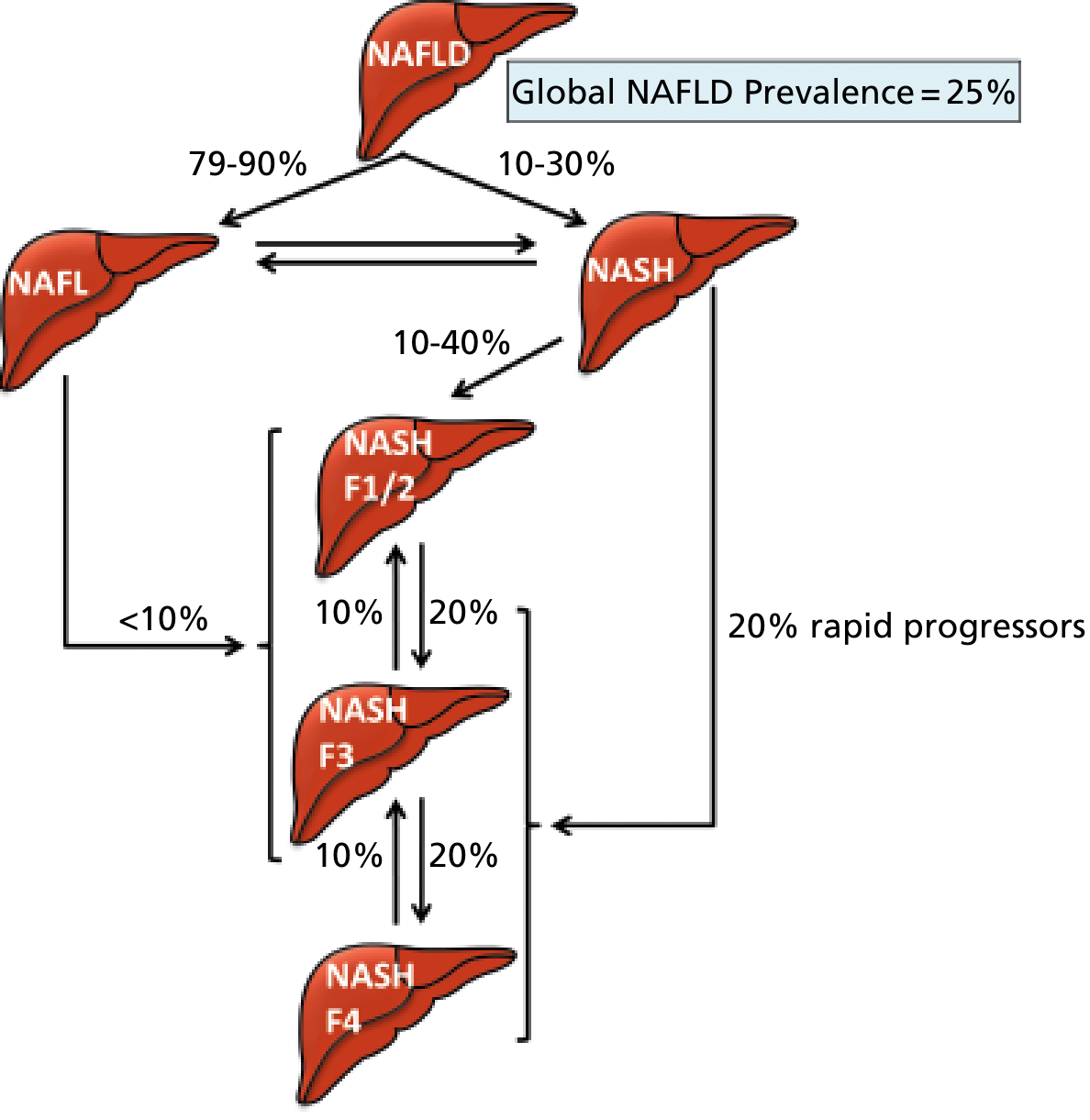
Fatty liver disease is the accumulation of fat (primarily triglycerides) in hepatocytes, affecting ≥5% of liver cells on histology or imaging. It is the most prevalent chronic liver disease globally, with a prevalence of roughly 25% worldwide.
Disease Spectrum
The spectrum ranges from simple steatosis to cirrhosis:
| Stage | Features |
|---|---|
| MASLD (steatosis only) | Fat accumulation, no significant injury; 79-90% of NAFLD |
| MASH (steatohepatitis) | Steatosis + ballooned hepatocytes + inflammation; 10-30% |
| Fibrosis F1-F3 | Progressive scarring; 10-40% of MASH progress here |
| Cirrhosis (F4) | End-stage, irreversible; ~20% are "rapid progressors" |
Key point: Fibrosis stage (not inflammation) is the primary predictor of clinical outcomes and mortality.
Pathogenesis
The central driver is insulin resistance, typically in the setting of obesity and metabolic syndrome:
- Insulin resistance - increases adipose tissue lipolysis, flooding the liver with free fatty acids (FFAs)
- Reduced adiponectin - impairs FFA oxidation in skeletal muscle, increases hepatic FFA uptake
- De novo lipogenesis - liver synthesizes more fat
- Lipotoxicity - accumulated lipids activate:
- ER stress
- Mitochondrial dysfunction
- Lysosomal dysfunction
- Reactive oxygen species (ROS) production
- Inflammasome activation (IL-1 release)
- Hepatocyte injury - ballooned hepatocytes produce sonic hedgehog, which activates hepatic stellate cells
- Fibrogenesis - stellate cell activation causes collagen deposition
- Gut dysbiosis - alterations in gut microbiome and bile acid signaling further promote inflammation
(Robbins & Kumar Basic Pathology; Yamada's Textbook of Gastroenterology)
Risk Factors / Associated Conditions
- Type 2 diabetes (or family history)
- Obesity, especially central/abdominal obesity
- Dyslipidemia (high triglycerides, low HDL, high LDL)
- Hypertension
- Metabolic syndrome
- Genetic factors: PNPLA3 rs738409 C>G polymorphism increases HCC risk
Clinical Features
- Most patients are asymptomatic - MASLD is the most common cause of incidentally elevated serum transaminases
- AST:ALT ratio < 1 (contrast with alcoholic liver disease where ratio is typically >2)
- When symptomatic: fatigue, malaise, right upper quadrant discomfort
- Advanced disease: features of chronic liver disease (jaundice, ascites, varices)
- Cardiovascular disease is the leading cause of death in MASLD (shared risk factors)
- In patients with MASH/cirrhosis, liver-related mortality exceeds cardiovascular mortality
Diagnosis
- Imaging (ultrasound, MRI, CT) can detect steatosis but cannot reliably grade inflammation or fibrosis
- Liver biopsy remains the gold standard for:
- Confirming MASH diagnosis
- Assessing fibrosis stage
- Distinguishing MASLD from other liver diseases
- Resolving discrepancies between non-invasive tests
- Non-invasive tests: FIB-4 score, liver stiffness measurement (elastography), MRI-PDFF for steatosis quantification
- The 2026 Japanese guidelines and 2024 European guidelines both confirm biopsy is NOT routinely required for simple steatosis diagnosis, but is essential for "at-risk MASH" assessment
Complications
- Cirrhosis - the endpoint of progressive fibrosis
- Hepatocellular carcinoma (HCC) - NAFLD/MASLD is the 3rd most common cause of HCC; incidence in MASLD-cirrhosis is ~10.9 per 1,000 person-years. As hepatitis C is successfully treated, MASLD is projected to become the leading cause of HCC in the US
- Cardiovascular disease - independent risk factor
- Pediatric MASLD - increasingly prevalent; histologically distinct (portal-predominant inflammation and fibrosis, mononuclear rather than neutrophilic infiltrates)
Treatment
Lifestyle (First-Line, Most Effective)
- ≥5% body weight loss: improves steatosis, ballooning, and inflammation
- 5-10% loss: reduces inflammation
- ≥10% loss: can reverse fibrosis
- Exercise and dietary modification are the cornerstones
- Bariatric surgery for eligible patients - proven to improve MASH histology
Pharmacotherapy (Recent Approvals)
| Drug | Mechanism | Status |
|---|---|---|
| Resmetirom (Rezdiffra) | Selective thyroid hormone receptor-β agonist | FDA-approved (2024) - first approved drug for MASH with fibrosis |
| Semaglutide (GLP-1 RA) | GLP-1 receptor agonist | AASLD Nov 2025 update recommends for MASH; strong evidence for fibrosis regression |
| Other GLP-1/GIP agonists | Incretin mimetics | In trials |
| FXR agonists, ACC inhibitors, ASK1 inhibitors | Various metabolic targets | Phase II/III trials |
Recent evidence update: A 2025 network meta-analysis (PMID 39903735) comparing pharmacological therapies for MASH found significant differences in fibrosis regression and MASH resolution rates across drug classes. A 2024 systematic review (PMID 39187533) confirmed resmetirom's efficacy and safety. The AASLD also issued a November 2025 guidance specifically on semaglutide for MASH.
Alcohol
The 2024 European guidelines recommend no alcohol intake in MASLD patients (previously, light drinking was considered acceptable).
Cardiovascular Risk Management
Given CVD is the top cause of death in MASLD, management of hypertension, dyslipidemia, and diabetes is an integral part of care - not just liver-focused therapy.
Summary
MASLD is a spectrum from simple steatosis to cirrhosis, driven by insulin resistance and metabolic dysfunction. Fibrosis stage determines prognosis. Weight loss remains the cornerstone of therapy, but the field now has its first FDA-approved drug (resmetirom) and strong evidence for semaglutide in MASH. Early identification of patients at risk for advanced fibrosis using non-invasive tools is the key clinical priority.
- Robbins & Kumar Basic Pathology, p. 1910-1926
- Yamada's Textbook of Gastroenterology, 7th ed., p. 2230
- 2024 European MASLD Clinical Practice Guidelines
- AASLD 2025 Practice Guidance (semaglutide update)
For biochemistry seminar PPT
Asking for Preferences
MBBS 1st year
Reading File
Reading File
Reading File
Running Command
mkdir -p /home/daytona/workspace/fatty-liver-ppt && ls /home/daytona/workspace/fatty-liver-ppt/
Writing File
~/fatty-liver-ppt/create_ppt.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Fatty Liver Disease";
pres.author = "Biochemistry Seminar";
// ─── PALETTE ───────────────────────────────────────────────────────────────
const C = {
navy: "0D2B45", // dominant dark bg
teal: "0A7E8C", // accent headers
amber: "F4A836", // highlights / accent
cream: "FDF6EC", // light bg
white: "FFFFFF",
ltGray: "E8EFF5",
midGray: "7A91A8",
red: "C0392B",
green: "27AE60",
};
// ─── HELPERS ───────────────────────────────────────────────────────────────
function titleBar(slide, title, subtitle) {
// dark left strip
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 0.18, h: 5.625,
fill: { color: C.teal }, line: { color: C.teal }
});
slide.addText(title, {
x: 0.35, y: 0.18, w: 9.3, h: 0.7,
fontSize: 26, bold: true, color: C.navy, fontFace: "Calibri",
margin: 0
});
// amber underline
slide.addShape(pres.shapes.RECTANGLE, {
x: 0.35, y: 0.92, w: 9.3, h: 0.04,
fill: { color: C.amber }, line: { color: C.amber }
});
if (subtitle) {
slide.addText(subtitle, {
x: 0.35, y: 0.98, w: 9.3, h: 0.38,
fontSize: 13, color: C.midGray, fontFace: "Calibri", italic: true, margin: 0
});
}
}
function bodyBox(slide, items, x, y, w, h, opts = {}) {
const fontSize = opts.fontSize || 15;
const color = opts.color || C.navy;
slide.addText(
items.map((t, i) => ({
text: t,
options: { bullet: true, breakLine: i < items.length - 1 }
})),
{ x, y, w, h, fontSize, color, fontFace: "Calibri",
paraSpaceBefore: 4, paraSpaceAfter: 2, lineSpacingMultiple: 1.15 }
);
}
function card(slide, x, y, w, h, fillColor, text, textColor, fontSize) {
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w, h,
fill: { color: fillColor },
line: { color: fillColor },
rectRadius: 0.12,
shadow: { type: "outer", color: "000000", blur: 6, offset: 3, angle: 135, opacity: 0.12 }
});
slide.addText(text, {
x: x + 0.08, y, w: w - 0.16, h,
fontSize: fontSize || 13, color: textColor || C.white,
fontFace: "Calibri", bold: true, align: "center", valign: "middle", margin: 0
});
}
function arrow(slide, x, y, w) {
slide.addShape(pres.shapes.RIGHT_ARROW, {
x, y, w, h: 0.32,
fill: { color: C.amber }, line: { color: C.amber }
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 1 – TITLE
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
// full navy background
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 5.625,
fill: { color: C.navy }, line: { color: C.navy }
});
// teal accent bar left
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 0.35, h: 5.625,
fill: { color: C.teal }, line: { color: C.teal }
});
// amber line
s.addShape(pres.shapes.RECTANGLE, {
x: 0.55, y: 2.62, w: 5.2, h: 0.06,
fill: { color: C.amber }, line: { color: C.amber }
});
s.addText("FATTY LIVER DISEASE", {
x: 0.55, y: 1.0, w: 8.8, h: 1.2,
fontSize: 44, bold: true, color: C.white, fontFace: "Calibri",
charSpacing: 3, margin: 0
});
s.addText("Biochemistry Seminar | MBBS 1st Year", {
x: 0.55, y: 2.72, w: 8.8, h: 0.5,
fontSize: 18, color: C.amber, fontFace: "Calibri", margin: 0
});
s.addText("Hepatic Steatosis • MASLD • Pathogenesis • Clinical Correlates", {
x: 0.55, y: 3.28, w: 8.8, h: 0.45,
fontSize: 14, color: C.midGray, fontFace: "Calibri", italic: true, margin: 0
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 2 – OUTLINE
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:10,h:5.625, fill:{color:C.cream}, line:{color:C.cream} });
titleBar(s, "Seminar Outline", "What we will cover today");
const topics = [
["1", "Definition & Introduction"],
["2", "Epidemiology"],
["3", "Types of Fatty Liver Disease"],
["4", "Normal Lipid Metabolism in the Liver"],
["5", "Pathogenesis & Biochemical Mechanisms"],
["6", "Risk Factors & Associated Conditions"],
["7", "Clinical Features & Diagnosis"],
["8", "Complications"],
["9", "Treatment & Management"],
["10", "Summary & Key Points"],
];
const col1 = topics.slice(0, 5);
const col2 = topics.slice(5);
col1.forEach(([num, text], i) => {
const y = 1.5 + i * 0.72;
slide_numberChip(s, num, 0.45, y);
s.addText(text, { x: 1.1, y, w: 3.8, h: 0.55, fontSize: 14.5, color: C.navy, fontFace: "Calibri", valign: "middle", margin: 0 });
});
col2.forEach(([num, text], i) => {
const y = 1.5 + i * 0.72;
slide_numberChip(s, num, 5.2, y);
s.addText(text, { x: 5.85, y, w: 3.8, h: 0.55, fontSize: 14.5, color: C.navy, fontFace: "Calibri", valign: "middle", margin: 0 });
});
}
function slide_numberChip(s, num, x, y) {
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y: y + 0.08, w: 0.5, h: 0.38,
fill: { color: C.teal }, line: { color: C.teal }, rectRadius: 0.08
});
s.addText(num, { x, y: y + 0.08, w: 0.5, h: 0.38, fontSize: 13, bold: true, color: C.white, fontFace: "Calibri", align: "center", valign: "middle", margin: 0 });
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 3 – DEFINITION
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:10,h:5.625, fill:{color:C.cream}, line:{color:C.cream} });
titleBar(s, "Definition", "What is Fatty Liver Disease?");
// big definition card
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.45, y: 1.45, w: 9.1, h: 1.35,
fill: { color: C.navy }, line: { color: C.navy }, rectRadius: 0.15,
shadow: { type: "outer", color: "000000", blur: 8, offset: 3, angle: 135, opacity: 0.18 }
});
s.addText([
{ text: "Fatty liver disease", options: { bold: true, color: C.amber } },
{ text: " (hepatic steatosis) is the abnormal accumulation of ", options: { color: C.white } },
{ text: "triglycerides", options: { bold: true, color: C.amber } },
{ text: " within hepatocytes, defined histologically as fat in ", options: { color: C.white } },
{ text: "≥5%", options: { bold: true, color: C.amber } },
{ text: " of liver cells.", options: { color: C.white } },
], { x: 0.65, y: 1.5, w: 8.7, h: 1.25, fontSize: 17, fontFace: "Calibri", valign: "middle", margin: 6 });
// 3 key fact chips
const facts = [
{ label: "Global Prevalence", val: "~25%" },
{ label: "Most Common Cause of", val: "Elevated ALT/AST" },
{ label: "Reversible with", val: "Weight Loss" },
];
facts.forEach((f, i) => {
const x = 0.45 + i * 3.1;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y: 3.05, w: 2.9, h: 1.8,
fill: { color: C.ltGray }, line: { color: C.teal, pt: 1.5 }, rectRadius: 0.12,
shadow: { type: "outer", color: "000000", blur: 4, offset: 2, angle: 135, opacity: 0.1 }
});
s.addText(f.val, { x, y: 3.1, w: 2.9, h: 0.88, fontSize: 22, bold: true, color: C.teal, fontFace: "Calibri", align: "center", valign: "middle", margin: 0 });
s.addText(f.label, { x, y: 3.98, w: 2.9, h: 0.72, fontSize: 12, color: C.navy, fontFace: "Calibri", align: "center", valign: "middle", margin: 0 });
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 4 – TYPES
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:10,h:5.625, fill:{color:C.cream}, line:{color:C.cream} });
titleBar(s, "Types of Fatty Liver Disease", "Modern Classification (2023 Nomenclature)");
// SLD umbrella box
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 2.8, y: 1.35, w: 4.4, h: 0.72,
fill: { color: C.navy }, line: { color: C.navy }, rectRadius: 0.1
});
s.addText("Steatotic Liver Disease (SLD)", { x: 2.8, y: 1.35, w: 4.4, h: 0.72, fontSize: 15, bold: true, color: C.white, fontFace: "Calibri", align: "center", valign: "middle", margin: 0 });
// branches
const types = [
{ label: "MASLD", sub: "Metabolic dysfunction-\nAssociated Steatotic\nLiver Disease\n(replaces NAFLD)", x: 0.3, color: C.teal },
{ label: "MetALD", sub: "MASLD + moderate\nalcohol use\n(new subcategory)", x: 3.1, color: C.amber },
{ label: "ALD", sub: "Alcohol-Associated\nLiver Disease\n(>20g/day women;\n>30g/day men)", x: 5.9, color: "#C0392B" },
{ label: "Other SLD", sub: "Drug-induced,\ngenetic, cryptogenic\ncauses", x: 7.5, color: C.midGray },
];
types.forEach(t => {
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: t.x, y: 2.35, w: 2.1, h: 2.85,
fill: { color: C.white },
line: { color: t.color, pt: 2.5 }, rectRadius: 0.12,
shadow: { type: "outer", color: "000000", blur: 5, offset: 2, angle: 135, opacity: 0.1 }
});
s.addShape(pres.shapes.RECTANGLE, {
x: t.x, y: 2.35, w: 2.1, h: 0.5,
fill: { color: t.color }, line: { color: t.color }
});
s.addText(t.label, { x: t.x, y: 2.35, w: 2.1, h: 0.5, fontSize: 14, bold: true, color: C.white, fontFace: "Calibri", align: "center", valign: "middle", margin: 0 });
s.addText(t.sub, { x: t.x + 0.1, y: 2.9, w: 1.9, h: 2.1, fontSize: 11.5, color: C.navy, fontFace: "Calibri", align: "center", valign: "top", margin: 4 });
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 5 – NORMAL LIPID METABOLISM
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:10,h:5.625, fill:{color:C.cream}, line:{color:C.cream} });
titleBar(s, "Normal Lipid Metabolism in the Liver", "Understanding the baseline before disease");
// flow boxes
const steps = [
{ label: "Dietary Fats\n(Chylomicrons)", color: C.teal },
{ label: "Fatty Acids\nfrom Adipose", color: C.teal },
{ label: "HEPATOCYTE\nFatty Acid Uptake", color: C.navy },
{ label: "β-Oxidation\n(Mitochondria)", color: C.green },
{ label: "VLDL Synthesis\n& Export", color: C.amber },
{ label: "Ketone Body\nProduction", color: "#8E44AD" },
];
// row 1: inputs → hepatocyte
[[0,1.45,2.05], [0,3.25,2.05]].forEach(([i, x]) => {});
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.35, y: 1.52, w: 2.2, h: 0.9, fill:{color:C.teal}, line:{color:C.teal}, rectRadius:0.1 });
s.addText("Dietary Fats\n(Chylomicrons)", { x:0.35,y:1.52,w:2.2,h:0.9, fontSize:12, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.35, y: 2.8, w: 2.2, h: 0.9, fill:{color:C.teal}, line:{color:C.teal}, rectRadius:0.1 });
s.addText("Free Fatty Acids\nfrom Adipose", { x:0.35,y:2.8,w:2.2,h:0.9, fontSize:12, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.35, y: 4.1, w: 2.2, h: 0.9, fill:{color:C.teal}, line:{color:C.teal}, rectRadius:0.1 });
s.addText("De Novo\nLipogenesis", { x:0.35,y:4.1,w:2.2,h:0.9, fontSize:12, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
// arrows → hepatocyte
s.addShape(pres.shapes.RIGHT_ARROW, { x:2.6,y:1.82,w:0.7,h:0.3, fill:{color:C.amber}, line:{color:C.amber} });
s.addShape(pres.shapes.RIGHT_ARROW, { x:2.6,y:3.1,w:0.7,h:0.3, fill:{color:C.amber}, line:{color:C.amber} });
s.addShape(pres.shapes.RIGHT_ARROW, { x:2.6,y:4.4,w:0.7,h:0.3, fill:{color:C.amber}, line:{color:C.amber} });
// hepatocyte central box
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:3.35, y:1.45, w:2.6, h:3.6, fill:{color:C.navy}, line:{color:C.navy}, rectRadius:0.15, shadow:{type:"outer",color:"000000",blur:8,offset:3,angle:135,opacity:0.2} });
s.addText("HEPATOCYTE", { x:3.35,y:1.5,w:2.6,h:0.52, fontSize:14, bold:true, color:C.amber, fontFace:"Calibri", align:"center", valign:"middle", margin:0, charSpacing:2 });
s.addText([
{ text: "• Fatty acid uptake (FATP, CD36)", options:{breakLine:true} },
{ text: "• Esterification → Triglycerides", options:{breakLine:true} },
{ text: "• β-Oxidation (ATP production)", options:{breakLine:true} },
{ text: "• VLDL assembly & secretion", options:{breakLine:true} },
{ text: "• Ketogenesis (fasting)", options:{breakLine:false} },
], { x:3.45,y:2.08,w:2.4,h:2.85, fontSize:11.5, color:C.white, fontFace:"Calibri", lineSpacingMultiple:1.25, margin:4 });
// output arrows
s.addShape(pres.shapes.RIGHT_ARROW, { x:6.0,y:1.82,w:0.65,h:0.3, fill:{color:C.amber}, line:{color:C.amber} });
s.addShape(pres.shapes.RIGHT_ARROW, { x:6.0,y:3.1,w:0.65,h:0.3, fill:{color:C.amber}, line:{color:C.amber} });
s.addShape(pres.shapes.RIGHT_ARROW, { x:6.0,y:4.4,w:0.65,h:0.3, fill:{color:C.amber}, line:{color:C.amber} });
// outputs
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:6.7,y:1.52,w:2.8,h:0.9, fill:{color:C.green}, line:{color:C.green}, rectRadius:0.1 });
s.addText("VLDL Export\n(to blood)", { x:6.7,y:1.52,w:2.8,h:0.9, fontSize:12, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:6.7,y:2.8,w:2.8,h:0.9, fill:{color:C.green}, line:{color:C.green}, rectRadius:0.1 });
s.addText("ATP via\nβ-Oxidation", { x:6.7,y:2.8,w:2.8,h:0.9, fontSize:12, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:6.7,y:4.1,w:2.8,h:0.9, fill:{color:"8E44AD"}, line:{color:"8E44AD"}, rectRadius:0.1 });
s.addText("Ketone Bodies\n(fasting state)", { x:6.7,y:4.1,w:2.8,h:0.9, fontSize:12, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 6 – PATHOGENESIS (Two-Hit Model)
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:10,h:5.625, fill:{color:C.cream}, line:{color:C.cream} });
titleBar(s, "Pathogenesis: The 'Two-Hit' Model", "How fatty liver progresses to steatohepatitis");
// HIT 1
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:0.35,y:1.38,w:4.35,h:3.82, fill:{color:C.white}, line:{color:C.teal,pt:2}, rectRadius:0.15, shadow:{type:"outer",color:"000000",blur:5,offset:2,angle:135,opacity:0.1} });
s.addShape(pres.shapes.RECTANGLE, { x:0.35,y:1.38,w:4.35,h:0.55, fill:{color:C.teal}, line:{color:C.teal} });
s.addText("HIT 1 — Steatosis", { x:0.35,y:1.38,w:4.35,h:0.55, fontSize:15, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
bodyBox(s, [
"Obesity + Insulin Resistance",
"↑ Adipose lipolysis → more FFAs to liver",
"↓ Adiponectin → ↓ FFA oxidation",
"↑ De novo lipogenesis in hepatocytes",
"↓ VLDL export capacity",
"Triglycerides accumulate → STEATOSIS",
], 0.55, 2.0, 4.0, 3.1, { fontSize: 13.5 });
// arrow between hits
s.addShape(pres.shapes.RIGHT_ARROW, { x:4.78,y:2.9,w:0.56,h:0.42, fill:{color:C.amber}, line:{color:C.amber} });
// HIT 2
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:5.38,y:1.38,w:4.28,h:3.82, fill:{color:C.white}, line:{color:C.red,pt:2}, rectRadius:0.15, shadow:{type:"outer",color:"000000",blur:5,offset:2,angle:135,opacity:0.1} });
s.addShape(pres.shapes.RECTANGLE, { x:5.38,y:1.38,w:4.28,h:0.55, fill:{color:C.red}, line:{color:C.red} });
s.addText("HIT 2 — Inflammation & Injury", { x:5.38,y:1.38,w:4.28,h:0.55, fontSize:15, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
bodyBox(s, [
"Lipotoxicity (palmitate, lysophosphatidylcholine)",
"↑ Reactive Oxygen Species (ROS)",
"ER stress & mitochondrial dysfunction",
"Inflammasome activation → IL-1β release",
"Gut dysbiosis → ↑ endotoxin (LPS)",
"Stellate cell activation → FIBROSIS",
], 5.55, 2.0, 3.95, 3.1, { fontSize: 13.5 });
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 7 – BIOCHEMICAL MECHANISMS (detailed)
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:10,h:5.625, fill:{color:C.cream}, line:{color:C.cream} });
titleBar(s, "Biochemical Mechanisms", "Key molecular pathways in MASLD");
const mechs = [
{ title: "Insulin Resistance", color: C.teal, points: ["↓ IRS-1/IRS-2 signaling", "↑ SREBP-1c → fatty acid synthesis", "↑ ChREBP → glycolysis & lipogenesis"] },
{ title: "Lipid Accumulation", color: C.amber, points: ["↑ FFA influx (CD36 upregulated)", "↑ ACC & FAS enzyme activity", "↓ CPT-1 → less β-oxidation"] },
{ title: "Oxidative Stress", color: C.red, points: ["↑ CYP2E1 activity", "Mitochondrial ETC uncoupling", "↑ ROS → lipid peroxidation (4-HNE, MDA)"] },
{ title: "Inflammation", color: "#8E44AD", points: ["NLRP3 inflammasome → IL-1β, IL-18", "TLR4 activation by LPS", "TNF-α, TGF-β → fibrosis"] },
];
mechs.forEach((m, i) => {
const col = i % 2;
const row = Math.floor(i / 2);
const x = 0.35 + col * 4.85;
const y = 1.35 + row * 2.05;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x, y, w: 4.6, h: 1.88, fill:{color:C.white}, line:{color:m.color, pt:2}, rectRadius:0.12, shadow:{type:"outer",color:"000000",blur:4,offset:2,angle:135,opacity:0.1} });
s.addShape(pres.shapes.RECTANGLE, { x, y, w: 4.6, h: 0.48, fill:{color:m.color}, line:{color:m.color} });
s.addText(m.title, { x, y, w:4.6, h:0.48, fontSize:14, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
bodyBox(s, m.points, x+0.15, y+0.52, 4.3, 1.3, { fontSize: 12.5 });
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 8 – RISK FACTORS
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:10,h:5.625, fill:{color:C.cream}, line:{color:C.cream} });
titleBar(s, "Risk Factors & Associated Conditions", "The metabolic syndrome connection");
const risks = [
{ icon: "🏋", label: "Obesity", detail: "BMI >25; especially\ncentral/abdominal\nobesity (↑ visceral fat)", color: C.teal },
{ icon: "💉", label: "Type 2 Diabetes", detail: "Insulin resistance\nis the central\nmolecular driver", color: C.amber },
{ icon: "🫀", label: "Dyslipidemia", detail: "↑ Triglycerides\n↓ HDL cholesterol\n↑ LDL cholesterol", color: C.red },
{ icon: "🩺", label: "Hypertension", detail: "Part of metabolic\nsyndrome; shared\nCVD risk", color: "#8E44AD" },
{ icon: "🧬", label: "Genetics", detail: "PNPLA3 I148M\nTM6SF2 E167K\nHSD17B13 variants", color: "#27AE60" },
{ icon: "🍺", label: "Alcohol (MetALD)", detail: "Moderate alcohol\nuse creates mixed\nMetALD category", color: C.midGray },
];
risks.forEach((r, i) => {
const col = i % 3;
const row = Math.floor(i / 3);
const x = 0.38 + col * 3.22;
const y = 1.38 + row * 2.05;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x, y, w:3.02, h:1.88, fill:{color:C.white}, line:{color:r.color, pt:2}, rectRadius:0.12, shadow:{type:"outer",color:"000000",blur:4,offset:2,angle:135,opacity:0.1} });
s.addShape(pres.shapes.RECTANGLE, { x, y, w:3.02, h:0.5, fill:{color:r.color}, line:{color:r.color} });
s.addText(r.label, { x, y, w:3.02, h:0.5, fontSize:13.5, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
s.addText(r.detail, { x:x+0.1, y:y+0.54, w:2.82, h:1.28, fontSize:12, color:C.navy, fontFace:"Calibri", align:"center", valign:"top", margin:2 });
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 9 – DISEASE SPECTRUM / PROGRESSION
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:10,h:5.625, fill:{color:C.cream}, line:{color:C.cream} });
titleBar(s, "Disease Spectrum & Progression", "From steatosis to cirrhosis — fibrosis stage determines prognosis");
// spectrum arrow bar
s.addShape(pres.shapes.RECTANGLE, { x:0.38,y:2.55,w:9.25,h:0.55, fill:{color:C.ltGray}, line:{color:C.ltGray} });
s.addShape(pres.shapes.RIGHT_ARROW, { x:9.0,y:2.55,w:0.6,h:0.55, fill:{color:C.navy}, line:{color:C.navy} });
const stages = [
{ label: "Steatosis\n(MASLD)", sub: "Fat ≥5%\nNo inflammation\n79–90%", color: C.teal, x: 0.38 },
{ label: "Steato-\nhepatitis\n(MASH)", sub: "Steatosis +\nBallooning +\nInflammation\n10–30%", color: C.amber, x: 2.72 },
{ label: "Fibrosis\nF1-F2", sub: "Perisinusoidal\nor periportal\nscarring", color: "#E67E22", x: 5.05 },
{ label: "Fibrosis\nF3", sub: "Bridging\nfibrosis\n(serious)", color: C.red, x: 7.0 },
{ label: "Cirrhosis\nF4", sub: "Irreversible\n↑ HCC risk\n(20% rapid)", color: "#8B0000", x: 8.55 },
];
stages.forEach(st => {
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:st.x, y:1.35, w:2.1, h:1.15, fill:{color:st.color}, line:{color:st.color}, rectRadius:0.1 });
s.addText(st.label, { x:st.x, y:1.35, w:2.1, h:1.15, fontSize:12.5, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:2 });
s.addText(st.sub, { x:st.x, y:3.16, w:2.1, h:1.6, fontSize:11.5, color:C.navy, fontFace:"Calibri", align:"center", valign:"top", margin:2 });
// connector lines
s.addShape(pres.shapes.RECTANGLE, { x:st.x+0.95, y:2.5, w:0.2, h:0.1, fill:{color:st.color}, line:{color:st.color} });
});
// "Reversible" label
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:0.38,y:4.88,w:4.0,h:0.42, fill:{color:C.green}, line:{color:C.green}, rectRadius:0.08 });
s.addText("✓ Potentially Reversible with Weight Loss / Treatment", { x:0.38,y:4.88,w:4.0,h:0.42, fontSize:11.5, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:5.82,y:4.88,w:3.82,h:0.42, fill:{color:C.red}, line:{color:C.red}, rectRadius:0.08 });
s.addText("✗ Progressive Fibrosis → Cirrhosis if untreated", { x:5.82,y:4.88,w:3.82,h:0.42, fontSize:11.5, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 10 – CLINICAL FEATURES & DIAGNOSIS
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:10,h:5.625, fill:{color:C.cream}, line:{color:C.cream} });
titleBar(s, "Clinical Features & Diagnosis", "Recognition and workup in clinical practice");
// Left: clinical features
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:0.35,y:1.38,w:4.45,h:3.82, fill:{color:C.white}, line:{color:C.teal,pt:2}, rectRadius:0.15, shadow:{type:"outer",color:"000000",blur:5,offset:2,angle:135,opacity:0.1} });
s.addShape(pres.shapes.RECTANGLE, { x:0.35,y:1.38,w:4.45,h:0.52, fill:{color:C.teal}, line:{color:C.teal} });
s.addText("Clinical Features", { x:0.35,y:1.38,w:4.45,h:0.52, fontSize:14.5, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
bodyBox(s, [
"Most patients are ASYMPTOMATIC",
"Incidental ↑ ALT/AST on blood test",
"AST:ALT ratio < 1 (cf. ALD where >2)",
"Fatigue, malaise (if active MASH)",
"RUQ discomfort (hepatomegaly)",
"Advanced: jaundice, ascites, varices",
"Acanthosis nigricans (insulin resistance)",
], 0.55, 1.95, 4.1, 3.22, { fontSize: 13 });
// Right: Diagnosis
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:5.22,y:1.38,w:4.45,h:3.82, fill:{color:C.white}, line:{color:C.amber,pt:2}, rectRadius:0.15, shadow:{type:"outer",color:"000000",blur:5,offset:2,angle:135,opacity:0.1} });
s.addShape(pres.shapes.RECTANGLE, { x:5.22,y:1.38,w:4.45,h:0.52, fill:{color:C.amber}, line:{color:C.amber} });
s.addText("Diagnosis", { x:5.22,y:1.38,w:4.45,h:0.52, fontSize:14.5, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
bodyBox(s, [
"Bloods: LFTs, fasting lipids, HbA1c, glucose",
"FIB-4 score (non-invasive fibrosis marker)",
"Ultrasound: bright echogenic liver (steatosis)",
"MRI-PDFF: quantifies fat accurately",
"Liver Elastography (FibroScan): stiffness",
"Liver Biopsy: gold standard for MASH/fibrosis",
"Exclude: viral hepatitis, autoimmune, Wilson's",
], 5.4, 1.95, 4.1, 3.22, { fontSize: 13 });
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 11 – COMPLICATIONS
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:10,h:5.625, fill:{color:C.cream}, line:{color:C.cream} });
titleBar(s, "Complications", "Why fatty liver disease matters");
const comps = [
{ title: "Cirrhosis", body: "End-stage fibrosis. Portal hypertension, ascites, variceal bleeding, hepatic encephalopathy.", color: C.red },
{ title: "Hepatocellular\nCarcinoma (HCC)", body: "3rd most common cause of HCC. Risk even before cirrhosis in MASH. Projected to surpass HCV-related HCC.", color: "#8B0000" },
{ title: "Cardiovascular\nDisease", body: "#1 cause of death in MASLD. Shared risk factors with metabolic syndrome. Independent CVD risk.", color: C.amber },
{ title: "Type 2 Diabetes\n& Worsening\nMetabolic Syndrome", body: "Bidirectional relationship: insulin resistance drives MASLD; MASLD worsens insulin resistance.", color: "#8E44AD" },
];
comps.forEach((c, i) => {
const col = i % 2;
const row = Math.floor(i / 2);
const x = 0.35 + col * 4.85;
const y = 1.35 + row * 2.05;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x, y, w:4.6, h:1.9, fill:{color:C.white}, line:{color:c.color, pt:2.5}, rectRadius:0.12, shadow:{type:"outer",color:"000000",blur:4,offset:2,angle:135,opacity:0.12} });
s.addShape(pres.shapes.RECTANGLE, { x, y, w:4.6, h:0.5, fill:{color:c.color}, line:{color:c.color} });
s.addText(c.title, { x, y, w:4.6, h:0.5, fontSize:13.5, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
s.addText(c.body, { x:x+0.12, y:y+0.55, w:4.36, h:1.28, fontSize:12.5, color:C.navy, fontFace:"Calibri", valign:"top", margin:3 });
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 12 – TREATMENT & MANAGEMENT
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:10,h:5.625, fill:{color:C.cream}, line:{color:C.cream} });
titleBar(s, "Treatment & Management", "Lifestyle first, pharmacotherapy emerging");
// pyramid-style hierarchy
// Base: Lifestyle
s.addShape(pres.shapes.RECTANGLE, { x:0.35,y:1.38,w:9.3,h:1.0, fill:{color:C.teal}, line:{color:C.teal}, shadow:{type:"outer",color:"000000",blur:4,offset:2,angle:135,opacity:0.1} });
s.addText("1st Line: Lifestyle Modification (Cornerstone of All Stages)", { x:0.35,y:1.38,w:9.3,h:0.42, fontSize:15, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
s.addText("≥5% weight loss → ↓ steatosis | 5–10% → ↓ inflammation | ≥10% → fibrosis reversal | Mediterranean diet + regular aerobic exercise", { x:0.35,y:1.8,w:9.3,h:0.52, fontSize:12.5, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
// Tier 2: Pharmacotherapy
s.addShape(pres.shapes.RECTANGLE, { x:0.35,y:2.45,w:9.3,h:1.58, fill:{color:C.ltGray}, line:{color:C.amber, pt:2} });
s.addText("2nd Line: Pharmacotherapy (For At-Risk MASH with Fibrosis)", { x:0.45,y:2.5,w:9.0,h:0.42, fontSize:14, bold:true, color:C.navy, fontFace:"Calibri", align:"left", valign:"middle", margin:0 });
const drugs = [
{ name: "Resmetirom\n(Rezdiffra)", mech: "THR-β agonist", note: "FDA approved 2024\nFirst approved drug for MASH", color: C.green },
{ name: "Semaglutide\n(Ozempic/Wegovy)", mech: "GLP-1 receptor agonist", note: "AASLD 2025 guidance\nFibrosis regression + weight loss", color: "#27AE60" },
{ name: "GLP-1/GIP\nAgonists", mech: "Tirzepatide etc.", note: "Phase III trials\nPromising data", color: C.midGray },
];
drugs.forEach((d, i) => {
const x = 0.38 + i * 3.08;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x, y:2.95, w:2.92, h:1.0, fill:{color:d.color}, line:{color:d.color}, rectRadius:0.1 });
s.addText(d.name, { x, y:2.95, w:2.92, h:0.45, fontSize:12.5, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
s.addText(d.mech + "\n" + d.note, { x, y:3.42, w:2.92, h:0.55, fontSize:10, color:C.white, fontFace:"Calibri", align:"center", valign:"top", margin:2 });
});
// Tier 3: Surgery
s.addShape(pres.shapes.RECTANGLE, { x:0.35,y:4.1,w:9.3,h:1.12, fill:{color:C.navy}, line:{color:C.navy} });
s.addText("3rd Line: Bariatric Surgery", { x:0.45,y:4.1,w:4.2,h:0.5, fontSize:14, bold:true, color:C.amber, fontFace:"Calibri", valign:"middle", margin:0 });
s.addText("For eligible obese patients (BMI ≥35 or ≥30 with comorbidities). Proven to improve/resolve MASH histology. Changes gut microbiome and bile acid signaling.", { x:0.45,y:4.58,w:9.0,h:0.58, fontSize:12, color:C.white, fontFace:"Calibri", valign:"top", margin:0 });
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 13 – KEY BIOCHEMISTRY POINTS (summary for exam)
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:10,h:5.625, fill:{color:C.cream}, line:{color:C.cream} });
titleBar(s, "High-Yield Biochemistry Points", "Must-know for MBBS exams");
const pts = [
{ num:"1", text:"Insulin resistance → ↑ SREBP-1c → ↑ de novo lipogenesis (ACC, FAS enzymes)" },
{ num:"2", text:"CPT-1 (carnitine palmitoyl transferase-1) is the rate-limiting enzyme of β-oxidation — inhibited in MASLD" },
{ num:"3", text:"VLDL export requires apoB-100 — impaired export → triglyceride accumulation" },
{ num:"4", text:"Lipotoxic lipids: palmitate (C16:0) and lysophosphatidylcholine induce hepatocyte apoptosis" },
{ num:"5", text:"ROS production via CYP2E1 and mitochondrial dysfunction drives oxidative stress" },
{ num:"6", text:"NLRP3 inflammasome activation → IL-1β & IL-18 (key drivers of MASH inflammation)" },
{ num:"7", text:"TGF-β → hepatic stellate cell → collagen I/III deposition → FIBROSIS" },
{ num:"8", text:"AST:ALT <1 in MASLD; >2 in alcoholic liver disease (remember for differentials)" },
];
pts.forEach((p, i) => {
const col = i % 2;
const row = Math.floor(i / 2);
const x = 0.35 + col * 4.88;
const y = 1.35 + row * 1.0;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x, y, w:4.65, h:0.88, fill:{color:C.white}, line:{color:C.teal, pt:1.5}, rectRadius:0.1, shadow:{type:"outer",color:"000000",blur:3,offset:1,angle:135,opacity:0.08} });
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:x+0.08, y:y+0.18, w:0.38, h:0.52, fill:{color:C.teal}, line:{color:C.teal}, rectRadius:0.06 });
s.addText(p.num, { x:x+0.08, y:y+0.18, w:0.38, h:0.52, fontSize:13, bold:true, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
s.addText(p.text, { x:x+0.55, y:y+0.08, w:4.0, h:0.72, fontSize:12, color:C.navy, fontFace:"Calibri", valign:"middle", margin:2, lineSpacingMultiple:1.15 });
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 14 – SUMMARY
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
// navy bg
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:10,h:5.625, fill:{color:C.navy}, line:{color:C.navy} });
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:0.35,h:5.625, fill:{color:C.teal}, line:{color:C.teal} });
s.addText("SUMMARY", { x:0.55,y:0.32,w:8.8,h:0.55, fontSize:28, bold:true, color:C.white, fontFace:"Calibri", charSpacing:5, margin:0 });
s.addShape(pres.shapes.RECTANGLE, { x:0.55,y:0.92,w:5.0,h:0.05, fill:{color:C.amber}, line:{color:C.amber} });
const summaryPoints = [
"MASLD = hepatic steatosis (≥5% hepatocytes) + at least 1 cardiometabolic risk factor",
"Central driver: INSULIN RESISTANCE → ↑ FFA → triglyceride accumulation",
"Two-hit model: Steatosis (Hit 1) → Oxidative stress/inflammation (Hit 2) → Fibrosis",
"FIBROSIS STAGE (not inflammation) is the key determinant of prognosis",
"Most patients are asymptomatic; AST:ALT < 1; diagnose via imaging ± biopsy",
"Leading complication: CVD (#1 killer); followed by cirrhosis, HCC",
"Treatment: Weight loss is king (≥10% reverses fibrosis); Resmetirom (2024 FDA) & Semaglutide (2025) now available",
"Remember: MASLD/MASH/MetALD is the new 2023 nomenclature replacing NAFLD/NASH",
];
summaryPoints.forEach((pt, i) => {
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:0.55, y:1.1+i*0.54, w:9.0, h:0.48, fill:{color:i%2===0?"1A3B55":"122B40"}, line:{color:C.teal, pt:1}, rectRadius:0.07 });
s.addText([
{ text: "▸ ", options: { color: C.amber, bold: true } },
{ text: pt, options: { color: C.white } }
], { x:0.68, y:1.1+i*0.54, w:8.78, h:0.48, fontSize:12.5, fontFace:"Calibri", valign:"middle", margin:0 });
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 15 – THANK YOU / REFERENCES
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:10,h:5.625, fill:{color:C.navy}, line:{color:C.navy} });
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:0.35,h:5.625, fill:{color:C.teal}, line:{color:C.teal} });
s.addShape(pres.shapes.RECTANGLE, { x:0,y:4.8,w:10,h:0.85, fill:{color:C.teal}, line:{color:C.teal} });
s.addText("Thank You", { x:0.6,y:0.6,w:8.8,h:1.1, fontSize:50, bold:true, color:C.white, fontFace:"Calibri", margin:0 });
s.addShape(pres.shapes.RECTANGLE, { x:0.6,y:1.72,w:4.5,h:0.06, fill:{color:C.amber}, line:{color:C.amber} });
s.addText("Questions & Discussion", { x:0.6,y:1.82,w:8.5,h:0.5, fontSize:18, color:C.amber, fontFace:"Calibri", italic:true, margin:0 });
s.addText("References", { x:0.6,y:2.5,w:8.5,h:0.42, fontSize:14, bold:true, color:C.midGray, fontFace:"Calibri", margin:0 });
s.addText([
{ text: "1. Robbins & Kumar Basic Pathology, 10th Ed — Chapter 14\n", options:{breakLine:false} },
{ text: "2. Yamada's Textbook of Gastroenterology, 7th Ed — Chapter 106\n", options:{breakLine:false} },
{ text: "3. 2024 European MASLD Clinical Practice Guidelines (EASL/EASO/EANM)\n", options:{breakLine:false} },
{ text: "4. AASLD 2025 Practice Guidance on Semaglutide for MASH (PMID: 41201884)\n", options:{breakLine:false} },
{ text: "5. Suvarna R et al., Sci Rep 2024 — Resmetirom meta-analysis (PMID: 39187533)", options:{breakLine:false} },
], { x:0.6, y:2.98, w:8.8, h:1.7, fontSize:11.5, color:C.midGray, fontFace:"Calibri", lineSpacingMultiple:1.4, margin:0 });
s.addText("Biochemistry Seminar • MBBS 1st Year • 2026", { x:0,y:4.8,w:10,h:0.85, fontSize:13, color:C.white, fontFace:"Calibri", align:"center", valign:"middle", margin:0 });
}
// ─── WRITE FILE ────────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/fatty-liver-ppt/Fatty_Liver_Disease_MBBS.pptx" })
.then(() => console.log("SUCCESS: PPT saved."))
.catch(err => { console.error("ERROR:", err); process.exit(1); });
Running Command
cd /home/daytona/workspace/fatty-liver-ppt && node create_ppt.js 2>&1
Running Command
ls -lh /home/daytona/workspace/fatty-liver-ppt/Fatty_Liver_Disease_MBBS.pptx
Your PPT is ready! Download it here:
Fatty Liver Disease MBBS
Presentation · PPTX
What's inside (15 slides)
| # | Slide | Content |
|---|---|---|
| 1 | Title Slide | Navy/teal design with amber accents |
| 2 | Seminar Outline | 10-topic overview with numbered chips |
| 3 | Definition | Key definition card + 3 fact boxes (prevalence, ALT/AST, reversibility) |
| 4 | Types of Fatty Liver | SLD umbrella with MASLD / MetALD / ALD / Other categorized in cards |
| 5 | Normal Lipid Metabolism | Hepatocyte flow diagram (inputs → hepatocyte → outputs) |
| 6 | Pathogenesis: Two-Hit Model | Hit 1 (steatosis) vs Hit 2 (inflammation) side-by-side boxes |
| 7 | Biochemical Mechanisms | 4-card grid: Insulin resistance, Lipid accumulation, Oxidative stress, Inflammation |
| 8 | Risk Factors | 6-card grid covering obesity, T2DM, dyslipidemia, HTN, genetics, alcohol |
| 9 | Disease Spectrum & Progression | Steatosis → MASH → F1-F2 → F3 → Cirrhosis with % progression rates |
| 10 | Clinical Features & Diagnosis | Two-column layout: symptoms vs diagnostic tools |
| 11 | Complications | Cirrhosis, HCC, CVD, metabolic syndrome - 4 cards |
| 12 | Treatment & Management | 3-tier layout: lifestyle → pharmacotherapy (resmetirom, semaglutide) → bariatric surgery |
| 13 | High-Yield Biochemistry Points | 8 exam-focused facts (SREBP-1c, CPT-1, VLDL, NLRP3, TGF-β, etc.) |
| 14 | Summary | Dark slide with 8 key takeaways |
| 15 | Thank You / References | Textbook + guideline citations |
Color scheme: Navy dominant, teal headers, amber highlights - designed for a professional biochemistry seminar look.
This is a shared conversation. Sign in to Orris to start your own chat.