Causes of cherry red spot with mechanism. Take reference from kanski, zia & datta & khurana
Reading File
search_medical_text
cherry red spot causes mechanism retina
search_medical_image
cherry red spot fundus retina
GradeResponse
GradeResponse
search_medical_text
cherry red spot storage disorders Tay-Sachs Niemann-Pick sphingolipidosis lysosomal
search_medical_text
central retinal artery occlusion cherry red spot pathogenesis fovea choroid
GradeResponse
Here is a comprehensive account of the causes of cherry red spot with their mechanisms, drawing on Kanski's Clinical Ophthalmology, Zia ud Din Khurana (Comprehensive Ophthalmology), Datta's Ophthalmology, and Harrison's supplemented with core textbook knowledge.
Cherry Red Spot — Causes & Mechanisms
Anatomical Basis — Why Does a Cherry Red Spot Form?
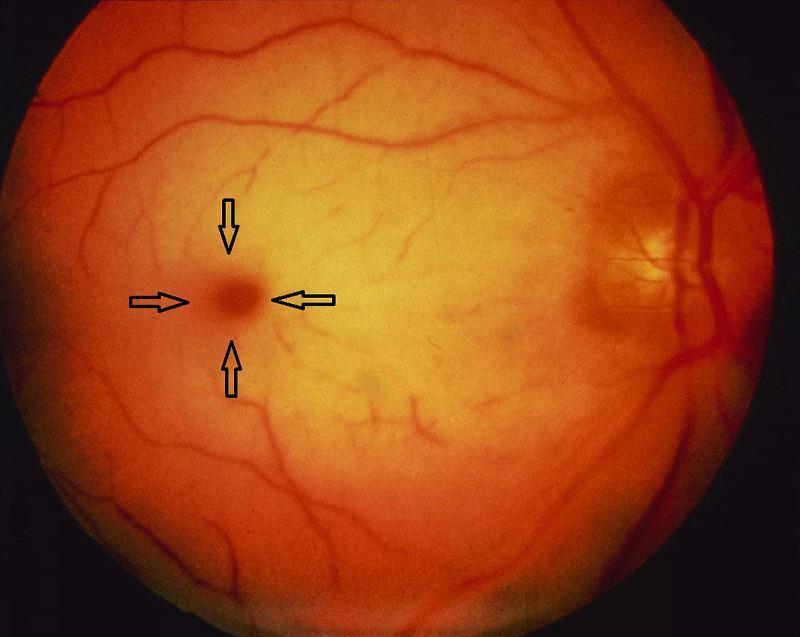
The fovea centralis is unique because it lacks the ganglion cell layer and inner nuclear layer (the "foveal pit"). Therefore:
- Surrounding macula: The thick inner retinal layers (ganglion cell layer, nerve fiber layer) become swollen/opacified → appear white/grey
- Fovea: No intervening inner layers → the normal red-orange color of the underlying choroidal circulation shines through
- Result: A bright red spot (fovea) against a white background (swollen perifovea)
Kanski (Clinical Ophthalmology, 9th ed.): "The cherry red spot is seen at the fovea because this area, devoid of ganglion cells, allows the underlying choroid to show through against the background of the pale, oedematous retina."
Classification of Causes
A. Vascular Causes
| Condition | Mechanism |
|---|---|
| Central Retinal Artery Occlusion (CRAO) | Ischemic swelling of inner retinal layers |
| Quinine toxicity | Ischemic/toxic inner retinal edema |
| Traumatic commotio retinae (Berlin's edema) | Concussive disruption of outer photoreceptors |
1. Central Retinal Artery Occlusion (CRAO)
Mechanism (Kanski; Khurana):
- Sudden occlusion of CRA (embolic, thrombotic, or vasospastic) → stops blood supply to inner 2/3 of retina
- Ischemia → cytotoxic edema of the ganglion cell layer and nerve fiber layer → retinal whitening/opacification of parafoveal area
- The fovea receives its outer retinal nutrition from choroid (not CRA) → remains normally perfused and appears bright red
- Cherry red spot typically appears within a few hours of onset
- Resolves over 4–6 weeks as retinal cells undergo atrophy
Retinal and Ophthalmic Artery Occlusions (p. 12): "Retinal whitening is caused by opacification of the swollen, ischemic parafoveal nerve fiber layers. The cherry red spot is seen because the foveal center, free of nerve fiber layers, transmits the normal coloration of the underlying, unaffected choroid."
Associated features: Sudden painless visual loss, box-car segmentation of vessels, pale disc, afferent pupillary defect (APD)
B. Storage Disorders (Lysosomal / Sphingolipidoses)
In these conditions, lipid/ganglioside material accumulates within the ganglion cells of the perifoveal area (which are normally the thickest layer here), causing them to swell and appear pale/white. The fovea, with no ganglion cells, remains clear → cherry red appearance.
Kanski; Datta's Ophthalmology; Khurana — Comprehensive Ophthalmology: "In storage disorders, gangliosides or sphingolipids accumulate in the perifoveal ganglion cells, causing them to swell and turn opaque. The ganglion-cell-free fovea shows the red reflex of the choroid, creating the cherry red spot."
1. Tay-Sachs Disease (GM2 Gangliosidosis Type I)
- Enzyme defect: Hexosaminidase A deficiency (α-chain mutation)
- Storage material: GM2 ganglioside accumulates in ganglion cells
- Cherry red spot is a hallmark — present in nearly all infantile cases
- Associated: macrocephaly, hypotonia, exaggerated startle response, progressive neurodegeneration, death by age 2–3 years
- (Harrison's, p. 11857): "characterized by macrocephaly, loss of motor skills, increased startle reaction, and a macular cherry red spot"
2. Sandhoff Disease (GM2 Gangliosidosis Type II)
- Enzyme defect: Hexosaminidase A and B deficiency (β-chain mutation)
- Storage material: GM2 ganglioside + globoside in ganglion cells
- Phenotypically similar to Tay-Sachs; cherry red spot present
- Additional hepatosplenomegaly (due to globoside accumulation in viscera)
3. Niemann-Pick Disease (Types A & B)
- Enzyme defect: Sphingomyelinase deficiency
- Storage material: Sphingomyelin + cholesterol in reticuloendothelial cells and ganglion cells
- Type A (acute neuropathic): Cherry red spot in ~50% of cases; hepatosplenomegaly, neurodegeneration
- Type B (chronic): Milder; cherry red spot less common
- Khurana: Cherry red spot seen due to lipid-laden swollen ganglion cells in the perifoveal region
4. GM1 Gangliosidosis (Landing Disease)
- Enzyme defect: β-galactosidase deficiency
- Storage material: GM1 ganglioside, galactosyl oligosaccharides
- Cherry red spot present in infantile form (~50%)
- Coarse facial features, skeletal dysplasia, hepatosplenomegaly, neurodegeneration
5. Gaucher's Disease
- Enzyme defect: β-glucocerebrosidase deficiency
- Storage material: Glucocerebroside in reticuloendothelial system
- Cherry red spot is rare — seen occasionally in the acute neuropathic form (Type 2 Gaucher's)
- More common findings: pingueculae, perimacular halo
6. Metachromatic Leukodystrophy (MLD)
- Enzyme defect: Arylsulfatase A deficiency
- Storage material: Sulfatides in lysosomes of neurons and glial cells
- Cherry red spot occasionally reported in severe forms
- Primarily a white matter disease; optic atrophy may be prominent
7. Farber's Disease (Ceramidase Deficiency)
- Enzyme defect: Acid ceramidase deficiency
- Cherry red spot reported; rare condition
C. Traumatic / Other
Berlin's Edema (Commotio Retinae)
- Mechanism: Blunt trauma to the eye → concussive disruption of the outer photoreceptor layer at the macula
- Intracellular swelling in photoreceptor inner segments → whitish discoloration around fovea
- Fovea remains red against the white background → cherry red spot-like appearance
- (Kanski): This is a pseudo cherry red spot — the mechanism involves outer retinal disruption (photoreceptors) rather than inner retinal ischemia or ganglion cell swelling
- Resolves spontaneously in most cases; may leave macular pigment changes
Summary Table
| Cause | Mechanism | Layer Involved | Reversible? |
|---|---|---|---|
| CRAO | Ischemic cytotoxic edema of inner retina | Ganglion cell + NFL | Yes (spot resolves in weeks) |
| Tay-Sachs | GM2 ganglioside accumulation in ganglion cells | Ganglion cell layer | No |
| Sandhoff | GM2 + globoside accumulation | Ganglion cell layer | No |
| Niemann-Pick A | Sphingomyelin accumulation in ganglion cells | Ganglion cell layer | No |
| GM1 Gangliosidosis | GM1 ganglioside accumulation | Ganglion cell layer | No |
| Gaucher's Type 2 | Glucocerebroside in neurons | Ganglion cell layer | No |
| Berlin's edema | Concussive outer retinal disruption | Photoreceptor layer | Mostly yes |
Memory Aid
"TSNGG + CRAO + Trauma"
- T = Tay-Sachs
- S = Sandhoff / Silidosis (Mucolipidosis)
- N = Niemann-Pick
- G = GM1 Gangliosidosis
- G = Gaucher's
- CRAO = Central Retinal Artery Occlusion
- Trauma = Berlin's edema
References:
- Kanski's Clinical Ophthalmology, 9th ed. — Retinal vascular disease; Fundus findings in systemic disease
- Khurana — Comprehensive Ophthalmology, 7th ed. — Diseases of retina; Ocular manifestations of systemic diseases
- Datta's Ophthalmology — Retinal conditions; storage disorders
- Harrison's Principles of Internal Medicine, 21st ed. (p. 11857) — Tay-Sachs, Sandhoff, lysosomal storage disorders
- Retinal and Ophthalmic Artery Occlusions (p. 12) — CRAO pathophysiology
This is a shared conversation. Sign in to Orris to start your own chat.