Pneumothorax full details for md exams 15marks
Reading File
search_medical_text
pneumothorax types classification pathophysiology etiology
search_medical_text
pneumothorax clinical features diagnosis CXR management treatment
search_medical_image
pneumothorax chest X-ray findings tension pneumothorax
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive 15-mark answer on Pneumothorax structured for MD examinations:
PNEUMOTHORAX
Definition
Pneumothorax is the presence of air in the pleural space (between the visceral and parietal pleura), leading to partial or complete lung collapse.
Classification / Types
1. Spontaneous Pneumothorax
A. Primary Spontaneous Pneumothorax (PSP)
- Occurs in the absence of underlying lung disease
- Typically tall, thin young males (M:F = 6:1), 20–30 years
- Caused by rupture of subpleural blebs/bullae (apical)
- Risk factors: smoking, Marfan syndrome, family history
B. Secondary Spontaneous Pneumothorax (SSP)
- Occurs as a complication of underlying lung disease
- More dangerous — less cardiopulmonary reserve
- Causes: COPD/emphysema (most common), asthma, TB, cystic fibrosis, Pneumocystis pneumonia, lung abscess, malignancy
2. Traumatic Pneumothorax
- Penetrating chest trauma (stab wound, gunshot)
- Blunt chest trauma (rib fractures lacerating lung)
- Iatrogenic: central line insertion, thoracentesis, lung biopsy, mechanical ventilation (barotrauma), tracheostomy
3. Tension Pneumothorax
- Air enters pleural space via a one-way valve mechanism
- Progressive air accumulation → increasing intrapleural pressure
- Life-threatening emergency: collapses ipsilateral lung, displaces mediastinum, compresses contralateral lung and great veins → reduced venous return → cardiovascular collapse
- Causes: penetrating trauma, mechanical ventilation (PEEP), failed intercostal tube
4. Open Pneumothorax (Sucking Chest Wound)
- Open communication between pleural space and atmosphere
- Air moves through the defect with each breath ("sucking" sound)
5. Catamenial Pneumothorax
- Rare; associated with thoracic endometriosis
- Occurs within 24–72 hours of menstruation, right-sided predominantly
Pathophysiology
Normally the pleural space is a potential space with slightly negative pressure (−5 to −8 cmH₂O). When air enters:
- Negative pressure is lost → elastic recoil of lung causes collapse
- Degree of collapse depends on volume of air and compliance of lung
- In tension pneumothorax, each breath traps more air → intrapleural pressure rises above atmospheric → mediastinal shift → kinking of SVC/IVC → obstructive shock
Clinical Features
Symptoms
| Feature | Details |
|---|---|
| Chest pain | Sudden, pleuritic, ipsilateral (classic presenting feature) |
| Dyspnea | Variable — mild in PSP, severe in SSP/tension |
| Dry cough | Occasional |
| Shock | Only in tension pneumothorax |
Signs
| Sign | Finding |
|---|---|
| Inspection | Reduced chest movement on affected side |
| Trachea | Central (simple) or deviated away from affected side (tension) |
| Percussion | Hyper-resonance over affected hemithorax |
| Auscultation | Diminished/absent breath sounds on affected side |
| Vocal resonance | Reduced |
Tension Pneumothorax — Clinical Triad
- Tracheal deviation away from affected side
- Absent breath sounds + hyper-resonance
- Hemodynamic instability (hypotension, tachycardia, raised JVP)
⚠️ Tension pneumothorax is a clinical diagnosis — do NOT wait for X-ray confirmation before treatment. (Bailey & Love's Surgery, 28th Ed., p. 395)
Investigations
1. Chest X-Ray (Erect PA — First Line)
- Visible pleural line (visceral pleural edge) with absent lung markings beyond it
- Lung collapse (partial/complete)
- In tension: mediastinal shift, depressed ipsilateral diaphragm, contralateral lung compression

Sizing (BTS Classification):
- Small: visible rim < 2 cm at level of hilum
- Large: visible rim ≥ 2 cm at level of hilum
2. CT Chest (Gold Standard)
- Confirms diagnosis when CXR is equivocal
- Identifies underlying bullae/blebs, quantifies size accurately
- Best for secondary pneumothorax with underlying lung disease
3. FAST Ultrasound
- Absence of "lung sliding" sign on M-mode
- Presence of "barcode/stratosphere sign" (normal: "seashore sign")
- Rapid, bedside, especially useful in trauma
4. ABG
- May show hypoxemia, hypocapnia (compensatory hyperventilation)
- Severe: respiratory acidosis (tension PTX)
5. ECG
- Tachycardia
- Decreased voltage on affected side
- May mimic anterior MI (rarely)
Management
A. Tension Pneumothorax — Emergency Treatment
- Immediate needle decompression:
- 14–16G cannula into 2nd intercostal space, midclavicular line (MCL), affected side
- Hissing of air confirms diagnosis
- Followed by intercostal chest drain (ICD):
- 5th ICS, anterior axillary line ("safe triangle")
B. Simple/Spontaneous Pneumothorax — BTS Guidelines
| Scenario | Treatment |
|---|---|
| Small PSP (< 2 cm), minimal symptoms | Observe, discharge, review in 2–4 weeks; high-flow O₂ (accelerates resorption) |
| Large PSP (≥ 2 cm) or symptomatic | Needle aspiration (16G cannula, 2nd ICS MCL) as first step |
| If aspiration fails | ICD (Seldinger technique) preferred |
| SSP (any size) | Requires ICD or needle aspiration depending on severity |
| SSP + mechanically ventilated | Always ICD |
C. Intercostal Chest Drain (ICD)
- Position: 5th ICS, anterior axillary line (triangle of safety)
- Triangle of safety: anterior border of latissimus dorsi, lateral border of pectoralis major, 5th ICS
- Connected to underwater seal drainage
- Remove when: lung fully expanded + no air leak for 24 hours
D. Surgical Management — Video-Assisted Thoracoscopic Surgery (VATS)
Indications:
- 2nd ipsilateral recurrence
- 1st recurrence in bilateral/contralateral PTX
- Persistent air leak > 5–7 days
- Haemopneumothorax
- Occupational risk patients (pilots, divers) after first episode
Procedure: VATS bullectomy + pleurodesis (mechanical or chemical)
E. Chemical Pleurodesis
- Agents: Talc (most effective), tetracycline, bleomycin
- Induces pleural symphysis → prevents recurrence
- Done via ICD or at VATS
Complications
| Complication | Notes |
|---|---|
| Recurrence | PSP: 25–30% within 2 years; SSP: higher |
| Haemopneumothorax | Blood + air in pleural space |
| Empyema | Post-ICD infection |
| Chronic pneumothorax | Persistent air leak > 3 months |
| Re-expansion pulmonary edema | Rapid lung re-expansion after large PTX |
| Tension pneumothorax | Cardiovascular collapse, fatal if untreated |
Key Differentials
- Acute MI (especially in young patient with chest pain)
- Pulmonary embolism
- Pleuritis
- Aortic dissection
- Giant emphysematous bulla (mimics PTX on CXR)
High-Yield Points for MD Exam
| Point | Detail |
|---|---|
| Most common cause of PSP | Rupture of apical subpleural blebs |
| Most common cause of SSP | COPD/Emphysema |
| Most common iatrogenic cause | Central venous catheter insertion |
| CXR finding | Visible pleural line, absent lung markings peripheral |
| First-line for large PSP | Needle aspiration (not ICD) |
| ICD position | 5th ICS, anterior axillary line |
| Tension PTX: trachea deviated | Away from affected side |
| Treatment of tension PTX | Immediate needle decompression (2nd ICS, MCL) |
| Definitive prevention of recurrence | VATS + bullectomy + pleurodesis |
| Best pleurodesis agent | Talc |
Prognosis
- PSP: Excellent prognosis; 25–30% recurrence rate without surgery; near-zero after VATS pleurodesis
- SSP: Depends on underlying disease; higher morbidity and mortality
- Tension PTX: Fatal if untreated; full recovery if promptly decompressed
References: Bailey & Love's Short Practice of Surgery, 28th Edition, p. 395; BTS Guidelines on Spontaneous Pneumothorax; Harrison's Principles of Internal Medicine, 21st Edition.
Eloborate still more
search_medical_text
pneumothorax pathophysiology pleural pressure mechanics lung collapse
search_medical_text
pneumothorax surgical management VATS pleurodesis recurrence prevention indications
search_medical_image
pneumothorax types anatomy diagram pleural space
GradeResponse
GradeResponse
GradeResponse
Here is the fully elaborated, exhaustive answer on Pneumothorax — exam-ready at the highest detail level:
PNEUMOTHORAX — COMPLETE ELABORATED ANSWER
1. DEFINITION
Pneumothorax is defined as an abnormal collection of air or gas within the pleural cavity (between the visceral and parietal pleura), resulting in partial or complete collapse of the underlying lung.
The term is derived from Greek: pneuma (air) + thorax (chest).
2. SURGICAL / APPLIED ANATOMY OF THE PLEURAL SPACE
- The pleural cavity is a potential space bounded by:
- Visceral pleura: covers the lung surface
- Parietal pleura: lines the chest wall, diaphragm, and mediastinum
- Normal pleural fluid volume: 5–15 mL (lubricating layer)
- Intrapleural pressure: −5 to −8 cmH₂O at rest; −15 to −20 cmH₂O during inspiration
- This negative pressure is generated by the opposing elastic recoil of the lung (tending to collapse) and chest wall (tending to expand)
- Pleural fluid dynamics: produced from parietal pleural capillaries (Starling forces — net secretion ~11 mmHg); reabsorbed mainly by visceral pleural capillaries (pulmonary circulation, net absorbing pressure ~6 mmHg) (Bailey & Love's, 28th Ed., p. 999)
- Elastic recoil of the lung contributes ~4 mmHg negative pressure, favouring lung expansion as long as the pleural seal is intact
When this seal is broken and air enters the pleural space, negative pressure is lost and the lung collapses due to its own elastic recoil.
3. CLASSIFICATION — DETAILED
A. Spontaneous Pneumothorax
i. Primary Spontaneous Pneumothorax (PSP)
- No clinically apparent underlying lung disease
- Incidence: 18–28/100,000/year (males), 1.2–6/100,000/year (females)
- Peak age: 20–30 years
- Body habitus: tall, thin, lean males (low BMI → stretched lung apices)
- Pathology: rupture of subpleural emphysematous blebs or bullae at lung apices
- Blebs: intrapleural air collections within visceral pleural layers
- Bullae: intraparenchymal air spaces > 1 cm diameter
- Mechanism: high alveolar-to-pleural pressure gradient at apex (gravity-dependent ventilation:perfusion mismatch) → ischemia → bleb formation → rupture
- Risk factors:
- Smoking (relative risk increased 20-fold in heavy smokers) — most important modifiable factor
- Marfan syndrome, homocystinuria, Ehlers-Danlos syndrome (connective tissue disorders)
- Family history (autosomal dominant tendency)
- Cannabis smoking
- Scuba diving, high-altitude activities
ii. Secondary Spontaneous Pneumothorax (SSP)
- Complicates existing pulmonary pathology
- More serious — reduced cardiopulmonary reserve leaves less tolerance
- Causes:
| Obstructive | COPD (most common overall), asthma, cystic fibrosis |
|---|---|
| Infectious | TB (most common in developing countries), Pneumocystis jirovecii pneumonia (PCP), necrotizing pneumonia, lung abscess, hydatid cyst rupture |
| Interstitial/Fibrotic | Langerhans cell histiocytosis, lymphangioleiomyomatosis (LAM — young women), sarcoidosis |
| Malignancy | Primary lung cancer, metastases (sarcomas — cannon ball metastases) |
| Rare | Marfan syndrome, tuberous sclerosis, Birt-Hogg-Dubé syndrome |
B. Traumatic Pneumothorax
i. Penetrating Trauma
- Stab wounds, gunshot wounds, impalement injuries
- Air enters directly through chest wall defect or via lacerated lung/bronchus
ii. Blunt Trauma
- Rib fractures → lacerate visceral pleura
- Sudden compression → alveolar rupture
- Tracheobronchial tears
iii. Iatrogenic (Most Common Cause Overall in Hospitals)
- Central venous catheter insertion (subclavian > internal jugular) — most common
- Thoracentesis / pleural aspiration
- Pleural biopsy
- CT-guided lung biopsy / FNAC
- Mechanical ventilation (barotrauma/volutrauma, especially with high PEEP)
- Positive pressure ventilation
- Tracheostomy
- Intercostal nerve blocks
- Acupuncture (rare)
C. Tension Pneumothorax
- One-way ball-valve mechanism: air enters pleural space during inspiration but cannot escape during expiration
- Progressive rise in intrapleural pressure above atmospheric → ipsilateral lung collapse → mediastinal shift → compression of contralateral lung → kinking/compression of SVC and IVC → reduced venous return → obstructive shock
- Without treatment: fatal within minutes
- Causes: penetrating chest wounds, mechanical ventilation, faulty ICD (clamped/blocked), traumatic pneumothorax with valvular flap
D. Open Pneumothorax (Sucking Chest Wound)
- Large chest wall defect (> 2/3 of tracheal diameter) → air preferentially enters through wound rather than trachea
- Audible "sucking" sound with each breath
- Leads to paradoxical breathing, ventilation failure
- First aid: 3-sided occlusive dressing (Asherman seal) — allows air out but not in
E. Catamenial Pneumothorax
- Rare condition (< 5% of all pneumothoraces in women)
- Thoracic endometriosis — diaphragmatic defects allow peritoneal air/endometrial implants to reach pleura
- Occurs within 24–72 hours of onset of menstruation
- Almost exclusively right-sided (98%)
- Recurrence inevitable without hormonal therapy
- Treatment: hormonal suppression (GnRH analogues, OCP) + VATS excision of endometriotic deposits + diaphragm repair + pleurodesis
F. Neonatal Pneumothorax
- Occurs due to high transpulmonary pressures during first breaths
- Complication of meconium aspiration syndrome, RDS, vigorous resuscitation
4. PATHOPHYSIOLOGY — IN DEPTH
Air enters pleural space
↓
Loss of negative intrapleural pressure
↓
Lung elastic recoil → lung collapses
↓
Ventilation-perfusion mismatch → Hypoxemia
↓
Compensatory tachypnoea + sympathetic activation
↓ (if tension)
Progressive air accumulation (ball-valve)
↓
Rising intrapleural pressure → mediastinal shift
↓
Contralateral lung compression (↓ ventilation)
SVC/IVC kinking (↓ venous return)
↓
Obstructive shock → cardiac arrest
Physiological Consequences:
| Parameter | Effect |
|---|---|
| FRC (functional residual capacity) | Decreased |
| Lung compliance | Decreased on affected side |
| PaO₂ | Decreased (V/Q mismatch) |
| PaCO₂ | Initially decreased (hyperventilation), rises in tension |
| Venous return | Decreased in tension |
| Cardiac output | Decreased in tension |
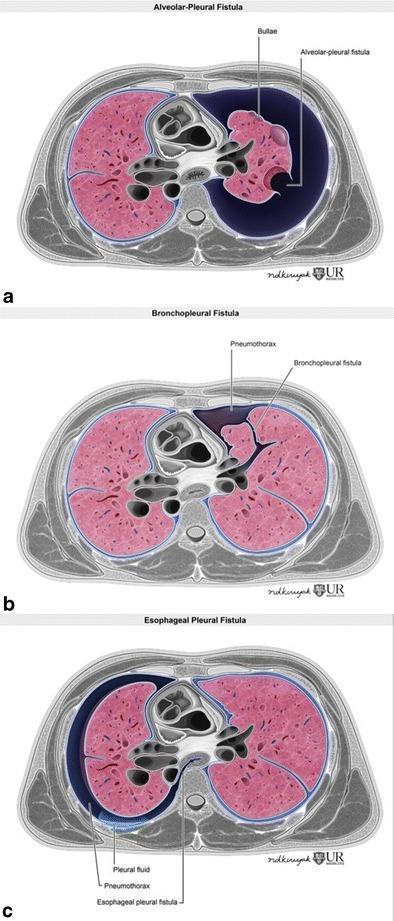
Fistulous Mechanisms (Air Leak Pathways):
5. CLINICAL FEATURES — DETAILED
Symptoms
| Symptom | PSP | SSP | Tension |
|---|---|---|---|
| Chest pain | Sudden, sharp, pleuritic, ipsilateral | Same | Severe |
| Dyspnoea | Mild–moderate | Severe (limited reserve) | Severe, progressive |
| Cough | Dry, irritating | Variable | — |
| Palpitations | Mild tachycardia | — | Severe |
| Syncope/collapse | Rare | Rare | Yes (shock) |
| Anxiety/agitation | Mild | — | Marked |
- Pain: described as "tearing" or "knife-like", typically worsens with breathing
- Symptoms may be surprisingly mild in PSP (young, healthy lungs can compensate)
- Symptoms typically begin at rest or with mild activity (NOT during strenuous exercise — distinguishes from cardiac causes)
Signs
| Examination | Finding |
|---|---|
| General | Tachycardia, tachypnoea, distress |
| Trachea | Midline in simple PTX; deviated AWAY from affected side in tension |
| Chest expansion | Decreased on affected side |
| Percussion | Hyper-resonance on affected side |
| Auscultation | Absent/diminished breath sounds on affected side |
| Vocal fremitus/resonance | Decreased on affected side |
| JVP | Raised in tension (due to obstructed venous return) |
| BP | Normal in simple; Hypotension in tension |
| SpO₂ | Mildly reduced in simple; critically low in tension |
| Skin | Cyanosis, diaphoresis in tension |
Classic Tension Pneumothorax Presentation — "5 Ds"
- Dyspnoea (severe, progressive)
- Distended neck veins (raised JVP)
- Deviation of trachea (away from affected side)
- Decreased breath sounds (ipsilateral)
- Drop in BP (hypotension/shock)
6. INVESTIGATIONS
A. Chest X-Ray (Standard Erect PA)
Findings:
- Visible visceral pleural line (white line) with no lung markings beyond it
- Hyperlucency of affected hemithorax
- Partial or complete lung collapse — lung retracted toward hilum
- Depression of ipsilateral hemidiaphragm (in large PTX)
- Widening of intercostal spaces (in large PTX)
In Tension PTX:
- Mediastinal shift away from affected side
- Tracheal deviation away from affected side
- Compression of contralateral lung
- Flattening/depression of ipsilateral diaphragm
BTS Size Classification on CXR:
- Small: visible rim of air < 2 cm at level of hilum
- Large: visible rim of air ≥ 2 cm at level of hilum
- A 2 cm rim corresponds to approximately 50% lung volume loss
Note on Supine CXR (ICU patients):
- PTX may appear as deep sulcus sign — abnormally deep, lucent costophrenic angle
- Hyperlucency of upper abdomen
- Lung edge may not be visible — easy to miss
B. CT Chest — Gold Standard
- Most accurate for sizing and characterizing pneumothorax
- Identifies underlying blebs, bullae, emphysema, malignancy
- Distinguishes PTX from giant emphysematous bullae (important — wrong treatment if misdiagnosed)
- Quantifies size accurately when CXR is equivocal
- Detects occult pneumothorax (missed on plain film)
- Guides surgical planning (identifies bleb location)
C. Ultrasound (FAST/POCUS — increasingly used in trauma/ICU)
| Finding | Normal | Pneumothorax |
|---|---|---|
| Lung sliding | Present (shimmering pleura) | Absent |
| M-mode | Seashore sign (sandy pattern) | Barcode/Stratosphere sign (parallel lines) |
| B-lines | Present | Absent (B-lines rule out PTX) |
| Lung pulse | Present | Absent |
- Sensitivity 86–98%, Specificity ~100% for PTX detection
- Advantage: bedside, no radiation, faster than CXR in emergencies
D. Arterial Blood Gas (ABG)
| Stage | Findings |
|---|---|
| Mild/early | Mild hypoxaemia; hypocapnia (hyperventilation) |
| Moderate | PaO₂ ↓↓, PaCO₂ normal |
| Severe/tension | Hypoxaemia + respiratory acidosis (PaCO₂ ↑) |
E. ECG
- Sinus tachycardia (most common)
- Rightward QRS axis shift (right-sided PTX)
- Decreased R-wave amplitude / electrical alternans (mimics pericardial effusion)
- T-wave inversions in anterior leads (right-sided)
- May mimic anterior STEMI — important differential
F. Other
- Peak flow/spirometry: reduced FEV1, FVC on affected side
- Oximetry: SpO₂ monitoring
- Blood tests: FBC, CRP (if infective cause suspected); LDH, ADA (if TB or malignancy suspected)
7. DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Features |
|---|---|
| Acute MI | ECG changes, troponin rise, no absent breath sounds |
| Pulmonary embolism | Normal breath sounds, D-dimer, CTPA |
| Aortic dissection | Tearing pain radiating to back, BP difference between arms |
| Acute severe asthma | Bilateral wheeze, no absent breath sounds |
| Pericardial tamponade | Muffled heart sounds, raised JVP, no hyper-resonance |
| Giant emphysematous bulla | CT differentiates — no mediastinal shift, no acute onset |
| Diaphragmatic hernia | Bowel sounds in chest, CXR shows bowel loops |
| Haemothorax | Dullness (not hyper-resonance) on percussion |
8. MANAGEMENT — COMPREHENSIVE ALGORITHM
STEP 1: Is it Tension Pneumothorax?
If YES → Do not wait for imaging — treat immediately
Tension Pneumothorax Management:
- High-flow O₂ (15 L/min via non-rebreather mask) — immediately
- Emergency needle decompression:
- 14–16G IV cannula
- 2nd ICS, midclavicular line (MCL), upper border of 3rd rib (to avoid neurovascular bundle)
- Hissing of air = confirms diagnosis
- Converts tension → simple pneumothorax
- Definitive: Intercostal chest drain (ICD):
- Insert into 5th ICS, anterior axillary line (triangle of safety)
- Attach to underwater seal drain
- If IV access/decompression not possible: open thoracostomy (trauma setting)
STEP 2: Simple Spontaneous Pneumothorax — BTS Algorithm
Is it symptomatic? / Is the patient breathless?
|
YES ←——|——→ NO
| |
Large? Small PSP (<2cm)?
(≥2cm rim) |
| YES ——→ Observe, discharge with safety advice
↓ High-flow O₂ if admitted
Needle Aspiration Review in 2-4 weeks with CXR
(1st line attempt)
|
Successful? → YES → Observe 1h → CXR → Discharge + review
|
NO
↓
Intercostal Chest Drain (ICD)
|
Persistent air leak > 3-5 days?
↓
VATS / Surgical consultation
STEP 3: Needle Aspiration (Simple Aspiration) — Technique
- Indication: Large/symptomatic PSP, first attempt before ICD
- Equipment: 16G cannula + 50 mL syringe + 3-way tap
- Site: 2nd ICS, MCL (or 4th/5th ICS, anterior axillary line)
- Procedure: Aspirate until resistance felt, patient coughs, or 2.5 L air aspirated
- Success: CXR after 1 hour shows expanded lung → discharge
- Failure: Recurrence/failure → proceed to ICD
- Success rate: ~60–80% in PSP; not recommended in SSP (proceed directly to ICD)
STEP 4: Intercostal Chest Drain (ICD)
Triangle of Safety (BTS):
- Anterior border: lateral border of pectoralis major
- Posterior border: anterior border of latissimus dorsi
- Inferior border: level of 5th ICS (nipple level)
- Apex: axilla
Technique:
- Position: patient supine or 45°, arm raised above head
- Landmark: 4th or 5th ICS, midaxillary line
- Anaesthetize skin, subcutaneous tissue, rib periosteum, parietal pleura (lidocaine 1%)
- Blunt dissection into pleural space (never trocar directly — risk of injury)
- Insert finger to confirm pleural space, clear adhesions
- Advance drain (28–32F for haemopneumothorax; smaller for simple PTX)
- Connect to underwater seal drain (UWS)
- Secure with suture, apply occlusive dressing
Underwater Seal Drain:
- Bottle filled with sterile water to 2 cm depth
- Long tube submerged — creates water seal
- Swinging: water level oscillates with respiration → confirms correct placement
- Bubbling: indicates ongoing air leak
- No swinging + no bubbling: drain is blocked OR lung is fully expanded
When to Remove ICD:
- Lung fully re-expanded on CXR
- No air bubbling for 24 hours
- Drain fluid output < 150–200 mL/day (if haemothorax)
- Remove at end-expiration with Valsalva (or end-inspiration — depends on local protocol)
- Apply occlusive dressing immediately on removal
STEP 5: Surgical Management
Indications for Surgery (VATS):
- 2nd ipsilateral spontaneous pneumothorax
- 1st episode with bilateral or contralateral pneumothorax
- 1st episode in high-risk occupations (pilots, divers, parachutists)
- 1st episode with haemopneumothorax
- Persistent air leak > 5–7 days despite ICD
- Failure of lung expansion with ICD
- Spontaneous pneumothorax in remote areas (profession/geography)
- Patient preference after fully counselled
VATS Procedure: (Bailey & Love's, 28th Ed., p. 1002)
The object is threefold:
- Deal with air leaks — staple/oversew bullae, close fistulae
- Search for and obliterate blebs and bullae (bullectomy)
- Make the visceral pleura adherent to the parietal pleura (pleurodesis) — so subsequent leaks are contained
Three Methods of Pleural Adhesion:
| Method | Technique | Notes |
|---|---|---|
| Pleurectomy | Strip parietal pleura from chest wall systematically | Most effective; higher bleeding risk |
| Pleural abrasion | Scourer scrapes off smooth parietal pleural surface | Less morbidity |
| Chemical pleurodesis | Talc insufflated into chest cavity via VATS or ICD | Talc most effective agent |
Chemical Pleurodesis Agents:
| Agent | Dose | Success Rate |
|---|---|---|
| Talc (first choice) | 2–4 g insufflated | 90–95% |
| Tetracycline/Doxycycline | 500 mg in 50 mL saline | 80–85% |
| Bleomycin | 60 units | 70% |
| Silver nitrate | — | 85–90% |
| Minocycline | 300 mg | 75–80% |
Mechanism of pleurodesis: Agent causes chemical pleuritis → intense inflammation → fibrin deposition → pleural symphysis (permanent fusion of visceral and parietal pleura)
Contraindication: Pleurodesis should NOT be performed in young patients with cystic fibrosis or those awaiting lung transplantation (makes future thoracic surgery extremely difficult)
9. MANAGEMENT IN SPECIAL SITUATIONS
Ventilated Patients (ICU)
- High risk of tension pneumothorax due to positive pressure ventilation
- Always insert ICD (needle aspiration insufficient)
- Use smaller Seldinger-technique drains for simple PTX
- Clamping ICD in ventilated patient is contraindicated (risk of tension)
HIV/AIDS Patients with PCP
- SSP with PCP has high recurrence rate (~50%)
- Persistent air leaks common due to necrotic lung tissue
- Early surgical referral; consider pleurodesis early
Pregnant Patients
- Rare; same management principles
- CXR safe in pregnancy (shielded)
- Avoid prolonged hypoxia — fetal risk
- ICD preferred over observation if significant
Bilateral Simultaneous Pneumothorax
- Very rare; life-threatening
- Bilateral ICDs + urgent surgical referral
Haemopneumothorax
- Blood + air in pleural space
- Occurs in 5% of spontaneous PTX (from torn adhesions/vessels)
- Requires large-bore ICD (28–32F)
- Surgery if > 1.5 L blood drained immediately or > 200 mL/hr ongoing
10. COMPLICATIONS
Immediate
| Complication | Notes |
|---|---|
| Tension pneumothorax | Life-threatening; obstructive shock → arrest |
| Hypoxic respiratory failure | Especially in SSP |
| Cardiovascular collapse | Tension → obstructed venous return |
Related to ICD
| Complication | Notes |
|---|---|
| Empyema | Post-drain infection; requires antibiotics ± washout |
| Haemothorax | Injury to intercostal vessels (always go over UPPER border of rib) |
| Lung laceration | If trocar used blindly |
| Subcutaneous emphysema | Air tracks into soft tissue; usually self-limiting |
| Drain misplacement | Into fissure, liver, spleen (abdominal insertion) |
| Drain blockage | Check swinging; flush with saline |
| Drain dislodgement | Resecure; may need reinsertion |
| Neurovascular injury | If inserted below lower border of rib |
Late Complications
| Complication | Notes |
|---|---|
| Recurrence | PSP: 25–30% within 2 years; SSP: 40–80% |
| Chronic/persistent pneumothorax | Air leak > 3 months |
| Re-expansion pulmonary oedema | Rapid re-expansion of chronically collapsed lung; non-cardiogenic pulmonary oedema; treat with O₂ ± diuretics |
| Fibrothorax | Chronic inflammation → pleural fibrosis → restrictive defect |
| Bronchopleural fistula | Persistent communication between bronchus and pleura |
11. PROGNOSIS AND RECURRENCE
| Type | Recurrence Rate | After Surgery |
|---|---|---|
| PSP (first episode) | 25–30% within 2 years | < 5% after VATS pleurodesis |
| PSP (after 2nd episode) | ~50% without surgery | — |
| SSP | 40–80% (disease-dependent) | < 5% after VATS |
| Catamenial | Near 100% without hormonal Rx | Low after VATS + hormonal Rx |
- Most recurrences in PSP occur within 6–24 months
- Risk of contralateral PTX: ~10–15% over lifetime
- PSP mortality: < 0.1%
- SSP mortality: up to 10% (due to underlying disease)
12. PREVENTION AND PATIENT ADVICE
- Smoking cessation — most important preventive measure
- Avoid scuba diving until lung function confirmed normal AND after surgical cure
- Avoid unpressurized air travel for at least 1 week (BTS: wait for full resolution; most airlines recommend 6 weeks post-pneumothorax before flying)
- Avoid vigorous Valsalva manoeuvres (heavy weight-lifting, playing brass instruments)
- Alert future healthcare providers to previous PTX history (risk of re-expansion during any positive pressure ventilation)
- Follow-up CXR to confirm complete re-expansion before return to activity
13. HIGH-YIELD EXAM SUMMARY TABLE
| Topic | Key Fact |
|---|---|
| Definition | Air in pleural space → lung collapse |
| Most common cause of PSP | Ruptured apical subpleural blebs |
| Most common cause of SSP | COPD/emphysema |
| Most common iatrogenic cause | Central venous catheter insertion |
| M:F ratio in PSP | 6:1 |
| Typical PSP patient | Tall, thin, young male, smoker |
| Tension PTX mechanism | Ball-valve → rising intrapleural pressure |
| Tension PTX emergency Rx | Needle decompression: 2nd ICS, MCL, 14–16G |
| ICD insertion site | 5th ICS, anterior axillary line (triangle of safety) |
| Breath sounds in PTX | Absent/diminished ipsilaterally |
| Percussion in PTX | Hyper-resonance |
| Tracheal deviation | Away from affected side (in tension) |
| CXR: small vs large | < 2 cm vs ≥ 2 cm rim at hilum |
| Ultrasound sign of PTX | Absent lung sliding; barcode/stratosphere sign |
| First-line Rx for large PSP | Needle aspiration |
| Direct ICD for SSP | Yes (no aspiration) |
| Surgical indication | 2nd ipsilateral, bilateral, occupational risk, persistent air leak |
| Surgery type | VATS + bullectomy + pleurodesis |
| Best chemical pleurodesis agent | Talc (90–95% success) |
| Pleurodesis methods | Pleurectomy, pleural abrasion, chemical |
| Recurrence without surgery | 25–30% (PSP), 40–80% (SSP) |
| Catamenial PTX | Right-sided; associated with thoracic endometriosis |
| Re-expansion pulmonary oedema | Non-cardiogenic; rapid re-expansion of chronic PTX |
| Flying after PTX | Avoid for at least 1 week (most say 6 weeks) |
| Pleurodesis contraindicated in | Pre-transplant patients, cystic fibrosis |
References: Bailey & Love's Short Practice of Surgery, 28th Edition, pp. 395, 999, 1002; BTS Guidelines for the Management of Spontaneous Pneumothorax (2010, updated 2023); Harrison's Principles of Internal Medicine, 21st Edition; Schwartz's Principles of Surgery, 11th Edition.
This is a shared conversation. Sign in to Orris to start your own chat.