MEN Syndromes 2. Oral GTT (indications, interpretation of result) 3. Tumors of Thyroid - classify, Colloid Goitre ( 4. Glycosylated Hemoglobin 5. Hashimoto's Thyroiditis - gross, morphologic features, complications 1. Diabetes Mellitus - diagnostic criteria*, Diabetic Gloerulosclerosis - pathogenesis, morphology; Diabetic Nephropathy () 2. Oral GTT - indications, method, interpretation 3. Diabetes Mellitus*** - laboratory investigations**; etiology, classification; Investigations with their significance; Classify* answer in detail covering imp points as welll in exaam point of view 2mbbs pathology refer harsh moham add diagrams as well cover required points for muhs exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Here are your complete, exam-oriented MUHS 2nd MBBS Pathology notes covering all the topics. Sourced from Robbins Pathology, Harrison's, and Clinical Pathology references.
2nd MBBS Pathology - MUHS Exam Notes
Endocrine Pathology: Diabetes, Thyroid & MEN Syndromes
1. DIABETES MELLITUS ★★★
Classification (WHO / ADA)
DIABETES MELLITUS
├── Type 1 DM (5-10%) - Absolute insulin deficiency
│ ├── 1A: Immune-mediated (HLA-DR3, HLA-DR4)
│ └── 1B: Idiopathic
├── Type 2 DM (90-95%) - Insulin resistance + relative deficiency
├── Gestational DM
└── Other Specific Types
├── MODY (Maturity Onset DM of Young) - Autosomal dominant
│ ├── MODY1: HNF4A mutation
│ ├── MODY2: Glucokinase (GCK) mutation
│ └── MODY3: HNF1A mutation (most common)
├── Diseases of exocrine pancreas
│ (Pancreatitis, CF, Hemochromatosis, Neoplasia)
├── Endocrinopathies
│ (Acromegaly, Cushing's, Glucagonoma, Pheochromocytoma)
├── Drug/Chemical-induced (Steroids, Thiazides, Pentamidine)
├── Infections (Congenital Rubella, CMV, Coxsackievirus)
└── Genetic syndromes (Down, Klinefelter, Turner syndromes)
Type 1 vs Type 2 - Key Comparison
| Feature | Type 1 | Type 2 |
|---|---|---|
| Frequency | 5-10% | 90-95% |
| Age of onset | Children/young adults | Middle-aged (but any age) |
| Pathogenesis | Autoimmune beta cell destruction | Insulin resistance + secretory defect |
| Autoantibodies | GAD65, IA-2, IAA, ZnT8 | Absent |
| C-peptide | Very low/undetectable | Detectable |
| Body type | Normal/thin | Often obese |
| Ketoacidosis | Common | Rare |
| Treatment | Insulin mandatory | Oral agents, then insulin |
| HLA association | DR3, DR4 | No strong HLA link |
Etiology/Pathogenesis
Type 1 DM:
- Genetic: HLA-DR3 and HLA-DR4 (95% of Type 1 patients carry one or both)
- Environmental trigger (viral infection, dietary factors) in genetically susceptible individual
- Autoimmune destruction of beta cells by:
- CD8+ cytotoxic T cells (direct killing)
- CD4+ Th1 cells releasing IFN-gamma → macrophage activation
- Autoantibodies (GAD65, IA-2, ZnT8, insulin autoantibodies)
- Progressive "insulitis" - lymphocytic infiltration of islets
- Loss of >90% of beta cell mass → absolute insulin deficiency
Type 2 DM:
- Insulin resistance (muscle, liver, adipose tissue) - primary defect
- Progressive beta cell dysfunction (exhaustion, glucotoxicity, lipotoxicity)
- Genetic predisposition (polygenic) + environmental factors (obesity, sedentary lifestyle)
- Glucotoxicity and lipotoxicity cause beta cell apoptosis over time
Diagnostic Criteria (ADA) ★★★
┌─────────────────────────────────────────────────────────────┐
│ DIAGNOSTIC CRITERIA FOR DM │
│ │
│ 1. FPG ≥ 126 mg/dL (7.0 mmol/L) — fasting ≥8 hrs │
│ 2. 2-hr PG ≥ 200 mg/dL during OGTT (75g glucose) │
│ 3. HbA1c ≥ 6.5% (48 mmol/mol) │
│ 4. Random PG ≥ 200 mg/dL + classic symptoms │
│ (polyuria, polydipsia, unexplained weight loss) │
│ │
│ NOTE: Criteria 1-3 require confirmation on repeat │
│ testing on a different day (unless unequivocal) │
└─────────────────────────────────────────────────────────────┘
Pre-Diabetes:
- Impaired Fasting Glucose (IFG): FPG 100-125 mg/dL
- Impaired Glucose Tolerance (IGT): 2-hr OGTT 140-199 mg/dL
- HbA1c 5.7-6.4%
Laboratory Investigations with Significance ★★
| Investigation | Normal | Significance |
|---|---|---|
| FPG (Fasting Plasma Glucose) | <100 mg/dL | Screening and diagnosis |
| OGTT 2-hr glucose | <140 mg/dL | Gold standard for diagnosis; mandatory in GDM |
| HbA1c | <5.7% | Reflects 3-month average glucose; monitoring control |
| Random blood glucose | <140 mg/dL | Screening; diagnosis if ≥200 + symptoms |
| Urine glucose | Negative | Not for diagnosis (renal threshold varies) |
| Serum C-peptide | 0.5-2.0 ng/mL | Distinguishes Type 1 (low) from Type 2 (normal/high) |
| Insulin levels | 5-20 µIU/mL | Low in T1DM; normal/high in early T2DM |
| Autoantibodies (GAD65, IA-2) | Negative | Confirm autoimmune (Type 1) DM |
| Serum ketones / Urine ketones | Negative | Diabetic ketoacidosis monitoring |
| Lipid profile | - | Dyslipidemia: ↑TG, ↓HDL, ↑LDL |
| Renal function / Urine microalbumin | <30 mg/day | Early nephropathy (microalbuminuria 30-300 mg/day) |
| Urine ACR (albumin:creatinine ratio) | <30 mg/g | >30 = microalbuminuria; >300 = macroalbuminuria |
| Serum creatinine/eGFR | - | Nephropathy staging |
| Urine NAG enzyme | - | Early tubular damage marker |
2. ORAL GLUCOSE TOLERANCE TEST (OGTT) ★★
Indications
INDICATIONS FOR OGTT
├── Diagnosis of GDM (Gestational Diabetes Mellitus) - PRIMARY use
├── Borderline fasting glucose (IFG: 100-125 mg/dL)
├── Suspected DM when FPG is normal but symptoms present
├── Reactive hypoglycemia evaluation
├── Diagnosis of IGT (Impaired Glucose Tolerance)
├── Follow-up of women with previous GDM
└── Screening in high-risk individuals (PCO, obesity, family history)
Method (Standard 75g OGTT)
PREPARATION (3 days before):
• Unrestricted diet (≥150g carbohydrate/day)
• Normal physical activity
• No drugs affecting glucose metabolism
PROCEDURE:
Day of test → 8-12 hours overnight fast
↓
Fasting blood sample drawn (baseline)
↓
75g anhydrous glucose dissolved in 250-300 mL water
(For GDM: 100g glucose used in some protocols)
↓
Patient rests (no smoking, eating, vigorous activity)
↓
Blood sample at 1 hour (optional)
↓
Blood sample at 2 hours
NOTE: In pregnancy, samples taken at 0, 1, 2, 3 hours (Carpenter & Coustan criteria)
Interpretation
Standard OGTT (75g) - Non-pregnant adults:
| Result | Fasting | 2-hr Post-load |
|---|---|---|
| Normal | <100 mg/dL | <140 mg/dL |
| IFG | 100-125 mg/dL | - |
| IGT | - | 140-199 mg/dL |
| Diabetes Mellitus | ≥126 mg/dL | ≥200 mg/dL |
OGTT in Pregnancy (GDM Screening - IADPSG criteria, 75g):
| Threshold | Value |
|---|---|
| Fasting | ≥92 mg/dL |
| 1-hour | ≥180 mg/dL |
| 2-hour | ≥153 mg/dL |
One abnormal value is sufficient for GDM diagnosis (IADPSG/WHO)
OGTT in Pregnancy (Carpenter & Coustan criteria, 100g) - used in USA:
| Time | Threshold |
|---|---|
| Fasting | ≥95 mg/dL |
| 1-hour | ≥180 mg/dL |
| 2-hour | ≥155 mg/dL |
| 3-hour | ≥140 mg/dL |
Two or more values must be met or exceeded
3. GLYCOSYLATED HEMOGLOBIN (HbA1c) ★★
Definition
HbA1c is hemoglobin to which glucose has been non-enzymatically and irreversibly attached (glycated) to the N-terminal valine of the beta chain of hemoglobin A.
Key Points
┌──────────────────────────────────────────────────────────┐
│ HbA1c FACTS │
│ │
│ • Reflects AVERAGE blood glucose over 2-3 months │
│ (reflects lifespan of RBCs ~120 days) │
│ • Measured as % of total hemoglobin │
│ • Formula: Average Glucose (mg/dL) = (28.7 × HbA1c) - 46.7 │
│ │
│ NORMAL: <5.7% │
│ PRE-DIABETES: 5.7-6.4% │
│ DIAGNOSTIC OF DM: ≥6.5% │
│ TARGET IN TREATED DM: <7% │
└──────────────────────────────────────────────────────────┘
Methods of Measurement
- High-Performance Liquid Chromatography (HPLC) - gold standard
- Immunoassay
- Affinity chromatography
- Ion-exchange chromatography
Factors Causing False Results
| False LOW HbA1c | False HIGH HbA1c |
|---|---|
| Hemolytic anemia (shortened RBC lifespan) | Iron deficiency anemia |
| Sickle cell disease | Vitamin B12/folate deficiency |
| Recent blood transfusion | Uremia (carbamylated Hb interferes) |
| Splenomegaly | Alcoholism |
| Pregnancy | Asplenia |
4. DIABETIC NEPHROPATHY / GLOMERULOSCLEROSIS ★★★
Pathogenesis
HYPERGLYCEMIA
│
├── ↑ Advanced Glycation End Products (AGEs)
│ → Cross-links collagen → GBM thickening
│ → Binds RAGE receptor → TGF-β, VEGF upregulation
│
├── Activation of Protein Kinase C (PKC)
│ → ↑ VEGF, TGF-β → mesangial expansion
│
├── Polyol pathway activation
│ (Glucose → Sorbitol via aldose reductase)
│ → Osmotic damage to cells
│
├── Hemodynamic changes
│ → Afferent arteriole dilation > efferent
│ → ↑ Intraglomerular pressure (hyperfiltration)
│ → GFR initially ↑ (hyperfiltration phase)
│
└── TGF-β overproduction
→ Mesangial matrix expansion
→ Basement membrane thickening
→ Fibrosis
Key molecules: TGF-β, VEGF, IGF-1, EGF, PDGF, Ang II, AGEs, ROS (Nox4)
Podocyte injury: Ang II and TGF-β trigger podocyte apoptosis → proteinuria. Neuropilin-1 suppression by AGEs reduces podocyte adhesion and migration.
Glomerular Basement Membrane: Type IV collagen accumulation + loss of heparin sulfate proteoglycan (negative charge) → proteinuria.
Morphology (Glomerular Lesions) ★★★
Two main types of diabetic glomerulosclerosis:
A. Diffuse Glomerulosclerosis (More Common)
- Diffuse increase in mesangial matrix and basement membrane thickening
- All glomeruli affected
- Early lesion; associated with microalbuminuria
B. Nodular Glomerulosclerosis (PATHOGNOMONIC) ★★★
- Kimmelstiel-Wilson lesion - ovoid/spherical deposits of laminated matrix in the periphery of the glomerulus
- PAS-positive, acellular nodules in the mesangium
- Nodule pushes capillaries to periphery
- Present in ~25% of patients
- Pathognomonic of diabetic nephropathy (but similar pattern in amyloidosis, light-chain deposition disease)
Other Morphologic Features:
- Exudative lesions: "Capsular drop" (accumulation between parietal epithelium and Bowman's capsule) and "fibrin cap" (hyaline deposits overlying peripheral capillaries)
- Glomerular basement membrane (GBM) thickening
- Afferent AND efferent arteriolar hyalinosis (hyalinosis of efferent arteriole is virtually DIAGNOSTIC of DM)
- Tubular lesions: Armanni-Ebstein lesion (glycogen accumulation in tubular epithelium, especially in renal medulla)
- Interstitial fibrosis and tubular atrophy (IFTA) in advanced disease
Stages of Diabetic Nephropathy (Mogensen Stages):
Stage I: Hyperfiltration - ↑GFR, kidney enlargement, no albuminuria
Stage II: Silent - GBM thickening, mesangial expansion; normal urine
Stage III: Incipient nephropathy - MICROALBUMINURIA (30-300 mg/day); BP rises
Stage IV: Overt nephropathy - MACROALBUMINURIA (>300 mg/day); declining GFR
Stage V: End-stage renal disease (ESRD) - GFR <15 mL/min; dialysis needed
5. MEN SYNDROMES (Multiple Endocrine Neoplasia) ★★
Overview
MEN syndromes are hereditary disorders caused by genetic mutations leading to tumors in multiple endocrine organs.
┌──────────────────┬────────────────────────────────────────────────────┐
│ SYNDROME │ KEY FEATURES │
├──────────────────┼────────────────────────────────────────────────────┤
│ MEN 1 │ "3 P's" - Parathyroid + Pancreas + Pituitary │
│ (Wermer's) │ Gene: MEN1 (Chromosome 11q13) - MENIN protein │
│ │ Tumor suppressor - Autosomal Dominant │
│ │ Parathyroid: ~100% (most common, first to appear) │
│ │ Pancreatic NETs: Gastrinoma > Insulinoma │
│ │ Pituitary: Prolactinoma > GH-oma > ACTH-oma │
│ │ Also: Carcinoid, Lipomas, Angiofibromas │
├──────────────────┼────────────────────────────────────────────────────┤
│ MEN 2A │ MTC + Pheochromocytoma + Hyperparathyroidism │
│ (Sipple's) │ Gene: RET proto-oncogene (Chr 10) - gain of function│
│ │ MTC: 95-100% (often first manifestation) │
│ │ Pheo: 50% │
│ │ PHPT: 20-30% │
├──────────────────┼────────────────────────────────────────────────────┤
│ MEN 2B │ MTC + Pheochromocytoma + Mucosal Neuromas │
│ │ Gene: RET (specific codon 918 mutation) │
│ │ + Marfanoid habitus + Ganglioneuromatosis of GIT │
│ │ Most aggressive MTC (NO hyperparathyroidism) │
├──────────────────┼────────────────────────────────────────────────────┤
│ MEN 4 │ MEN1-like phenotype │
│ │ Gene: CDKN1B (p27 cyclin-dependent kinase inhibitor)│
│ │ Parathyroid + Pituitary + PNET (like MEN1) │
└──────────────────┴────────────────────────────────────────────────────┘
Genetics Summary:
- MEN1: MEN1 gene (11q13) - encodes menin (tumor suppressor) - "2-hit hypothesis" (Knudson)
- MEN2A/2B: RET proto-oncogene (10q11.2) - gain-of-function mutation
- MEN4: CDKN1B gene
Zollinger-Ellison Syndrome (in MEN1):
- Gastrinoma of pancreas/duodenum → hypergastrinemia → peptic ulcers
- Treated with PPIs + surgical resection
6. THYROID TUMORS - CLASSIFICATION ★★
Classification of Thyroid Tumors (WHO)
THYROID TUMORS
│
├── A. BENIGN
│ └── Follicular Adenoma (most common benign thyroid tumor)
│ ├── Simple/Normofollicular adenoma
│ ├── Macrofollicular (colloid) adenoma
│ ├── Microfollicular (fetal) adenoma
│ ├── Embryonal (trabecular) adenoma
│ └── Hurthle cell (oxyphilic/oncocytic) adenoma
│
└── B. MALIGNANT (Thyroid Carcinomas)
│
├── EPITHELIAL (from follicular cells)
│ ├── Differentiated
│ │ ├── Papillary Carcinoma (most common ~85%)
│ │ └── Follicular Carcinoma (~10%)
│ ├── Poorly Differentiated Carcinoma
│ └── Undifferentiated/Anaplastic Carcinoma (~1-2%, worst prognosis)
│
├── C-CELL ORIGIN
│ └── Medullary Carcinoma (~5%) - secretes Calcitonin + Amyloid
│
└── OTHERS
├── Primary Thyroid Lymphoma (B-cell, associated with Hashimoto's)
└── Metastatic (from breast, lung, renal cell carcinoma)
Papillary Carcinoma (Most Common)
- Genetics: BRAF V600E mutation (most common), RET/PTC rearrangement
- Gross: Irregular, white, firm, non-encapsulated; may be cystic; "ground glass" or stippled calcification (psammoma bodies)
- Histology:
- Papillary architecture (finger-like projections with fibrovascular core)
- Orphan Annie eye nuclei - ground-glass, "Optically clear" nuclei with nuclear grooves and inclusions (PATHOGNOMONIC)
- Psammoma bodies (concentrically laminated calcifications) - in 40-50%
- Lymphatic invasion and cervical lymph node metastasis (common)
- Prognosis: Excellent (>98% 10-year survival); spreads to lymph nodes but rarely blood
Follicular Carcinoma
- Genetics: RAS mutations, PAX8-PPARG fusion (translocation)
- Gross: Encapsulated with capsular and/or vascular invasion (differentiates from adenoma)
- Histology: Follicles of varying size; capsular invasion and/or vascular invasion required for diagnosis
- Spread: Hematogenous (to lung, bone, liver) - NOT lymphatic
- Hurthle cell carcinoma - variant with oxyphilic cells
Medullary Carcinoma (MTC)
- Origin: Parafollicular C cells (neuroendocrine)
- Genetics: RET mutation (sporadic and familial/MEN2)
- Gross: Solitary nodule (sporadic); Bilateral/multicentric (syndromic/MEN2)
- Histology:
- Polygonal/spindle cells in nests and trabeculae
- Amyloid stroma (derived from calcitonin polypeptides) - Congo red positive
- Neurosecretory granules on EM
- Markers: Calcitonin (serum marker), CEA, Chromogranin A
- Prognosis: Intermediate (better than anaplastic, worse than papillary)
Anaplastic Carcinoma
- Most aggressive thyroid malignancy; rare but deadly
- Undifferentiated cells, spindle cells, giant cells
- No radioiodine uptake; no effective treatment
- Median survival: 3-6 months
COLLOID GOITRE (Multinodular Goitre / Follicular Nodular Disease) ★★
Definition: Diffuse or nodular enlargement of the thyroid due to repeated cycles of stimulation and involution, without significant inflammation or neoplasia.
Pathogenesis:
Iodine deficiency / ↑TSH → Follicular hyperplasia
↓
Colloid accumulation when TSH falls → Involution
↓
Repeated cycles of hyperplasia and involution
↓
Nodule formation (some cells more responsive than others - polyclonal)
↓
Multinodular Goitre (Colloid Goitre)
Types:
- Diffuse Non-toxic Goitre - uniform enlargement, often in endemic iodine-deficient areas (endemic goitre)
- Multinodular Goitre (MNG) - multiple nodules; most common cause of thyroid enlargement in adults
Gross Morphology:
- Markedly enlarged thyroid (can reach enormous size - >100g; normal ~25g)
- Multiple nodules of varying size
- Cut section: colloid-filled distended follicles (glistening, brown/tan)
- Areas of hemorrhage, fibrosis, cystic change, and calcification
- Nodules compressed by fibrous septae
Histological Morphology:
- Markedly enlarged follicles distended with colloid ("colloid" goitre)
- Follicular epithelium: flattened (involuted) to hyperplastic (cuboidal/columnar)
- Areas of "resorption vacuoles" (Sanderson's polsters) - scalloped colloid at edges of follicles
- Fibrous septae separating nodules
- Focal hemorrhage, hemosiderin deposits, dystrophic calcification
- Papillary projections may mimic papillary carcinoma (but no nuclear features of malignancy)
Clinical Features:
- Usually euthyroid
- Pressure effects: dysphagia, stridor, dyspnea, Pemberton's sign
- Rarely: hyperthyroidism (toxic MNG = Plummer's disease)
- Risk of malignancy: low but present (particularly papillary carcinoma)
7. HASHIMOTO'S THYROIDITIS ★★★
Source: Robbins Pathology (9780443264528)
Introduction
- Most common cause of hypothyroidism in iodine-sufficient areas
- Autoimmune destruction of the thyroid gland
- Female:Male = 10:1 to 20:1
- Age: 45-65 years (most common), but also affects children
- Originally described by Hashimoto in 1912 as "struma lymphomatosa"
Pathogenesis
Breakdown of self-tolerance to thyroid autoantigens → autoimmune thyroid destruction
Autoantibodies present:
- Anti-thyroglobulin antibodies
- Anti-thyroid peroxidase (TPO) antibodies (microsomal antibodies) - most sensitive marker
Mechanisms of thyroid cell death:
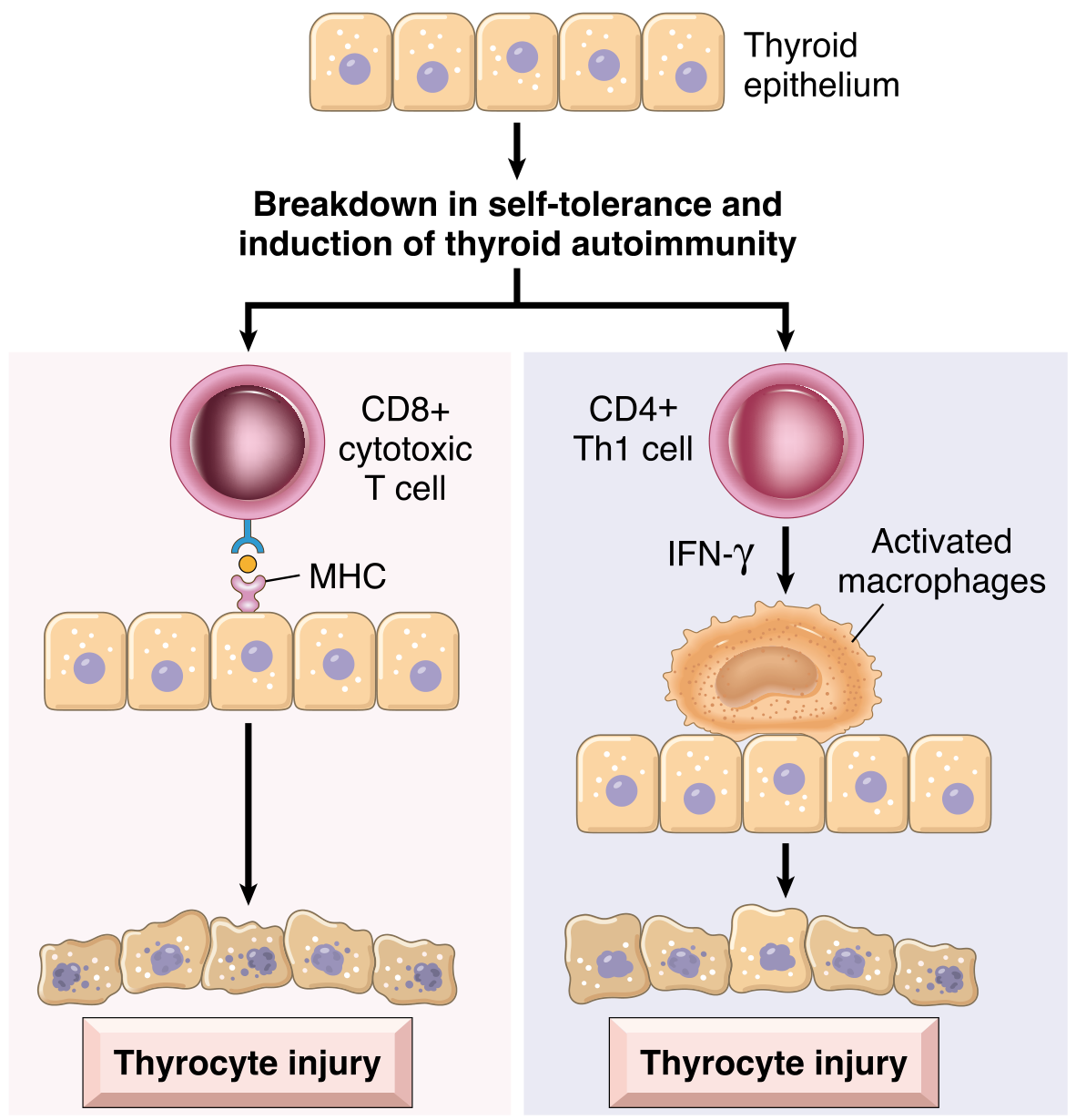
Fig. Pathogenesis of Hashimoto thyroiditis: CD8+ T cells directly kill thyrocytes via MHC recognition; CD4+ Th1 cells release IFN-γ activating macrophages causing thyrocyte injury.
1. CD8+ cytotoxic T cells → direct cell-mediated killing of thyrocytes
2. CD4+ Th1 cells → IFN-γ release → macrophage activation → thyroid damage
3. Anti-TPO and anti-thyroglobulin antibodies → complement-dependent
cytotoxicity + ADCC (antibody-dependent cell-mediated cytotoxicity)
4. Genetic susceptibility: CTLA-4, PTPN22, IL2RA polymorphisms
Gross Morphology
- Thyroid: diffusely enlarged (symmetric)
- Well demarcated from adjacent structures (no invasion - differentiates from Reidel's thyroiditis)
- Cut surface: pale, yellow-tan, firm, somewhat nodular
Microscopic / Histological Features ★★★
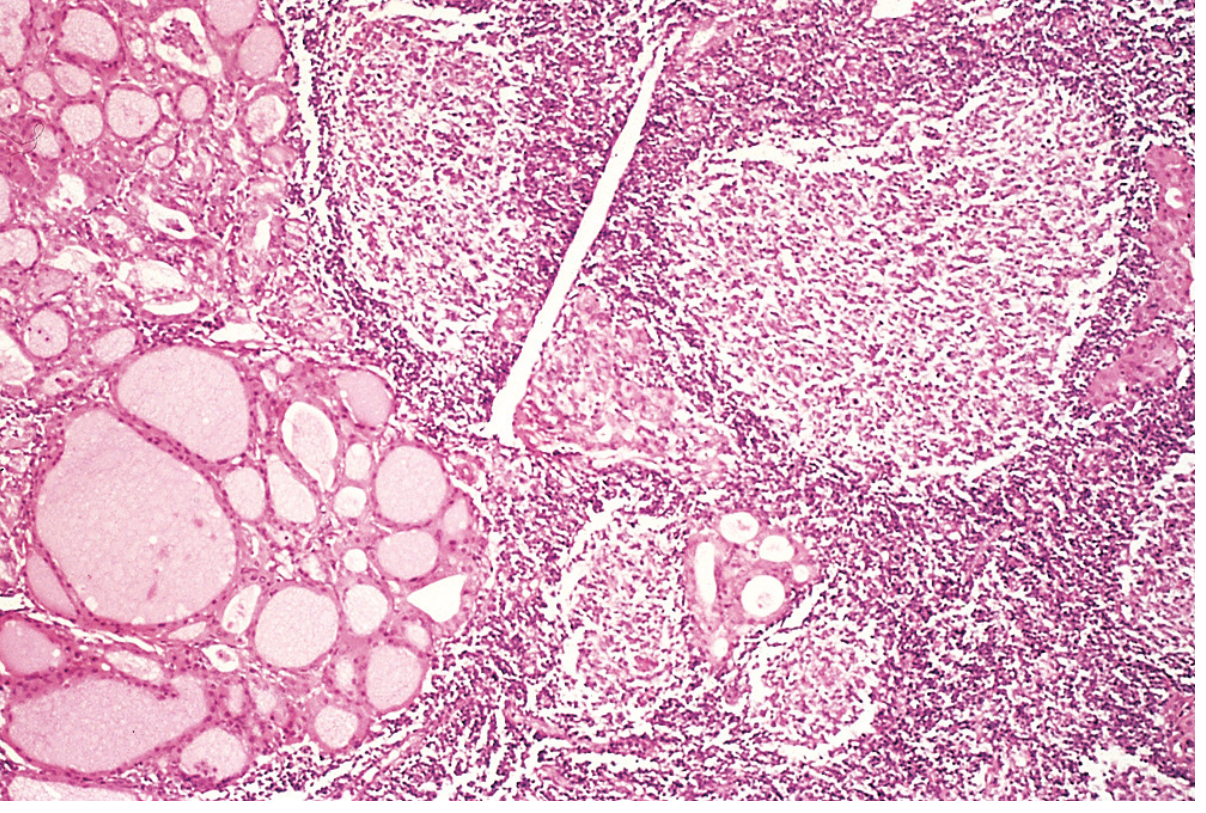
Fig. Hashimoto thyroiditis: Dense lymphocytic infiltrate with germinal centers (right). Residual thyroid follicles lined by eosinophilic oncocytic (Hurthle) cells (left).
- Diffuse lymphocytic infiltration - small lymphocytes, plasma cells
- Lymphoid follicles with well-developed germinal centers (hallmark)
- Atrophic thyroid follicles - small, reduced colloid
- Hurthle cell (oncocytic/oxyphilic) metaplasia - follicular epithelium replaced by cells with abundant eosinophilic granular cytoplasm (mitochondria-rich) - represents metaplastic response to chronic injury
- Interstitial fibrosis - increased connective tissue (does NOT extend beyond gland capsule - unlike Reidel's)
FNA (Fine Needle Aspiration) findings:
- Hurthle cells + heterogeneous population of lymphocytes = characteristic of Hashimoto's
Clinical Features
- Painless enlargement of thyroid (may be asymmetric initially)
- Gradual development of hypothyroidism (T3, T4 ↓; TSH ↑ compensatory)
- "Hashitoxicosis" - transient thyrotoxicosis initially (due to follicle disruption and hormone release)
- Lab: Anti-TPO antibodies (positive in >95%); Anti-thyroglobulin antibodies
Complications ★★
┌─────────────────────────────────────────────────────────┐
│ COMPLICATIONS OF HASHIMOTO'S │
│ │
│ 1. HYPOTHYROIDISM (most common outcome) │
│ 2. Increased risk of PRIMARY THYROID LYMPHOMA │
│ (Extranodal marginal zone B-cell lymphoma - MALT) │
│ 3. Other autoimmune diseases: │
│ - Endocrine: Type 1 DM, Autoimmune adrenalitis │
│ - Non-endocrine: SLE, Myasthenia gravis, Sjögren's │
│ 4. Possible increased risk of PAPILLARY CARCINOMA │
│ (controversial but some evidence supports this) │
│ 5. Hashitoxicosis (transient, early) │
└─────────────────────────────────────────────────────────┘
QUICK REVISION DIAGRAM SUMMARIES
DM Complications (for context with nephropathy)
DIABETES MELLITUS
│
Chronic Hyperglycemia
│
┌───┴────────────────────────────────────────┐
│ │
Microvascular Macrovascular
(small vessel disease) (large vessel disease)
│ │
├── Diabetic Nephropathy ├── Coronary artery disease
│ (Kimmelstiel-Wilson lesions) ├── Peripheral arterial disease
├── Diabetic Retinopathy └── Cerebrovascular disease
│ (dot-blot hemorrhages, microaneurysms)
└── Diabetic Neuropathy
(Peripheral > Autonomic)
MEN Syndromes Quick Diagram
MEN1 (Wermer's) MEN2A (Sipple's) MEN2B
MEN1 gene (11q13) RET gene (10q11) RET gene (codon 918)
Menin protein Proto-oncogene Proto-oncogene
(Tumor suppressor) (Gain of function) (Gain of function)
│ │ │
Parathyroid (100%) Medullary Thyroid Ca Medullary Thyroid Ca
Pancreatic NETs Pheochromocytoma Pheochromocytoma
Pituitary adenoma Hyperparathyroidism Mucosal Neuromas
(Gastrinoma=ZES) Marfanoid habitus
(Insulinoma) No PHPT
EXAM HIGH-YIELD POINTS (MUHS Focus)
| Topic | Most Important Point |
|---|---|
| DM Diagnosis | FPG ≥126, OGTT ≥200, HbA1c ≥6.5%, Random ≥200+symptoms |
| DM Type 1 vs 2 | Autoimmune vs insulin resistance; C-peptide absent vs present |
| OGTT | Fasting 8h, 75g glucose, sample at 0+2h; GDM=IADPSG (any 1 abnormal) |
| HbA1c | 3-month average; HPLC method; target <7%; false low in hemolysis |
| Diabetic Nephropathy | Kimmelstiel-Wilson nodules (pathognomonic); efferent arteriolar hyalinosis (virtually diagnostic) |
| Hashimoto's | Anti-TPO antibodies; Hurthle cells + lymphocytic infiltrate; most common hypothyroid cause |
| MEN1 | 3P: Parathyroid+Pancreas+Pituitary; MEN1 gene; autosomal dominant |
| MEN2A | MTC+Pheo+PHPT; RET gene |
| Papillary Carcinoma | Orphan Annie nuclei + Psammoma bodies; most common thyroid Ca; BRAF mutation |
| Medullary Carcinoma | C-cells; Calcitonin marker; amyloid stroma; RET mutation; MEN2 |
| Colloid Goitre | Distended follicles + colloid; Scalloped resorption vacuoles; fibrous septae |
Sources: Robbins & Cotran Pathologic Basis of Disease (10th Ed.), Harrison's Principles of Internal Medicine (22E), Henry's Clinical Diagnosis and Management by Laboratory Methods, Comprehensive Clinical Nephrology (7th Ed.), Sabiston Textbook of Surgery.
Add histo pathology diagram and gross as well
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have all the images needed. Here is the complete, fully illustrated update with all gross and histopathology diagrams embedded:
Histopathology & Gross Diagrams - MUHS Pathology Notes
(Additions to previous notes - All images from Robbins Pathology)
COLLOID GOITRE (Multinodular / Follicular Nodular Disease) - Gross & Histo
Gross Morphology
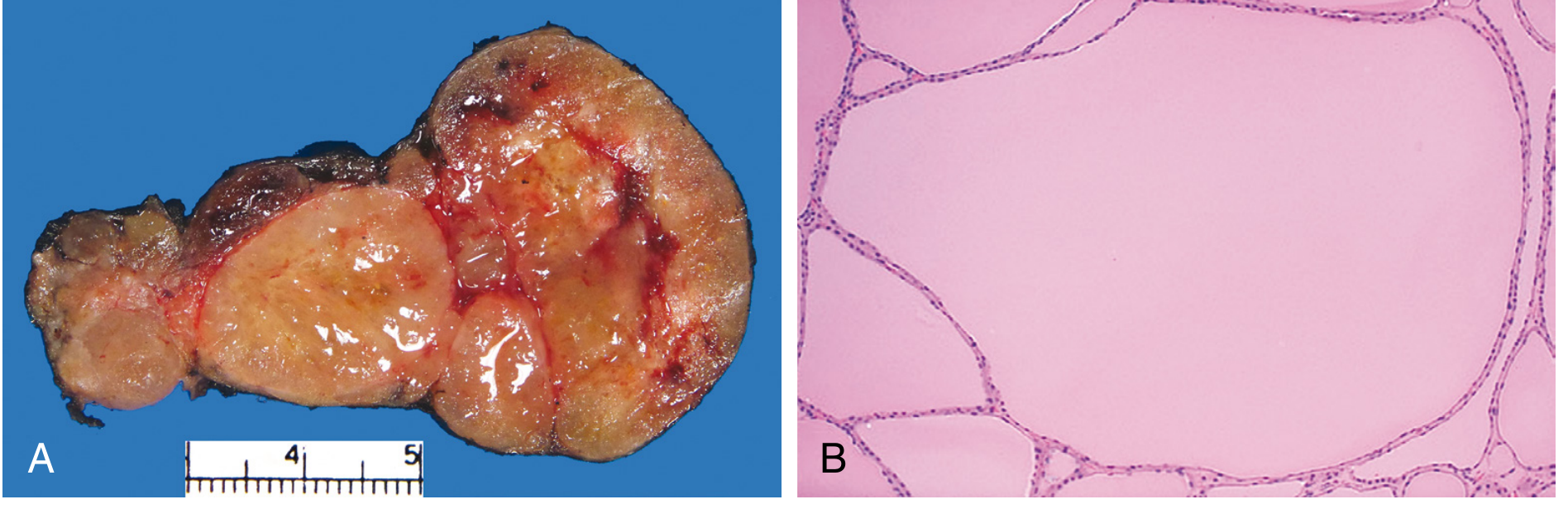
Fig. Follicular Nodular Disease (Colloid Goitre)
- (A) GROSS: Cut surface shows tan, glistening, gelatinous (colloid-rich) nodules of varying sizes. Note areas of dark hemorrhage and brown/orange coloration due to hemosiderin.
- (B) HISTO: Markedly enlarged follicles filled with abundant pale pink colloid. Follicular lining epithelium is flattened and inactive (low cuboidal). Large follicles with scalloped edges (resorption vacuoles - Sanderson's polsters) are visible.
What to note in the microscope:
- Follicles greatly distended with colloid (pale pink, PAS+)
- Lining epithelium: FLAT / LOW CUBOIDAL (inactive)
- Scalloped/vacuolated colloid margins (resorption vacuoles)
- Fibrous septae separating nodules
- No capsule between nodules (unlike follicular adenoma)
- Areas of old hemorrhage, hemosiderin, calcification
HASHIMOTO'S THYROIDITIS - Gross & Histo
Pathogenesis Diagram
Fig. Pathogenesis of Hashimoto Thyroiditis - Two main immune mechanisms: (Left) CD8+ cytotoxic T cells recognize thyroid antigens via MHC and directly kill thyrocytes. (Right) CD4+ Th1 cells release IFN-γ which activates macrophages causing inflammatory thyroid damage.
Histology
Fig. Hashimoto Thyroiditis - H&E section (Robbins Pathology)
Annotated features to identify in exam:
LEFT SIDE of image:
- Residual thyroid follicles (atrophic, small)
- Hurthle cells (oncocytes): follicular epithelium replaced by
cells with abundant BRIGHT PINK GRANULAR cytoplasm
(due to mitochondrial accumulation - metaplastic response)
- Colloid: reduced or absent
RIGHT SIDE of image:
- Dense LYMPHOCYTIC INFILTRATE replacing parenchyma
- GERMINAL CENTERS (secondary lymphoid follicles) -
HALLMARK of Hashimoto's, distinguishes from normal
- Plasma cells
- Increased interstitial fibrosis (pale areas between follicles)
Key histological triad to write in exam:
- Dense lymphocytic infiltration with germinal center formation
- Hurthle cell (oxyphilic/oncocytic) metaplasia of follicular epithelium
- Atrophic follicles + interstitial fibrosis
PAPILLARY CARCINOMA OF THYROID - Gross & Histo ★★★
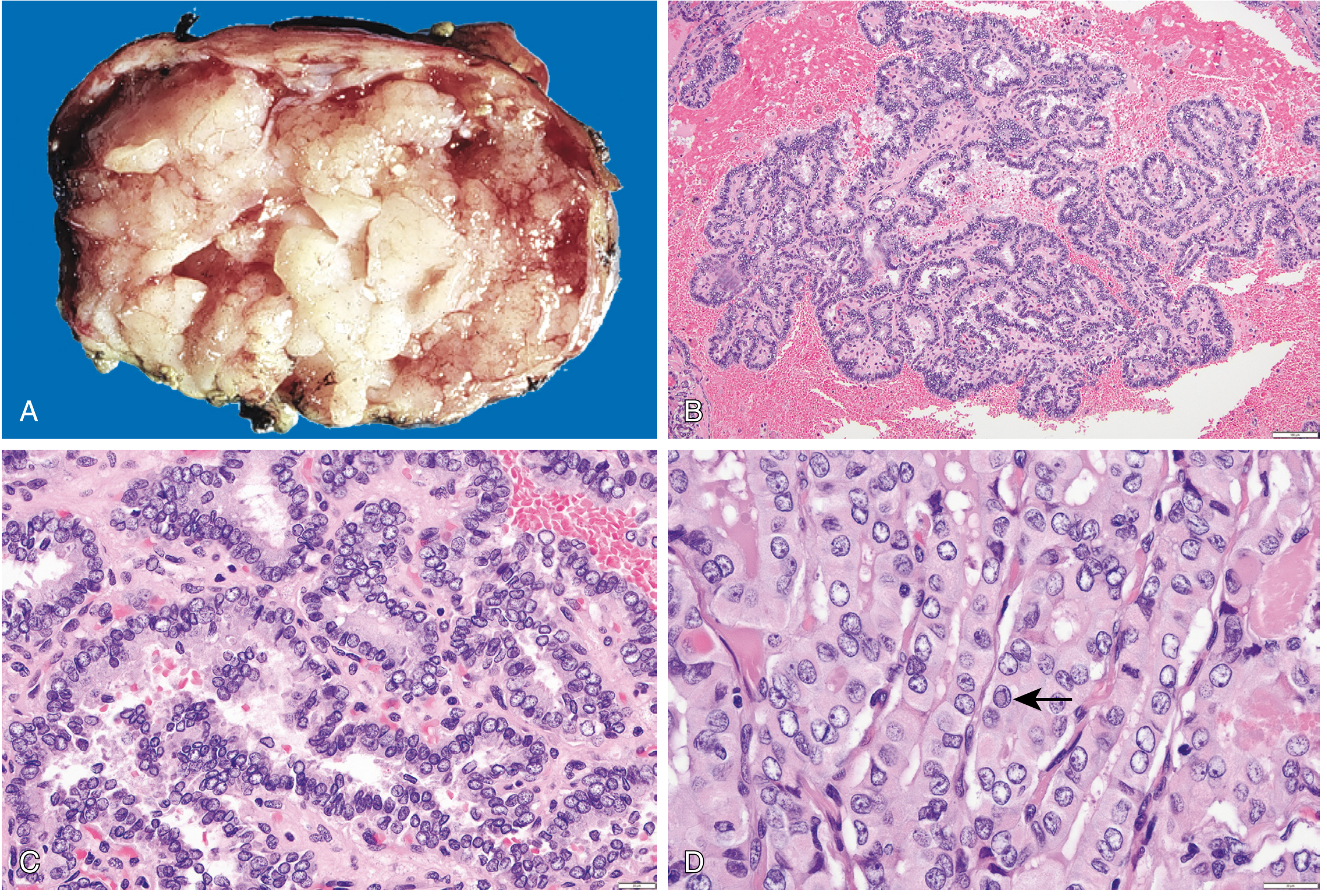
Fig. 24.19 Papillary Carcinoma of the Thyroid (Robbins)
Panel-by-panel breakdown for exam:
| Panel | What you see | Significance |
|---|---|---|
| (A) GROSS | White, firm, irregular nodule; papillary structures visible; may be cystic | Non-encapsulated, infiltrative appearance |
| (B) LOW POWER | Branching papillae with fibrovascular cores; complex architecture | Classic papillary pattern - key diagnostic feature |
| (C) HIGH POWER | Cells with pale/empty ground-glass nuclei, nuclear crowding and overlap | "ORPHAN ANNIE EYE" nuclei - PATHOGNOMONIC |
| (D) HIGH POWER | Nucleus containing a round cytoplasmic inclusion (arrow) | INTRANUCLEAR PSEUDOINCLUSION - pathognomonic |
Critical Microscopic Features to Write:
1. PAPILLAE: Branching finger-like projections with fibrovascular stalks
2. ORPHAN ANNIE EYE NUCLEI: Ground-glass, optically clear, pale nuclei
3. NUCLEAR GROOVES: "Coffee bean" shaped nuclei
4. INTRANUCLEAR PSEUDOINCLUSIONS: cytoplasm pushed into nucleus
5. PSAMMOMA BODIES: Concentric laminated calcifications (40-50% cases)
6. LYMPHATIC INVASION (not blood vessel invasion)
FOLLICULAR CARCINOMA - Gross & Histo
Gross
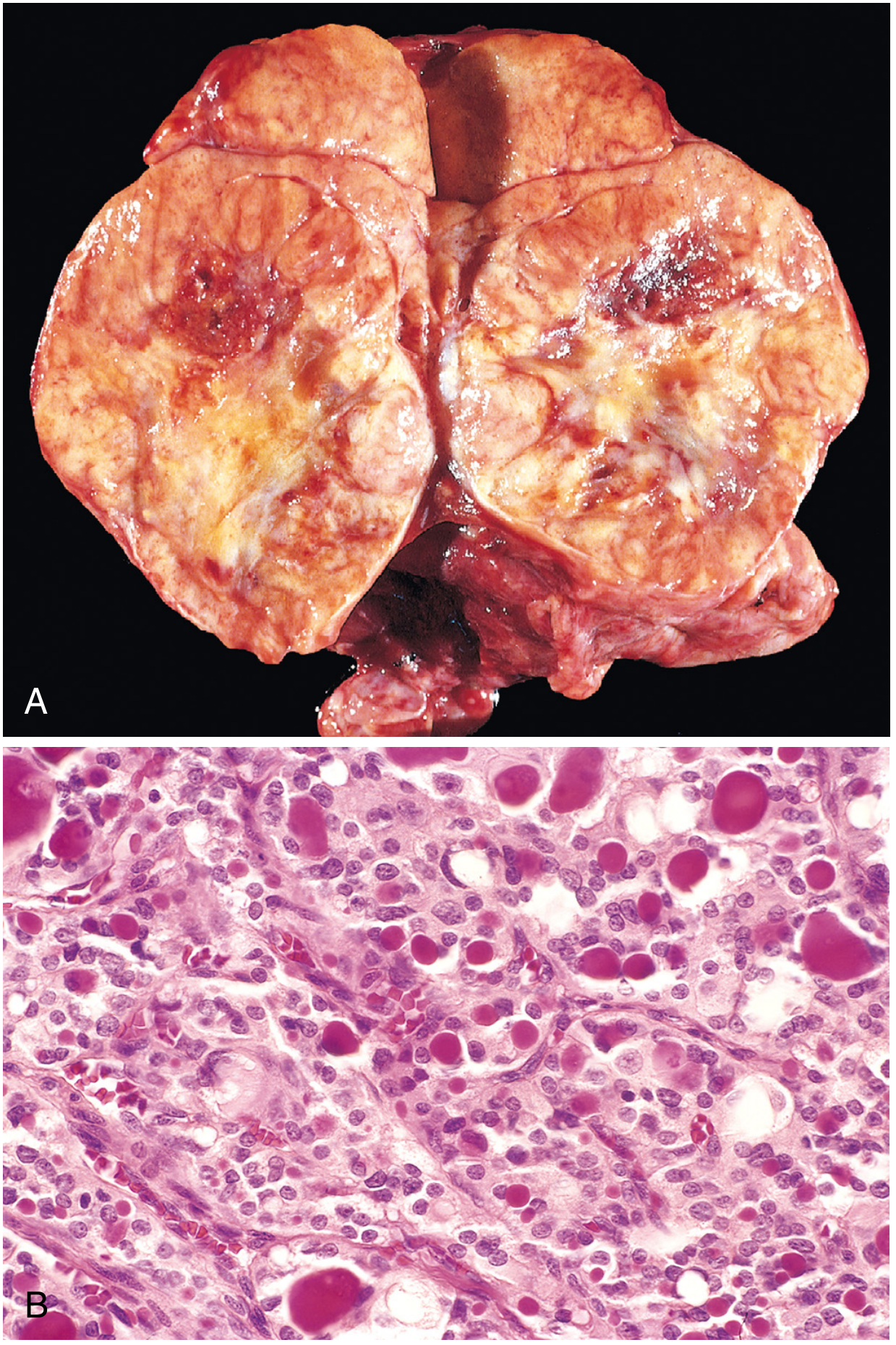
Fig. 24.20A Follicular Carcinoma - Gross appearance
- Large, light-tan/grey mass substantially replacing the thyroid lobe
- Small foci of hemorrhage visible
- Sharply demarcated but WITHOUT a well-formed capsule (unlike adenoma)
- Note: Gross appearance alone CANNOT reliably distinguish follicular adenoma from carcinoma
Histology - Capsular Invasion (Key Diagnostic Feature)
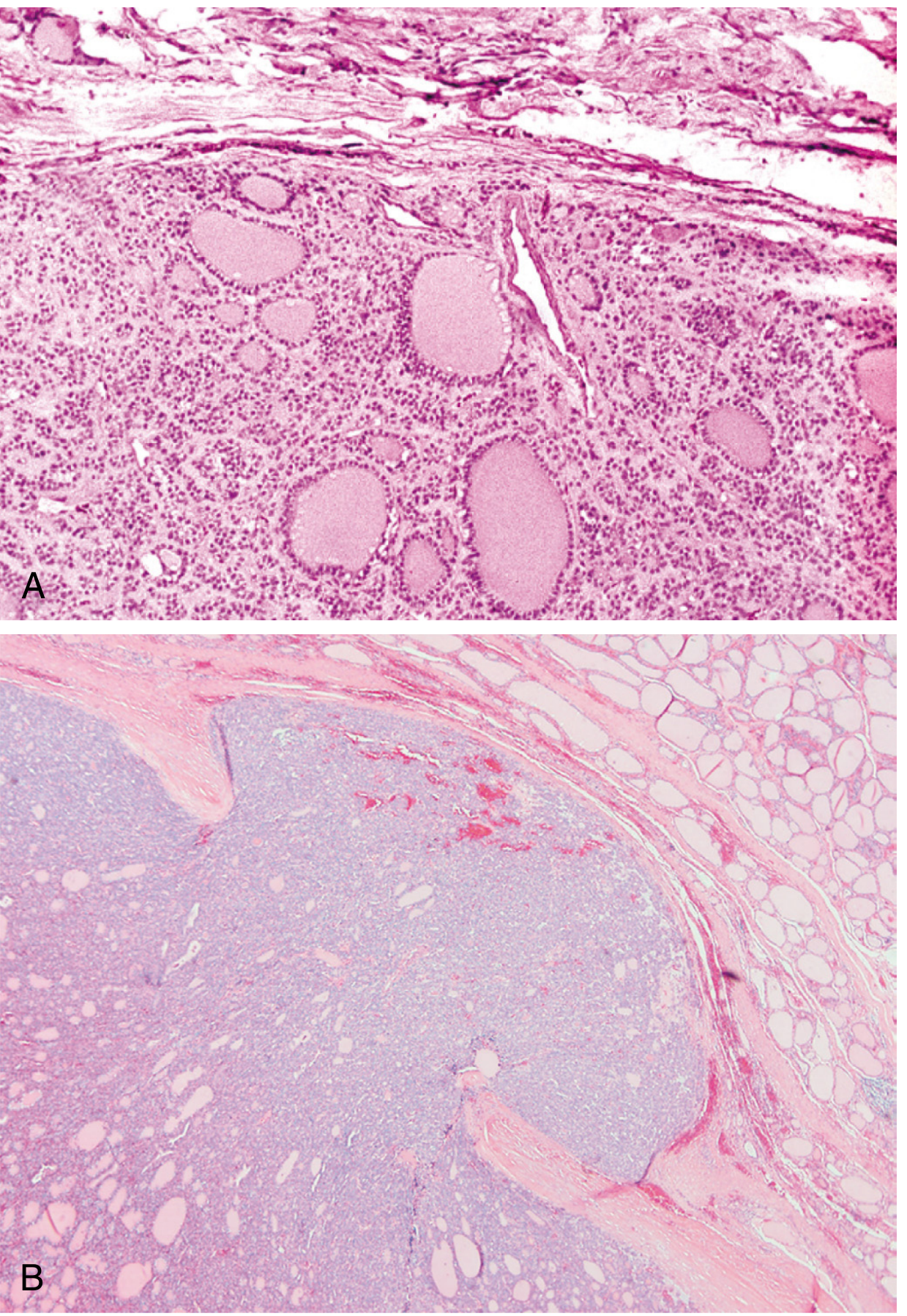
Fig. 24.21 Capsular Integrity - Adenoma vs. Carcinoma (Robbins)
(A) FOLLICULAR ADENOMA:
- Complete, intact fibrous capsule (circumferential)
- No capsular breach
- Compressed normal thyroid outside capsule
- Follicular cells uniform; colloid-filled follicles
(B) FOLLICULAR CARCINOMA:
- CAPSULAR INVASION - tumor mushrooming through capsule
- And/or VASCULAR INVASION (tumor in venous vessels)
- These two features = DIAGNOSTIC of malignancy
- FNAC CANNOT distinguish adenoma from carcinoma
(requires histology of capsule)
Rule for exams:
Capsular invasion + Vascular invasion = Follicular CARCINOMA Absence of both = Follicular ADENOMA (regardless of nuclear atypia)
MEDULLARY CARCINOMA - Gross & Histo
Gross
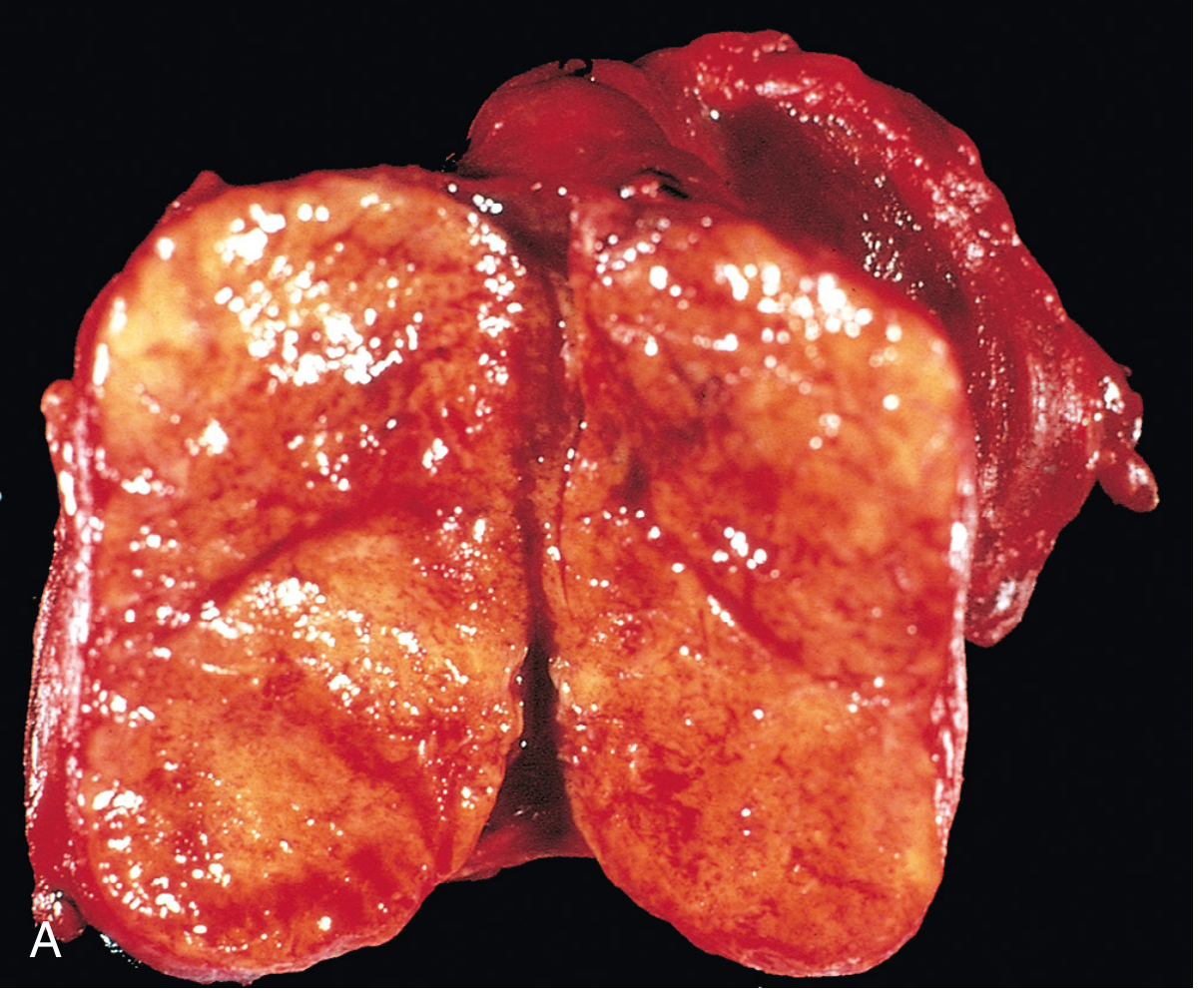
Fig. 24.22A Medullary Carcinoma - Gross (Robbins)
- Firm, pale grey-tan to cream-colored SOLITARY nodule (in sporadic)
- Bilateral and multicentric in MEN2 syndrome
- Infiltrative, no true capsule
- May contain areas of necrosis/hemorrhage in large lesions
Histology (Amyloid stroma)
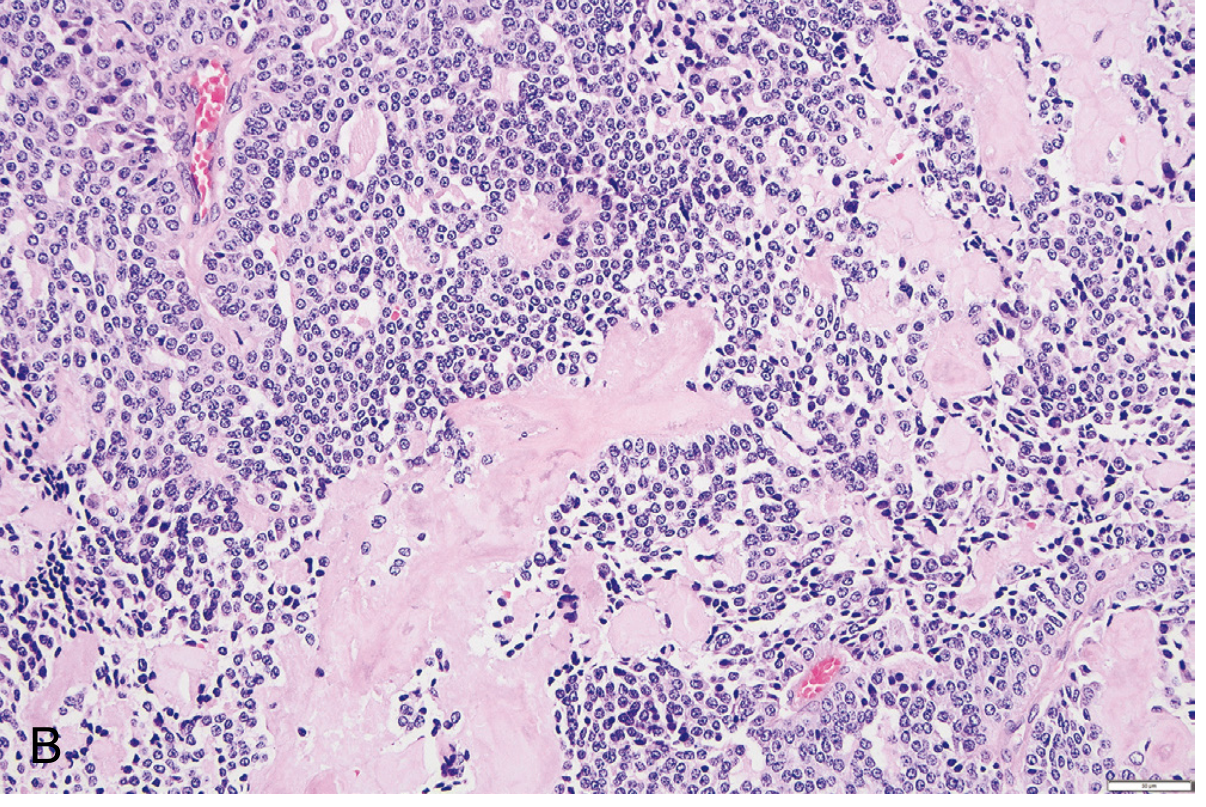
Fig. 24.22B Medullary Carcinoma - H&E section (Robbins)
Key histological features:
1. POLYGONAL to SPINDLE-SHAPED cells
2. Arranged in NESTS, TRABECULAE (neuroendocrine pattern)
3. Round nuclei with STIPPLED/SALT-AND-PEPPER CHROMATIN
(typical of all neuroendocrine tumors)
4. AMYLOID STROMA (pink, acellular, intercellular material)
- Derived from calcitonin polypeptides
- Congo red POSITIVE (apple-green birefringence under polarized light)
5. C-cell hyperplasia in surrounding parenchyma (in MEN2 cases)
EM of Medullary Carcinoma
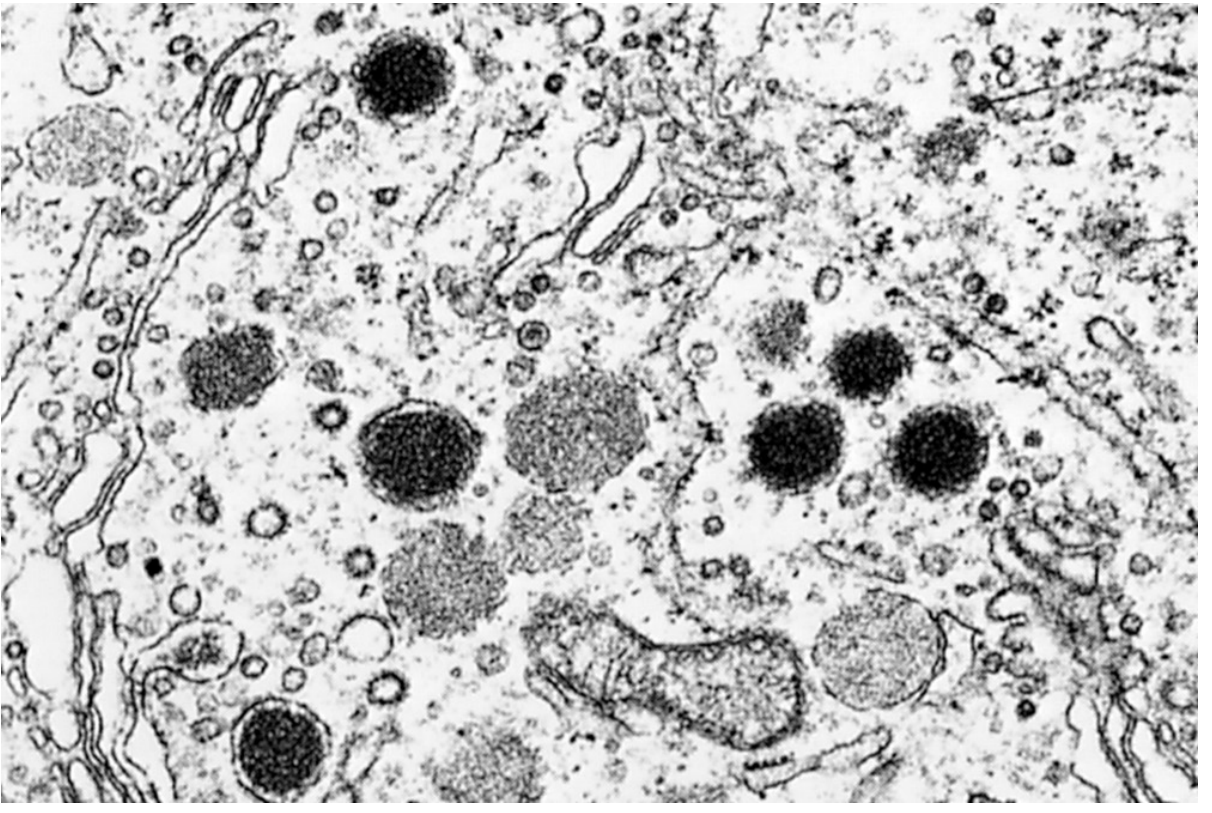
Fig. 24.23 Electron Micrograph - Medullary Carcinoma (Robbins)
- Dense, membrane-bound neurosecretory granules (dark oval bodies)
- Granules are the storage sites of calcitonin and other peptides
- Confirms neuroendocrine (parafollicular C cell) origin
DIABETIC NEPHROPATHY - Pathophysiology Diagram
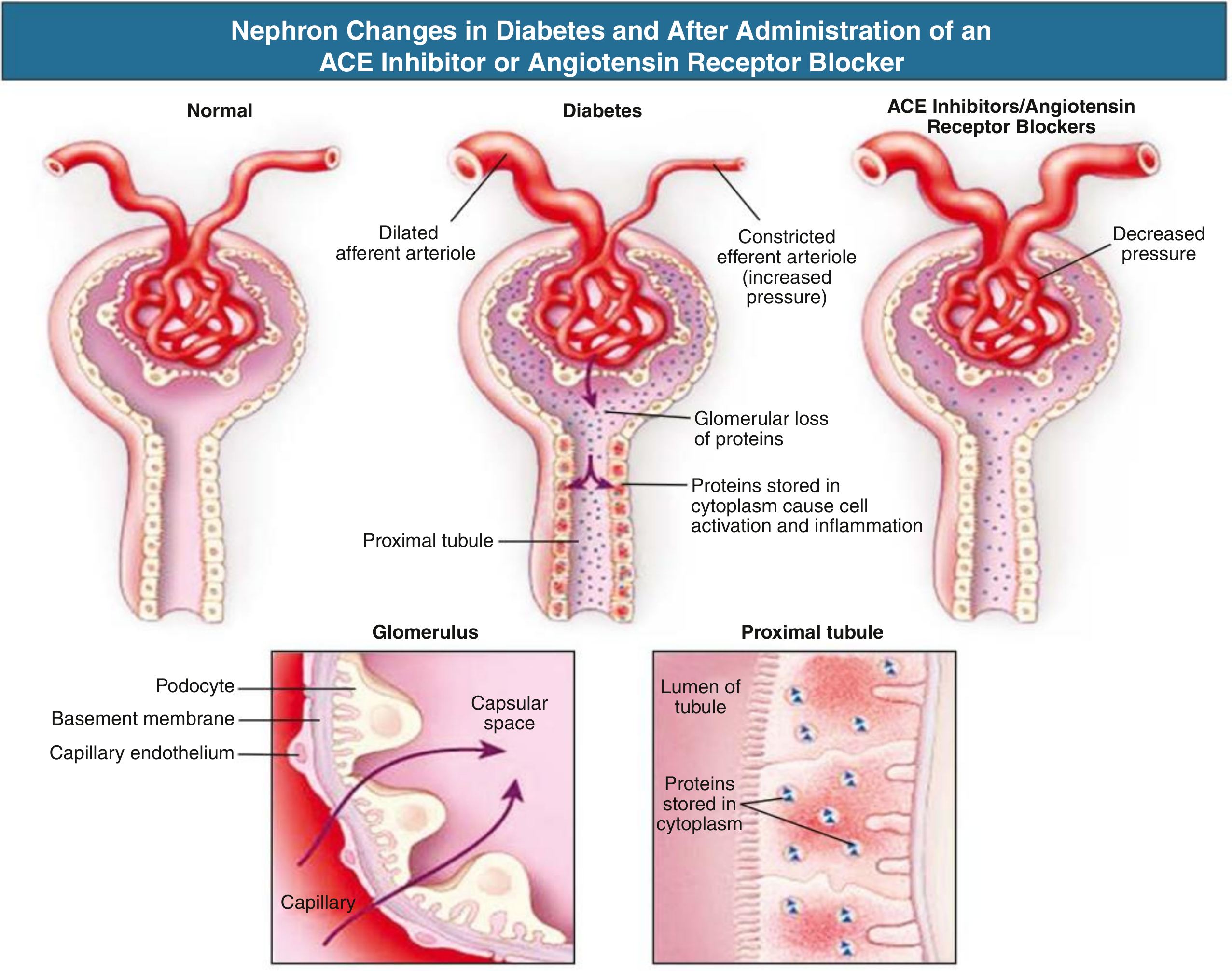
Fig. Nephron Changes in Diabetic Kidney Disease (Comprehensive Clinical Nephrology)
Reading the diagram:
NORMAL: Balanced afferent/efferent tone
↓
DIABETES: Dilated AFFERENT + Constricted EFFERENT (Ang II)
→ Glomerular HYPERTENSION (↑ intraglomerular pressure)
→ Protein leaks across GBM
→ Proteins endocytosed by proximal tubular cells
→ Inflammation → Interstitial fibrosis
↓
ACE-I / ARBs: Dilate efferent arteriole
→ ↓ Intraglomerular pressure → ↓ Proteinuria
→ Slow progression of nephropathy
SUMMARY TABLE - Gross & Histo Features for Exam
| Lesion | Gross | Key Histology |
|---|---|---|
| Colloid Goitre | Enlarged, tan/brown, gelatinous cut surface, multiple nodules | Distended follicles + flat epithelium + scalloped colloid |
| Hashimoto's | Pale yellow-tan, firm, diffusely enlarged | Lymphocytes + germinal centers + Hurthle cells + fibrosis |
| Papillary Ca | Firm, white, non-encapsulated, papillary projections visible | Orphan Annie nuclei + nuclear grooves + psammoma bodies |
| Follicular Ca | Solitary, grey-tan, may breach capsule | Uniform follicles + CAPSULAR/VASCULAR INVASION (key!) |
| Medullary Ca | Firm, pale-cream, solitary (or bilateral in MEN2) | Nests of spindle cells + amyloid stroma + Congo red + |
| Diabetic Nephropathy | Enlarged kidneys early; small, granular, scarred late | Kimmelstiel-Wilson nodules + GBM thickening + arteriolar hyalinosis |
All histopathology images: Robbins & Cotran Pathologic Basis of Disease (9780443264528). Nephron diagram: Comprehensive Clinical Nephrology, 7th Edition.
This is a shared conversation. Sign in to Orris to start your own chat.