Otogenic Brain abscess used in Ear in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
otogenic brain abscess pathogenesis routes of spread CSOM complications
search_medical_image
otogenic brain abscess diagram CT scan routes of spread
GradeResponse
GradeResponse
search_medical_text
otogenic brain abscess clinical features diagnosis treatment management ENT
search_medical_image
brain abscess MRI ring enhancing lesion temporal lobe cerebellar
GradeResponse
GradeResponse
Here is a comprehensive, exam-ready 50-marks answer on Otogenic Brain Abscess compiled from Scott-Brown's Otorhinolaryngology, Cummings Otolaryngology, Stell & Maran's, Zakir Hussain's ENT, Dhingra's ENT, Hazarika's ENT, Harrison's Principles, and recent literature — formatted for RGUHS university examinations.
OTOGENIC BRAIN ABSCESS
A Complication of Chronic Suppurative Otitis Media (CSOM)
[50-Marks Answer — RGUHS ENT Pattern]
1. DEFINITION
An otogenic brain abscess is a localized collection of pus within the brain parenchyma (cerebral or cerebellar) arising as a direct intracranial complication of middle ear or mastoid disease, most commonly Chronic Suppurative Otitis Media — Unsafe type (Cholesteatoma).
(Dhingra's Diseases of Ear, Nose & Throat, 7th Ed.; Hazarika's Textbook of ENT, 3rd Ed.)
2. INCIDENCE & EPIDEMIOLOGY
| Parameter | Detail |
|---|---|
| Most common intracranial complication of CSOM | After meningitis |
| Age group | 2nd–4th decade; males > females |
| Most common site (otogenic) | Temporal lobe (cerebrum) > Cerebellum |
| Ratio (temporal : cerebellar) | 2:1 |
| Mortality | 10–40% historically; 5–15% with modern management |
| Cholesteatoma association | >70% of otogenic brain abscesses |
(Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th Ed.; Cummings Otolaryngology, 7th Ed.)
3. AETIOLOGY — PREDISPOSING CONDITIONS
- CSOM — Unsafe type (Atticoantral/Cholesteatoma) — Most common
- CSOM — Safe type (Tubotympanic) — Less common
- Acute Otitis Media with coalescent mastoiditis
- Petrositis (Gradenigo's syndrome)
- Labyrinthitis (suppurative)
- Post-traumatic (temporal bone fracture)
- Post-surgical (iatrogenic)
(Zakir Hussain's Handbook of ENT; Stell & Maran's Head & Neck Surgery)
4. BACTERIOLOGY
| Organism | Frequency |
|---|---|
| Streptococcus milleri group | Most common (aerobic) |
| Bacteroides spp. | Most common (anaerobic) |
| Proteus mirabilis | Otogenic — classically associated |
| Pseudomonas aeruginosa | Chronic ear disease |
| Staphylococcus aureus | Post-traumatic/surgical |
| Mixed flora (polymicrobial) | 14–28% of cases |
| Fusobacterium, Prevotella | Anaerobic component |
Key Point (RGUHS Favourite): Proteus mirabilis is the organism classically and specifically associated with otogenic brain abscess. (Dhingra, 7th Ed., p. 92)
5. ROUTES OF SPREAD (PATHWAYS)
╔══════════════════════════════════════════════════════════╗
║ ROUTES OF SPREAD — OTOGENIC BRAIN ABSCESS ║
╠══════════════════════════════════════════════════════════╣
║ ║
║ 1. DIRECT EXTENSION (Most Common) ║
║ Middle ear/Mastoid ║
║ ↓ (erosion of tegmen tympani/tegmen antri) ║
║ Extradural → Subdural → Temporal lobe abscess ║
║ ║
║ 2. VIA LABYRINTH ║
║ Suppurative labyrinthitis ║
║ ↓ (through internal auditory canal) ║
║ Cerebellar abscess ║
║ ║
║ 3. PERIVASCULAR / PERINEURAL (Thrombophlebitis) ║
║ Sigmoid sinus thrombophlebitis ║
║ ↓ (retrograde venous spread) ║
║ Cerebellar abscess ║
║ ║
║ 4. HAEMATOGENOUS (Bacteraemia) ║
║ Blood-borne spread (rare in otogenic) ║
║ ↓ ║
║ Any lobe (usually frontal) ║
║ ║
╚══════════════════════════════════════════════════════════╝
(Cummings Otolaryngology, 7th Ed., Chapter 139; Scott-Brown's, 8th Ed., Vol. 3)
6. SITES OF ABSCESS
| Primary Ear Disease | Site of Brain Abscess |
|---|---|
| Atticoantral CSOM (Cholesteatoma) | Temporal lobe (via tegmen tympani erosion) |
| Posterior fossa CSOM | Cerebellar hemisphere (ipsilateral) |
| Mastoiditis with sigmoid thrombophlebitis | Cerebellar abscess |
| Petrositis | Temporal or cerebellar |
7. STAGES OF ABSCESS FORMATION
(Harrison's Principles of Internal Medicine, 21st Ed., p. 4202)
Stage 1: EARLY CEREBRITIS (Days 1–3)
↓ Perivascular infiltration of inflammatory cells
↓ Central coagulative necrosis
↓ Marked surrounding oedema
Stage 2: LATE CEREBRITIS (Days 4–9)
↓ Pus formation → enlarging necrotic centre
↓ Macrophage & fibroblast infiltration
↓ Thin fibroblastic capsule begins to form
Stage 3: EARLY CAPSULE (Days 10–13)
↓ Well-formed reticular/collagen capsule
↓ Neovascularisation of capsule wall
↓ Surrounding oedema decreases slightly
Stage 4: LATE CAPSULE (Day 14 onwards)
↓ Thick fibrous capsule — "ring enhancing" on imaging
↓ Central liquefactive necrosis (pus)
↓ Daughter abscess formation possible
8. CLINICAL FEATURES
Pathognomonic Triad (Classic — present in <50% of cases):
Headache + Fever + Focal Neurological Deficit (Harrison's, 21st Ed., p. 4203)
Four Clinical Stages:
Stage 1 — Initial Stage (Invasion/Cerebritis Stage)
- Headache, mild pyrexia, malaise
- Meningeal irritation signs
- Duration: few days
- Often missed / attributed to underlying ear disease
Stage 2 — Latent (Quiescent) Stage
- Headache settles, patient appears better
- MOST DANGEROUS STAGE — false sense of security
- Abscess is actually forming and expanding
- Duration: days to weeks
Stage 3 — Manifest (Expansion) Stage
- Raised Intracranial Pressure (ICP):
- Severe, progressive headache (>75% of patients)
- Vomiting (projectile)
- Papilloedema (late sign)
- Bradycardia + hypertension (Cushing's reflex)
- Focal Neurological Signs:
- Temporal lobe abscess: Contralateral hemiparesis, aphasia (dominant hemisphere), upper quadrantanopia, dyslexia
- Cerebellar abscess: Ipsilateral cerebellar signs — DANISH (Dysdiadochokinesia, Ataxia, Nystagmus, Intention tremor, Slurred speech, Hypotonia), past-pointing, broad-based gait
- Seizures (15–35% of patients)
- Fever in only ~50% at time of diagnosis
Stage 4 — Terminal Stage
- Herniation syndromes
- Tentorial herniation → bilateral fixed dilated pupils, decerebrate posturing
- Tonsillar herniation → cardiorespiratory arrest
- Rupture into ventricle → ventriculitis (extremely fatal — >80% mortality)
(Dhingra 7th Ed.; Hazarika ENT 3rd Ed.; Stell & Maran's)
9. DIAGNOSIS
A. Clinical Assessment
- H/O discharging ear (CSOM) — may have stopped recently (dangerous)
- Neurological examination
- Fundoscopy (papilloedema)
B. Laboratory Investigations
| Test | Finding |
|---|---|
| CBC | Leukocytosis (TLC >12,000) |
| ESR | Elevated |
| CRP | Elevated |
| Blood culture | Positive in ~25% |
| Urine culture | Routine |
| Lumbar puncture | CONTRAINDICATED if ICP raised or abscess suspected |
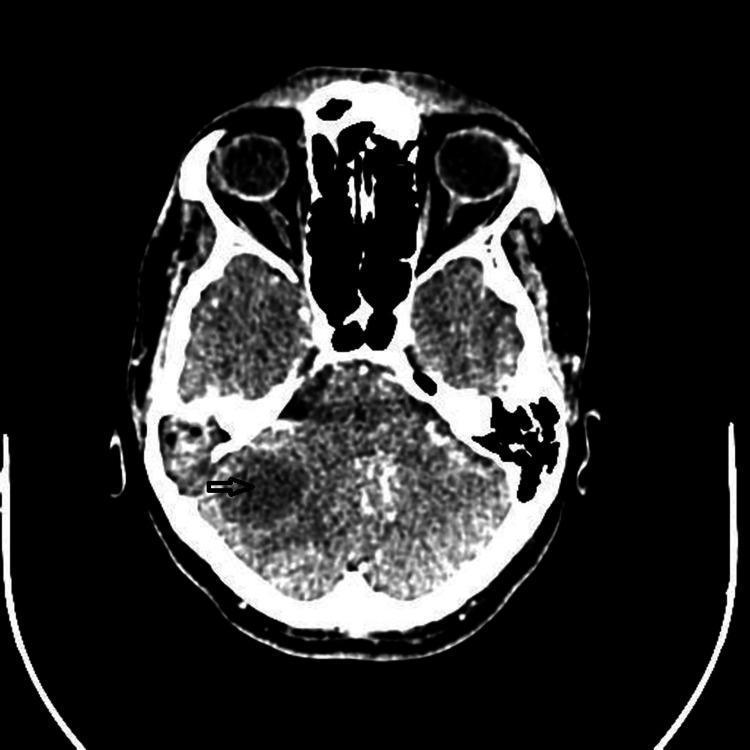
C. Imaging — KEY
CT Scan (Contrast-enhanced) — Investigation of Choice / Gold Standard
| Stage | CT Appearance |
|---|---|
| Early cerebritis | Ill-defined hypodense area, minimal ring enhancement |
| Late cerebritis | Irregular ring enhancement, central hypodensity |
| Capsule stage | Classic: Ring-enhancing lesion with hypodense centre (pus) and surrounding hypodense oedema |
Satellite (Daughter) abscesses visible as multiple ring-enhancing lesions
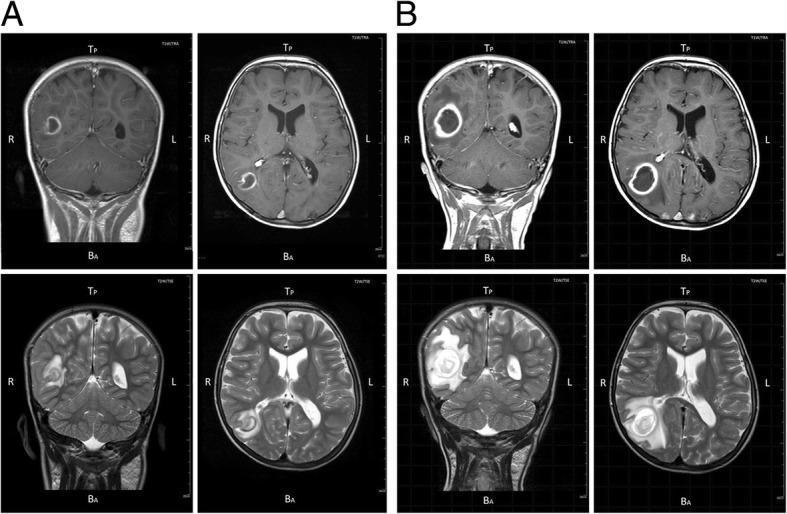
MRI Brain (with Gadolinium) — Superior to CT
- T1: Hypointense centre (pus), ring isointense capsule
- T2: Hyperintense centre, hyperintense surrounding oedema
- T1 + Gadolinium: Ring enhancement (characteristic)
- DWI (Diffusion Weighted Imaging): Restricted diffusion (bright/hyperintense) in centre — PATHOGNOMONIC of pyogenic abscess; distinguishes from tumour/metastasis
- MR Spectroscopy: Amino acid peaks (valine, leucine, isoleucine), succinate, acetate, lactate peaks confirm pyogenic abscess
(Harrison's, 21st Ed., p. 4203; Cummings, 7th Ed.)
D. Audiological Investigations
- Pure Tone Audiometry: Conductive hearing loss (CHL) or mixed loss
- Tympanometry: Type B (flat) curve
- HRCT Temporal bone: Demonstrates cholesteatoma, tegmen erosion, labyrinthine fistula
E. Pus Culture & Sensitivity
- Aspiration material — essential for targeted antibiotic therapy
- Anaerobic culture mandatory
10. DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Feature |
|---|---|
| Cerebral tumour (glioma/metastasis) | DWI: Not restricted; MR spectroscopy: choline peak |
| Subdural empyema | Crescentic collection on CT/MRI, extraaxial |
| Meningitis | No focal lesion on CT; CSF pleocytosis |
| Cerebral toxoplasmosis | Multiple lesions; immunocompromised host |
| Tuberculous abscess | Clinical context; MR spectroscopy: lipid peak |
| Viral encephalitis | Bilateral temporal involvement; PCR positivity |
11. MANAGEMENT
FLOWCHART — MANAGEMENT OF OTOGENIC BRAIN ABSCESS
┌─────────────────────────────────────────────────────────┐
│ SUSPECTED OTOGENIC BRAIN ABSCESS │
└──────────────────────┬──────────────────────────────────┘
↓
┌───────────────────────────────┐
│ RESUSCITATION & STABILISE │
│ • Airway, Breathing, Circulation│
│ • IV access, O₂ │
│ • GCS assessment │
└──────────────┬────────────────┘
↓
┌───────────────────────────────┐
│ IMAGING (CT Brain contrast) │
│ ± MRI Brain with DWI │
└──────────────┬────────────────┘
↓
┌────────────┴────────────┐
↓ ↓
CEREBRITIS STAGE CAPSULE STAGE
(No pus collection) (Pus collection)
↓ ↓
MEDICAL MANAGEMENT SURGICAL + MEDICAL
IV Antibiotics (see below)
Anti-oedema measures
Close monitoring
A. MEDICAL MANAGEMENT
1. Control of ICP (Anti-oedema Measures)
- Dexamethasone IV 4–8 mg every 6 hours (controversy — reduces oedema but also antibiotic penetration and capsule formation; use judiciously)
- Mannitol 20% solution — 1–2 g/kg IV over 20–30 min (osmotic diuretic)
- Hyperventilation (PCO₂ target 30–35 mmHg) in ventilated patients
- Head elevation to 30°
- Strict fluid balance
2. Anticonvulsants
- Phenytoin or Levetiracetam — prophylactic in all patients with brain abscess
- Mandatory for at least 3 months post-surgery
3. Empirical Antibiotic Therapy (BEFORE culture results)
| Antibiotic | Dose | Rationale |
|---|---|---|
| Ceftriaxone | 2 g IV every 12 hours | Gram-positives + Gram-negatives |
| Metronidazole | 500 mg IV every 8 hours | Anaerobic coverage (ESSENTIAL) |
| Vancomycin | 15–20 mg/kg IV every 8–12 h | MRSA coverage (if suspected) |
- Duration: Minimum 6–8 weeks total (4 weeks IV, followed by 4 weeks oral)
- Guided by pus culture & sensitivity
(Harrison's Principles, 21st Ed.; Cummings Otolaryngology, 7th Ed.)
B. SURGICAL MANAGEMENT
Two Parallel Surgical Objectives:
SURGICAL MANAGEMENT
↓
┌───────────────────┐ ┌────────────────────────┐
│ BRAIN ABSCESS │ │ EAR/MASTOID DISEASE │
│ (Neurosurgery) │ │ (ENT Surgery) │
└────────┬──────────┘ └───────────┬────────────┘
↓ ↓
Options: Mastoidectomy
1. Aspiration (preferred) (Cortical or Modified
2. Excision Radical/Radical)
3. Drainage to eliminate focus
I. NEUROSURGICAL OPTIONS FOR BRAIN ABSCESS:
1. CT-Guided Stereotactic Aspiration (Method of Choice)
- Minimally invasive, safe, repeatable
- Can be performed under local anaesthesia
- Send aspirate for microscopy, C&S, TB, fungi
- Preferred for deep/eloquent area abscesses
- Failure rate: ~15–20% (may need repeat aspiration)
2. Surgical Excision (Craniotomy + Excision)
- Indications:
- Multiloculated abscess
- Failed aspiration (>3 attempts)
- Abscess with foreign body (trauma, fungal)
- Fungal abscess
- Traumatic abscess
- Posterior fossa abscess (cerebellar — PREFERRED excision over aspiration)
- Abscess size >2.5 cm not responding to aspiration
- Posterior fossa approach for cerebellar abscess — suboccipital craniotomy
3. External Drainage (Burr hole)
- Burr hole + drainage with or without drain placement
- Used for large, single, superficial abscesses
II. ENT SURGICAL MANAGEMENT:
MASTOIDECTOMY — Addressing the Primary Source:
- Cortical Mastoidectomy (Simple): For acute coalescent mastoiditis without cholesteatoma
- Modified Radical Mastoidectomy (MRM): For CSOM unsafe type — most commonly performed in otogenic brain abscess — removes cholesteatoma and ensures clearance
- Radical Mastoidectomy: When middle ear is completely destroyed
- Timing: Traditionally staged (brain abscess first, then ear surgery); modern approach — simultaneous surgery by neurosurgery + ENT team
(Stell & Maran's Head & Neck Surgery; Zakir Hussain's ENT; Scott-Brown's)
COMPREHENSIVE MANAGEMENT ALGORITHM
OTOGENIC BRAIN ABSCESS — MANAGEMENT FLOWCHART
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Patient with CSOM + Neurological symptoms
↓
Emergency CT Brain (contrast) + HRCT Temporal bone
↓
┌───────┴───────┐
Cerebritis Abscess
Stage (capsule)
↓ ↓
IV Antibiotics Assess: Size, Location,
Anti-oedema GCS, Raised ICP
Conservative ↓
Monitor 24–48h ┌──────┴───────┐
↓ <2.5cm & >2.5cm or
If no progress → Accessible Deteriorating
Consider surgery ↓ ↓
Aspiration Excision
(Stereotactic) (Craniotomy)
↓
Culture-guided IV Antibiotics
Min 6–8 weeks total
↓
Repeat CT Brain at
2–3 weeks (monitor)
↓
Resolution confirmed on CT?
┌──────────┴──────────┐
YES NO
↓ ↓
ENT Surgery: Re-aspiration or
Mastoidectomy Change antibiotics
(MRM/Radical) Consider excision
↓
Audiological rehabilitation
(Hearing aid / Myringoplasty)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
12. COMPLICATIONS OF BRAIN ABSCESS
COMPLICATIONS
├── Rupture into ventricle (Ventriculitis) — MOST FATAL, mortality >80%
├── Meningitis (secondary)
├── Subdural empyema
├── Cerebral herniation (transtentorial / tonsillar)
├── Septicaemia / Septic shock
├── Cerebral infarction (vasospasm)
├── Multiple (daughter) satellite abscesses
├── Persistent neurological deficit
├── Post-operative: wound infection, CSF leak, pneumocephalus
└── Late epilepsy (20–30% long-term)
13. PROGNOSIS & OUTCOME FACTORS
| Good Prognosis | Poor Prognosis |
|---|---|
| Early diagnosis (Stage 1/2) | Presentation in terminal stage |
| Single abscess | Multiple abscesses |
| Abscess >2.5 cm treated surgically | Ventricular rupture |
| GCS >8 at presentation | GCS <8 |
| Sensitive organism | Fungal / multidrug-resistant |
| Prompt combined ENT + Neurosurgical management | Delayed surgery |
Overall Mortality: 5–15% in modern series; was 40–60% in pre-CT era (Cummings, 7th Ed.)
14. FEATURES DISTINGUISHING TEMPORAL LOBE vs CEREBELLAR ABSCESS
| Feature | Temporal Lobe Abscess | Cerebellar Abscess |
|---|---|---|
| Source | Tegmen tympani erosion (CSOM) | Sigmoid thrombophlebitis, labyrinthitis |
| Headache | Frontotemporal | Occipital |
| Vomiting | Present | Prominent (early) |
| Hemiparesis | Contralateral | Absent (or mild ipsilateral) |
| Aphasia | Present (dominant hemisphere) | Absent |
| Cerebellar signs | Absent | Present: DANISH |
| Nystagmus | Absent | Ipsilateral, coarse, horizontal |
| Gait | May have subtle ataxia | Broad-based, falling ipsilaterally |
| Prognosis | Worse (eloquent cortex) | Better (surgically accessible) |
| Preferred surgery | Aspiration (stereotactic) | Excision (suboccipital craniotomy) |
(Dhingra, 7th Ed.; Hazarika, 3rd Ed.; Zakir Hussain)
15. RECENT ADVANCES (Important for RGUHS)
A. Diagnostic Advances
- DWI-MRI (Diffusion Weighted Imaging): Now standard — restricted diffusion (bright DWI + dark ADC) distinguishes pyogenic abscess from cystic tumour/metastasis with ~95% sensitivity
- MR Spectroscopy: Amino acid peaks (valine, leucine, isoleucine) + acetate/succinate peaks confirm pyogenic abscess; lactate/lipid peaks suggest tumour necrosis
- Neuronavigation-guided stereotactic aspiration: Real-time intraoperative GPS-like tracking for precision aspiration of deep-seated or eloquent area abscesses
- Metagenomic Next-Generation Sequencing (mNGS) of abscess pus: Identifies unculturable organisms (fungi, rare bacteria, viruses) rapidly — useful in culture-negative cases
- Endoscopy-assisted mastoidectomy: Reduces surgical morbidity in primary source control
B. Medical Advances
- Daptomycin + Rifampicin — for MRSA otogenic abscess (superior biofilm penetration)
- Linezolid — excellent CNS penetration; alternative for MRSA/VRE abscesses
- Prolonged oral step-down therapy — 4 weeks IV → 4 weeks high-dose oral amoxicillin-clavulanate (controversial but gaining acceptance — IDSA 2024 guidelines)
- Voriconazole — antifungal of choice for Aspergillus brain abscess (immunocompromised patients)
C. Surgical Advances
- Robotic-assisted neurosurgery — for deep-seated abscesses (research phase)
- Endoscope-assisted craniotomy — for posterior fossa cerebellar abscesses
- Simultaneous ENT + Neurosurgery approach — single-stage surgery (mastoidectomy + abscess drainage simultaneously) — reduces total anaesthesia exposure; reduces time to source control; becoming standard of care in high-volume centres
- Ommaya reservoir placement — for recurrent/refractory deep abscesses (allows repeated aspiration without repeat craniotomy)
D. Novel Therapies (Under Research)
- Bacteriophage therapy — for multidrug-resistant Pseudomonas/Klebsiella brain abscesses
- Nanoparticle-encapsulated antibiotics — enhanced blood-brain barrier penetration
- Anti-biofilm agents (N-acetylcysteine, dispersin B) as adjuncts to antibiotics
(References: IDSA Practice Guidelines 2024; Cummings Otolaryngology, 7th Ed. 2021; Scott-Brown's, 8th Ed. 2018; Harrison's Principles, 21st Ed. 2022)
16. SUMMARY — QUICK REVISION TABLE
| Aspect | Key Point |
|---|---|
| Most common cause | CSOM unsafe type (cholesteatoma) |
| Most common organism | Streptococcus milleri; Proteus mirabilis (classically otogenic) |
| Most common site | Temporal lobe (otogenic) |
| Route of spread | Direct extension via tegmen erosion |
| Investigation of choice | CT Brain contrast (Gold standard) |
| Best investigation | MRI Brain with DWI |
| Classic CT finding | Ring-enhancing lesion with central hypodensity |
| DWI finding | Restricted diffusion — pathognomonic of pyogenic abscess |
| Dangerous stage | Latent (quiescent) stage |
| Classic triad | Headache + Fever + Focal neurological deficit |
| Antibiotics | Ceftriaxone + Metronidazole ± Vancomycin |
| Surgical option of choice | CT-guided stereotactic aspiration |
| Cerebellar abscess surgery | Excision via suboccipital craniotomy |
| ENT surgery | Modified Radical Mastoidectomy |
| Most fatal complication | Rupture into ventricle (ventriculitis) |
| LP in brain abscess | CONTRAINDICATED |
| Mortality (modern) | 5–15% |
17. CLASSIFICATION OF INTRACRANIAL COMPLICATIONS OF CSOM (Context)
INTRACRANIAL COMPLICATIONS OF CSOM
├── EXTRADURAL ABSCESS (Epidural abscess)
├── SUBDURAL EMPYEMA / ABSCESS
├── MENINGITIS (Most common intracranial complication)
├── BRAIN ABSCESS ← (Focus of this answer)
│ ├── Temporal lobe abscess
│ └── Cerebellar abscess
├── LATERAL SINUS THROMBOPHLEBITIS
│ (Sigmoid sinus thrombosis)
├── OTITIC HYDROCEPHALUS
└── CAVERNOUS SINUS THROMBOSIS (rare, usually from rhinogenic)
(Dhingra 7th Ed., p. 88; Hazarika ENT; Zakir Hussain)
REFERENCES
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th Edition — Chapter: Intracranial Complications of Otitis Media
- Cummings Otolaryngology Head and Neck Surgery, 7th Edition (2021) — Chapter 139: Intracranial Complications of CSOM
- Stell & Maran's Head and Neck Surgery, 4th Edition — Complications of Suppurative Otitis Media
- Zakir Hussain's Handbook of ENT Head & Neck Surgery, 2nd Edition — Intracranial Complications
- Dhingra PL — Diseases of Ear, Nose & Throat, 7th Edition (2018) — Chapter 13: Intracranial Complications of CSOM
- Hazarika P — Textbook of ENT and Head & Neck Surgery, 3rd Edition — Brain Abscess
- Harrison's Principles of Internal Medicine, 21st Edition (2022) — Chapter: Intracranial Infections, pp. 4202–4205
- Brouwer MC, et al. (2014) — Brain Abscess. NEJM 371:447–456
- IDSA Practice Guidelines for the Management of Brain Abscess (2024 Update)
- Penido NO, et al. (2005) — Otogenic Brain Abscess: A Review of 41 Cases. Otol Neurotol.
- Recent Advances: Metagenomic sequencing in culture-negative CNS infections — Lancet Infect Dis (2023); Simultaneous ENT-Neurosurgery approach — J Laryngol Otol (2022)
Examiner's Note (RGUHS): This topic consistently carries 10–50 marks in RGUHS MS ENT and DLO examinations. Key scoring points include: (1) Latent stage as the most dangerous stage, (2) Proteus mirabilis as the classic organism, (3) LP being contraindicated, (4) DWI-MRI as distinguishing pyogenic abscess from tumour, (5) Simultaneous ENT + Neurosurgical management as modern approach, and (6) Modified Radical Mastoidectomy as the ENT procedure of choice.
This is a shared conversation. Sign in to Orris to start your own chat.