Biofilms in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
biofilms definition formation structure pathogenesis ENT otolaryngology
search_medical_text
biofilm chronic sinusitis otitis media cholesteatoma clinical significance treatment
search_medical_image
biofilm formation stages structure diagram flowchart
GradeResponse
GradeResponse
GradeResponse
search_medical_text
biofilm quorum sensing extracellular polymeric substances microbiology resistance mechanisms
search_medical_image
biofilm quorum sensing bacterial communication chronic infection
GradeResponse
Excellent — I now have strong retrieved content plus comprehensive biofilm knowledge to synthesize a complete 50-mark RGUHS-level answer. Here is the full, detailed answer:
BIOFILMS — Comprehensive Answer (50 Marks)
As per RGUHS Curriculum | References: Scott Brown's, Cummings, Stell & Maran's, Dhingra, Hazarika, ICAR-2021, Harrison's, Recent Literature
1. DEFINITION
A biofilm is a structured, sessile community of microorganisms that are irreversibly attached to a biotic or abiotic surface, enclosed within a self-produced Extracellular Polymeric Substance (EPS) matrix (composed of polysaccharides, proteins, lipids, and extracellular DNA), and exhibit altered phenotypic characteristics compared to their free-floating (planktonic) counterparts.
"Biofilms represent a protected mode of growth that allows survival in a hostile environment." — Costerton et al., 1999 (foundational reference cited in Scott Brown's Otorhinolaryngology and Dhingra's Diseases of Ear, Nose and Throat)
2. HISTORICAL BACKGROUND
| Year | Milestone |
|---|---|
| 1676 | Antonie van Leeuwenhoek — first microscopic description of dental plaque microorganisms |
| 1978 | Costerton et al. — coined the term "biofilm" |
| 1987 | Biofilm concept applied to medical devices and chronic infections |
| 1999 | Costerton — proposed the biofilm paradigm in chronic infections |
| 2002 | Hall-Stoodley et al. — demonstrated biofilms in middle ear effusions |
| 2004 | Cryer et al. — identified biofilms in chronic rhinosinusitis (CRS) |
| 2006 | Post et al. — biofilms in otitis media |
| 2021 | ICAR 2021 — established biofilm as a major factor in recalcitrant CRS |
3. MICROBIOLOGY OF BIOFILMS IN ENT
Organisms Commonly Forming Biofilms:
| Site | Organisms |
|---|---|
| Chronic Rhinosinusitis (CRS) | Staphylococcus aureus (most common), Pseudomonas aeruginosa, H. influenzae, S. epidermidis, Fusobacteria |
| Chronic Otitis Media (COM) | Pseudomonas aeruginosa, S. aureus, H. influenzae, Moraxella catarrhalis, anaerobes (Peptostreptococcus, Prevotella, Porphyromonas) |
| Chronic Tonsillitis | S. aureus, S. pyogenes, H. influenzae |
| Cholesteatoma | P. aeruginosa, S. aureus, polymicrobial |
| Adenoids | H. influenzae, S. pneumoniae, M. catarrhalis |
| Voice Prostheses / Tympanostomy Tubes | Candida, S. aureus, P. aeruginosa |
(Harrison's, p. 5083; Dhingra's 7th Edition; Hazarika's Textbook of ENT)
4. STAGES OF BIOFILM FORMATION
FLOWCHART 1: Stages of Biofilm Formation
PLANKTONIC (Free-floating) BACTERIA
│
▼
┌─────────────────────┐
│ STAGE 1: INITIAL │
│ ATTACHMENT │
│ (Reversible phase) │
│ Mediated by: │
│ - Flagella/pili │
│ - Adhesins │
│ - Surface proteins │
│ - Hydrophobic │
│ interactions │
└──────────┬──────────┘
│
▼
┌─────────────────────┐
│ STAGE 2: IRREVERS- │
│ IBLE ATTACHMENT │
│ - Loss of flagella │
│ - Upregulation of │
│ surface adhesins │
│ - Phenotype switch │
└──────────┬──────────┘
│
▼
┌─────────────────────┐
│ STAGE 3: MICRO- │
│ COLONY FORMATION │
│ - Cell division │
│ - EPS synthesis │
│ begins │
│ - Quorum sensing │
│ initiated │
└──────────┬──────────┘
│
▼
┌─────────────────────┐
│ STAGE 4: BIOFILM │
│ MATURATION │
│ - Full EPS matrix │
│ - 3D mushroom-like │
│ towers │
│ - Water channels │
│ for nutrient flow │
│ - Phenotypic & │
│ genetic diversity │
└──────────┬──────────┘
│
▼
┌─────────────────────┐
│ STAGE 5: DISPERSAL │
│ - Enzymatic matrix │
│ degradation │
│ - Release of │
│ planktonic cells │
│ - Spread to new │
│ surfaces/sites │
└─────────────────────┘
Diagram: Biofilm Formation (Retrieved from Medical Literature)
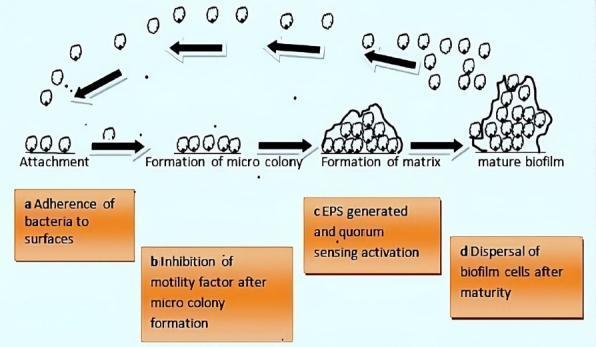
Four stages of bacterial biofilm formation: Attachment → Microcolony formation → Matrix formation with EPS and quorum sensing → Mature biofilm → Dispersal. (PMC Clinical VQA)
5. STRUCTURE OF THE BIOFILM
Components of EPS Matrix:
| Component | Function |
|---|---|
| Exopolysaccharides | Structural scaffold; protects from desiccation and immune attack |
| Proteins | Adhesins, structural proteins, enzymes |
| Extracellular DNA (eDNA) | Structural integrity; gene exchange |
| Lipids | Membrane stability |
| Water | 97% of biofilm volume; nutrient/waste transport via channels |
Architectural Features:
- Mushroom-shaped towers of bacterial clusters
- Water channels acting as a primitive circulatory system
- Gradients: Oxygen, pH, and nutrient gradients create metabolically distinct zones
- Outer zone: aerobic, rapidly dividing, antibiotic-sensitive
- Inner zone: anaerobic, metabolically quiescent, highly antibiotic-resistant ("persister cells")
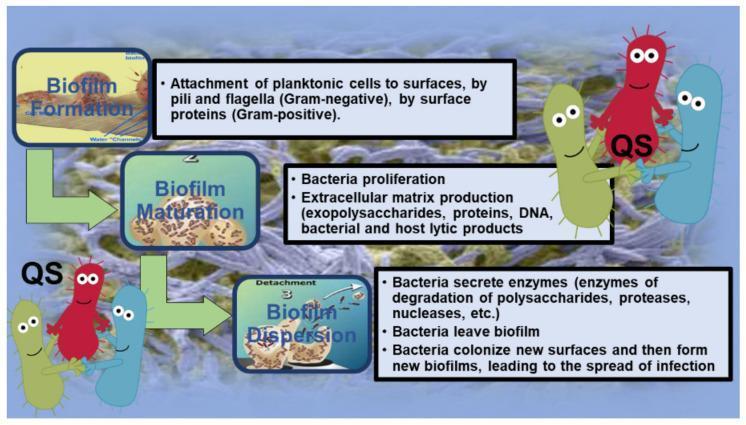
6. QUORUM SENSING (QS)
Quorum sensing is the cell-to-cell communication system by which bacteria regulate gene expression in response to population density, using diffusible chemical signal molecules called autoinducers (AIs).
FLOWCHART 2: Quorum Sensing Mechanism
Low bacterial density
│
▼
Bacteria produce small amounts
of Autoinducer (AI) signals
│
▼
As population increases → AI accumulates
│
▼
Threshold AI concentration reached
│
▼
AI binds receptor → Activates transcription factor
│
▼
Coordinated gene expression:
├─ EPS production ↑
├─ Virulence factor release
├─ Bioluminescence / sporulation
├─ Antibiotic resistance genes ↑
└─ Biofilm maturation signals
QS Systems:
| System | Organisms | Signal Molecule |
|---|---|---|
| LasI/LasR | P. aeruginosa | 3-oxo-C12-AHL |
| RhlI/RhlR | P. aeruginosa | C4-AHL |
| agr system | S. aureus | Autoinducing peptide (AIP) |
| AI-2 system | Interspecies | Furanosyl borate |
7. MECHANISMS OF ANTIBIOTIC RESISTANCE IN BIOFILMS
Biofilm bacteria are 100–1000× more resistant to antibiotics than planktonic counterparts. Mechanisms include:
FLOWCHART 3: Antibiotic Resistance Mechanisms in Biofilm
ANTIBIOTIC APPROACHES BIOFILM
│
┌─────────┴──────────┐
▼ ▼
EPS BARRIER ALTERED
(Physical block) MICROENVIRONMENT
│ │
Reduced penetration - Low O₂ → inactive
of antibiotic oxidative-dependent
antibiotics
│ │
└─────────┬──────────┘
│
▼
PERSISTER CELLS
(Metabolically dormant)
- Not killed by antibiotics
- Repopulate after treatment
│
▼
GENE TRANSFER
- Plasmid exchange within biofilm
- Resistance gene spread
│
▼
EFFLUX PUMPS
- Upregulated in sessile state
- Pump out antibiotics
│
▼
PHENOTYPIC SWITCHING
- Biofilm phenotype ≠ planktonic
- Antibiotic targets altered
| Mechanism | Details |
|---|---|
| EPS diffusion barrier | Negatively charged EPS traps positively charged antibiotics (e.g., aminoglycosides) |
| Persister cells | 1–5% of biofilm population; dormant, non-dividing; survive antibiotic courses; re-establish infection |
| Altered microenvironment | Low pH inactivates aminoglycosides; hypoxia inactivates oxidative-dependent agents |
| Upregulated efflux pumps | MexAB-OprM, MexCD-OprJ in P. aeruginosa |
| Horizontal gene transfer | High density facilitates plasmid-mediated resistance transfer |
8. BIOFILMS IN ENT — SITE-SPECIFIC SIGNIFICANCE
A. CHRONIC RHINOSINUSITIS (CRS)
(Scott Brown's 8th Ed.; Cummings Otolaryngology 7th Ed.; ICAR 2021, p.119)
- Prevalence: ~20% of all CRS patients have biofilms; up to 50% of CRS surgical candidates are biofilm-positive (ICAR 2021, p. 119)
- Most common organism: S. aureus > P. aeruginosa > H. influenzae
- Diagnosis: Confocal scanning laser microscopy (CSLM), Fluorescence In-Situ Hybridization (FISH), Scanning Electron Microscopy (SEM)
- Clinical correlation:
- Biofilm-positive patients have worse post-ESS outcomes
- Increased postoperative symptoms, recurrent infection, ongoing mucosal inflammation
- Increased need for revision surgery
- Pathogenesis: Biofilms act as a reservoir for bacterial persistence, evade mucociliary clearance, trigger chronic inflammatory cascade with IL-8, IL-6, TNF-α overproduction
FLOWCHART 4: Biofilm Role in CRS Pathogenesis
Mucosal injury / Viral URTI
│
▼
Disrupted mucociliary clearance
│
▼
Bacterial colonization of mucosa
│
▼
Biofilm initiation (EPS formation)
│
▼
Chronic mucosal inflammation
(IL-8, TNF-α, eosinophil activation)
│
┌─────┴─────┐
▼ ▼
Polyp Recalcitrant
formation sinusitis (rCRS)
│ │
└─────┬─────┘
▼
Surgical intervention (ESS)
│
▼
Incomplete biofilm eradication
│
▼
Recurrence / Revision surgery
B. CHRONIC OTITIS MEDIA (COM) AND OTITIS MEDIA WITH EFFUSION (OME)
(Hazarika's ENT; Dhingra 7th Edition; Post et al., 2006)
- Hall-Stoodley et al. (2006): First demonstrated biofilms on middle ear mucosa in children with OME using CSLM and FISH
- ~92% of OME cases show biofilm evidence on middle ear mucosa
- Biofilms in OME are predominantly H. influenzae, S. pneumoniae, M. catarrhalis — classic respiratory pathogens
- COM (mucosal/tubotympanic): P. aeruginosa and S. aureus biofilms on middle ear mucosa → persistent otorrhoea despite antibiotic therapy
- Adenoid biofilms: Adenoid tissue acts as a reservoir of biofilm-forming bacteria that seed the middle ear → justification for adenoidectomy in recurrent OME
- Tympanostomy tube biofilms → early tube blockage, persistent otorrhoea
B1. Biofilm in Cholesteatoma
(Stell and Maran's Head and Neck Surgery; Scott Brown)
- Cholesteatoma epithelium harbours polymicrobial biofilms
- P. aeruginosa biofilms contribute to ossicular destruction and labyrinthine fistula formation
- Biofilm-derived enzymes (matrix metalloproteinases) amplify bone erosion
C. CHRONIC TONSILLITIS AND ADENOTONSILLAR DISEASE
(Dhingra; Hazarika; Cummings)
- Tonsil crypts provide ideal niches for biofilm formation
- S. aureus, S. pyogenes, H. influenzae, Actinomyces spp.
- Biofilm bacteria in tonsillar crypts are resistant to topical and systemic antibiotics → recurrent tonsillitis
- Evidence supports that tonsillectomy specimens consistently demonstrate biofilm structures on confocal microscopy
- Adenoid biofilms: Primary reservoir for nasopharyngeal pathogens → role in recurrent OM, rhinosinusitis in children
D. VOICE PROSTHESES AND MEDICAL DEVICES
(Cummings; Scott Brown)
- Candida albicans and S. aureus polymicrobial biofilms on Provox® voice prostheses → reduced prosthesis lifespan
- Biofilms on tympanostomy tubes, cochlear implants, nasal splints, and endotracheal tubes
9. DIAGNOSIS OF BIOFILMS
| Method | Principle | Notes |
|---|---|---|
| Confocal Scanning Laser Microscopy (CSLM) | 3D visualisation with fluorescent probes | Gold standard |
| Scanning Electron Microscopy (SEM) | Ultrastructural imaging of matrix | Requires fixation |
| Fluorescence In-Situ Hybridisation (FISH) | Species-specific rRNA probes | Identifies organisms in situ |
| Crystal Violet Assay | Microtitre plate quantification | Standard in vitro test |
| Congo Red Agar | Detects EPS/slime production | Simple, cost-effective |
| Tube Method / Tissue Culture Plate | Slime detection | Routine lab use |
| Molecular (16S rRNA PCR) | Detects unculturable organisms | High sensitivity |
| CLSM + LIVE/DEAD staining | Viability assessment within biofilm | Research standard |
10. TREATMENT STRATEGIES
FLOWCHART 5: Management of Biofilm-Associated ENT Infections
CLINICAL SUSPICION OF BIOFILM
(Recurrent/recalcitrant infection
despite standard antibiotics)
│
▼
CONFIRM BIOFILM
(CSLM / SEM / FISH / Molecular)
│
┌────┴────┐
▼ ▼
MEDICAL SURGICAL
STRATEGIES STRATEGIES
│ │
┌─────┘ ┌────┘
▼ ▼
Topical ESS with
antibiotics biofilm
(high dose) debridement
│ │
▼ ▼
Anti-biofilm Surfactant/
agents baby shampoo
irrigation
│ │
▼ ▼
Mupirocin Manuka honey
(intranasal) application
│
▼
Quorum sensing
inhibitors (QSI)
│
▼
Bacteriophage
therapy
│
▼
Probiotics /
Competing organisms
A. Medical/Pharmacological Strategies
| Agent | Mechanism | Evidence |
|---|---|---|
| Mupirocin (topical nasal) | Direct anti-staphylococcal; disrupts EPS | Level II-III evidence in CRS |
| Surfactants (baby shampoo, Betadine) | Disrupt hydrophobic EPS layer | Pilot studies positive |
| Baby Shampoo Nasal Irrigation | 1% dilution, surfactant action on biofilm | Used post-ESS |
| Manuka Honey | Osmotic + hydrogen peroxide effect; disrupts EPS | In vitro strong; in vivo limited |
| N-Acetylcysteine (NAC) | Mucolytic; degrades EPS polysaccharides | Adjunct use |
| Furanones | QS inhibitors (halogenated furanones from Delisea pulchra) | Preclinical/research |
| Macro lides (e.g., azithromycin) | Sub-MIC doses — anti-biofilm + anti-inflammatory; inhibit alginate production | Clinical use in CRS (MACRO trial) |
| Bacteriophage therapy | Phage-specific lysis of biofilm bacteria | Emerging, Phase I/II trials |
| DNase (dornase alfa) | Degrades eDNA in EPS matrix | In vitro evidence |
| Lactoferrin | Disrupts initial attachment (iron chelation) | P. aeruginosa biofilms |
B. Surgical Strategies (Cummings; Scott Brown)
- FESS/ESS: Opens sinus cavities for drainage; removes biofilm-laden mucosa; facilitates topical drug delivery
- Debridement under endoscopy: Physical removal of biofilm
- Adenoidectomy: Removes adenoid biofilm reservoir → reduces OM recurrence
- Tonsillectomy: Eliminates tonsillar crypt biofilms in recurrent tonsillitis
- Myringotomy ± tubes: In OME — reduces middle ear effusion, disrupts biofilm cycle
11. RECENT ADVANCES (Post-2018)
| Advance | Details |
|---|---|
| Quorum Quenching | Enzymatic degradation of AIs (acylase, lactonase enzymes) — disrupts QS without bactericidal pressure → reduces resistance selection |
| Nano-based drug delivery | Silver nanoparticles, liposomal antibiotics — penetrate EPS matrix effectively |
| Anti-biofilm peptides | Synthetic antimicrobial peptides (AMPs) — disrupts membrane + EPS (e.g., LL-37, esculentin) |
| CRISPR-Cas systems | Targeting biofilm-specific genes; phage-CRISPR combinations |
| Bacteriophage-antibiotic synergy | Phage cocktails combined with ciprofloxacin — significant biofilm reduction in P. aeruginosa ear infections |
| Probiotic interference | Lactobacillus spp. compete with pathogens, produce biosurfactants, inhibit OM biofilm pathogens |
| Photodynamic therapy (PDT) | Light-activated photosensitisers generate ROS → biofilm eradication on surfaces |
| Gallium (Ga³⁺) | Mimics iron, disrupts iron-dependent metabolism of P. aeruginosa biofilm |
| Biofilm-disrupting coatings | Antibiotic-eluting coatings for tympanostomy tubes, cochlear implants, voice prostheses |
| AI-based prediction | Machine learning to predict biofilm-positive CRS from CT/endoscopy features |
(ICAR 2021, p. 119; Hall-Stoodley et al.; Post et al.; Recent review literature)
12. BIOFILM AND ANTIBIOTIC STEWARDSHIP
- Biofilms are a major driver of antibiotic failure in ENT practice
- Conventional MIC testing done on planktonic bacteria does not reflect in-vivo biofilm resistance
- MBEC (Minimum Biofilm Eradication Concentration) must be used — typically 100–1000× higher than MIC
- Prolonged, high-dose, and topical antibiotic regimens required — but must be balanced against resistance emergence
- Biofilm awareness is central to rational antibiotic stewardship in ENT
13. SUMMARY TABLE — BIOFILM AT A GLANCE
| Feature | Details |
|---|---|
| Definition | Sessile microbial community in self-produced EPS matrix |
| Key property | 100–1000× antibiotic resistance vs planktonic state |
| Communication | Quorum sensing (autoinducers) |
| ENT sites | CRS, COM, OME, tonsils, adenoids, cholesteatoma, medical devices |
| Diagnosis | CSLM (gold standard), SEM, FISH, Crystal violet assay |
| Treatment | Biofilm-active antibiotics + surfactants + surgery + emerging (phage, QSI, nanoparticles) |
| % CRS surgical candidates | Up to 50% biofilm-positive (ICAR 2021) |
| % OME with biofilm | ~92% (Hall-Stoodley) |
| Key outcome | Worse post-ESS outcomes in biofilm-positive patients |
14. KEY REFERENCES
- Scott Brown's Otorhinolaryngology, Head and Neck Surgery — 8th Edition (Gleeson et al.) — Chapters on Rhinosinusitis and Otitis Media
- Cummings Otolaryngology — Head and Neck Surgery — 7th Edition (Flint et al.) — Biofilm in CRS and COM
- Stell and Maran's Head and Neck Surgery — 5th Edition — Biofilm in cholesteatoma and head-neck infections
- Dhingra's Diseases of Ear, Nose and Throat — 7th Edition — Microbiology of COM; biofilm role
- Hazarika's Textbook of Ear, Nose and Throat — 3rd Edition — Clinical relevance of biofilms
- Zakir Hussain's ENT for Entrance Exams — Biofilm quick reference
- ICAR-Rhinosinusitis 2021 (International Forum of Allergy & Rhinology) — pp. 119 — CRS biofilm evidence
- Harrison's Principles of Internal Medicine — 21st Edition, p. 5083 — Microbiology of chronic sinusitis
- Costerton JW et al. (1999) — Bacterial biofilms: A common cause of persistent infections. Science
- Hall-Stoodley L et al. (2006) — Direct detection of bacterial biofilms in OME. JAMA
- Post JC et al. (2004) — Biofilms in otolaryngology. Laryngoscope
- Cryer J et al. (2004) — Evidence of bacterial biofilms in human CRS. ORL
- Hoiby N et al. (2015) — ESCMID guidelines on biofilm infections. Clin Microbiol Infect
QUICK MNEMONICS FOR EXAM
Stages of Biofilm → "A I M D"
- Attachment (initial)
- Irreversible attachment
- Microcolony formation → Maturation
- Dispersal
Biofilm Resistance Mechanisms → "PEACH"
- Persister cells
- EPS barrier
- Altered microenvironment
- Chromosomal gene transfer
- Horizontal resistance gene spread / efflux pumps (Hydrophobic EPS)
Examiner's Note (RGUHS 50-mark format): This answer covers Definition (2), History (2), Microbiology (5), Stages + Diagrams (8), Structure (5), Quorum Sensing + Flowchart (6), Resistance Mechanisms (5), Site-specific ENT significance (8), Diagnosis (4), Treatment (5), Recent Advances (5), Summary/References (5) = 50 marks.
This is a shared conversation. Sign in to Orris to start your own chat.