Cholinergic drugs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer.
Cholinergic Drugs
Cholinergic drugs are agents that mimic, enhance, or prolong the actions of acetylcholine (ACh) at cholinergic synapses. They are broadly divided into direct-acting (act on cholinoceptors themselves) and indirect-acting (inhibit acetylcholinesterase, thereby increasing ACh at the synapse).
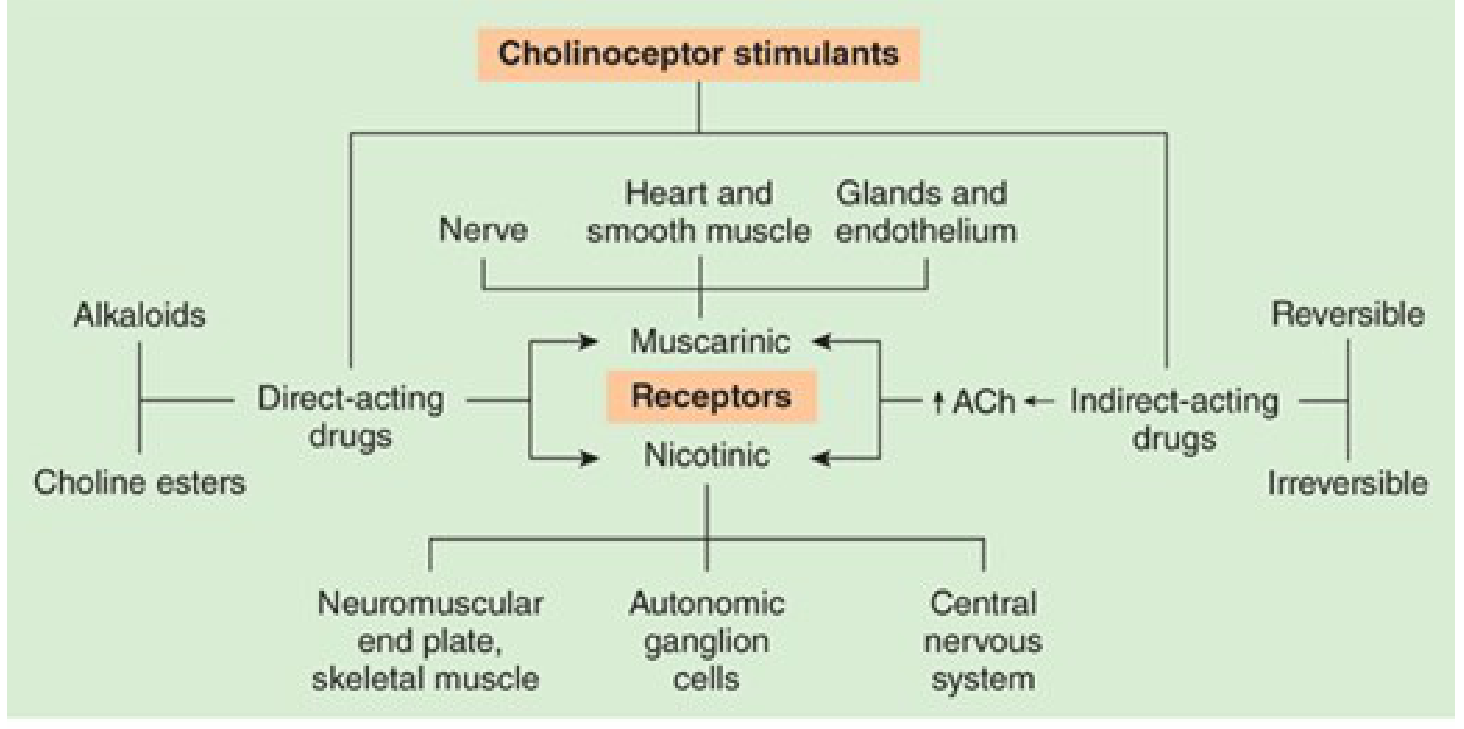
1. Cholinoceptors: The Targets
Two receptor families mediate ACh effects:
Muscarinic Receptors (G protein-coupled, 7-TM)
| Subtype | Location | Signaling | Key Effect |
|---|---|---|---|
| M1 | Nerves, CNS | Gq/11 → IP3, DAG | Slow EPSP in ganglia |
| M2 | Heart, nerves, smooth muscle | Gi/o → ↓cAMP, ↑K⁺ | Bradycardia, decreased contractility |
| M3 | Glands, smooth muscle, endothelium | Gq/11 → IP3, DAG | Secretion, smooth muscle contraction |
| M4 | CNS | Gi/o → ↓cAMP | CNS modulation |
| M5 | CNS | Gq/11 → IP3, DAG | CNS modulation |
Nicotinic Receptors (ligand-gated ion channels, pentameric)
| Subtype | Location | Effect |
|---|---|---|
| NM (muscle type) | Skeletal NMJ | Na⁺/K⁺ depolarization → muscle contraction |
| NN (neuronal type) | Autonomic ganglia, CNS | Na⁺/K⁺ depolarization → ganglionic transmission |
2. Direct-Acting Cholinomimetics
These drugs bind directly to muscarinic and/or nicotinic receptors.
A. Choline Esters
| Drug | Muscarinic | Nicotinic | AChE Hydrolysis | Key Features |
|---|---|---|---|---|
| Acetylcholine | +++ | +++ | Very rapid | No therapeutic use (too short-acting) |
| Methacholine | +++ | + | Slow | Bronchial challenge test |
| Carbachol | ++ | ++ | Resistant | Glaucoma, GI motility |
| Bethanechol | ++ | Minimal | Resistant | Urinary retention, GI atony |
Bethanechol is the most clinically used: given orally (10-25 mg 3-4x/day for GI disorders) or subcutaneously (5 mg for urinary retention). It is resistant to AChE hydrolysis, giving it a longer duration of action than ACh.
B. Cholinomimetic Alkaloids
| Drug | Receptor Selectivity | Key Use |
|---|---|---|
| Pilocarpine | Muscarinic (M3) | Glaucoma (topical), Sjögren syndrome (dry mouth) |
| Muscarine | Muscarinic | Toxin (mushroom poisoning) - no therapeutic use |
| Nicotine | Nicotinic | Smoking cessation |
| Cevimeline | Muscarinic (M1, M3) | Dry mouth in Sjögren syndrome |
Pilocarpine is notable: IV administration can paradoxically cause hypertension via M1 receptor activation at sympathetic ganglia, causing slow EPSP and ganglionic discharge.
3. Indirect-Acting Cholinomimetics (Anticholinesterases)
These drugs inhibit acetylcholinesterase (AChE), the enzyme that hydrolyzes ACh, causing ACh to accumulate at all cholinergic synapses.
A. Reversible (Noncovalent) Inhibitors
| Drug | Key Properties | Uses |
|---|---|---|
| Edrophonium | Quaternary amine, short-acting (minutes), renal elimination | Diagnosis of myasthenia gravis (Tensilon test) |
| Tacrine | Lipophilic, crosses BBB | Alzheimer's disease (largely obsolete due to hepatotoxicity) |
| Donepezil | Lipophilic, crosses BBB, long-acting | Alzheimer's disease (first-line) |
B. Reversible Carbamate Inhibitors
| Drug | Key Properties | Uses |
|---|---|---|
| Physostigmine | Tertiary amine, crosses BBB | Glaucoma (topical), atropine overdose reversal |
| Neostigmine | Quaternary amine, does NOT cross BBB | Myasthenia gravis, postoperative ileus, reversal of NMJ blockade |
| Pyridostigmine | Quaternary amine | Myasthenia gravis (longer-acting than neostigmine) |
| Rivastigmine | Lipophilic, crosses BBB | Alzheimer's disease, Parkinson's dementia |
| Galantamine | Crosses BBB; also allosteric nicotinic modulator | Alzheimer's disease |
Carbamates form a covalent but reversible carbamylated intermediate at the AChE active site (hydrolysis in minutes to hours).
C. Irreversible Organophosphate Inhibitors
These form covalent phosphorylated complexes with AChE that are extremely long-lasting ("aging" locks in the bond over time).
| Drug | Use/Context |
|---|---|
| Echothiophate | Glaucoma (topical) |
| Malathion, Parathion | Agricultural insecticides |
| Sarin, VX, Tabun | Chemical warfare nerve agents |
| Soman | Nerve agent with fastest "aging" |
Treatment of organophosphate poisoning:
- Atropine (0.5-5 mg IV) - blocks muscarinic excess (dyspnea, lacrimation, bradycardia, secretions). Titrate until signs of muscarinic excess resolve.
- Pralidoxime (2-PAM) - reactivates AChE if given before "aging." Initial 1-2% solution IV over 15-30 min, then 1% infusion (200-500 mg/h) until fasciculations cease. Does not enter CNS.
- Oxygen, airway support, decontamination (remove clothing, wash skin).
4. Organ System Effects of Cholinomimetics (DUMBELS/SLUDGE)
| System | Effect |
|---|---|
| Eye | Miosis, accommodation spasm (ciliary contraction → near vision), decreased intraocular pressure |
| Heart | Bradycardia (M2), decreased AV conduction, decreased force (atria) |
| Blood vessels | Vasodilation via endothelial NO release (M3); direct contraction of denervated vessels |
| Lungs | Bronchoconstriction, increased secretions (M3) |
| GI tract | Increased motility, secretions, defecation (M3) |
| Urinary bladder | Detrusor contraction, sphincter relaxation → urination (M3) |
| Glands | Increased salivation, lacrimation, sweating |
| Skeletal muscle | Fasciculations, weakness (NM at NMJ) |
| CNS | Anxiety, seizures (at toxic doses) |
The classic mnemonics:
- SLUDGE: Salivation, Lacrimation, Urination, Defecation, GI distress, Emesis
- DUMBELS: Diarrhea/Diaphoresis, Urination, Miosis, Bradycardia/Bronchospasm, Emesis, Lacrimation, Salivation
5. Clinical Applications Summary
| Indication | Drug of Choice |
|---|---|
| Myasthenia gravis (chronic) | Pyridostigmine |
| Myasthenia gravis (diagnosis) | Edrophonium |
| Alzheimer's disease | Donepezil, rivastigmine, galantamine |
| Glaucoma (acute angle-closure) | Pilocarpine + topical β-blocker |
| Urinary retention / postoperative ileus | Bethanechol, neostigmine |
| Acute colonic pseudo-obstruction (Ogilvie syndrome) | Neostigmine IV 2 mg |
| Dry mouth (Sjögren, radiation) | Pilocarpine, cevimeline |
| Reversal of NMJ blockade (post-anesthesia) | Neostigmine + glycopyrrolate (to block muscarinic side effects) |
| Organophosphate poisoning | Atropine + pralidoxime (2-PAM) |
| Atropine/anticholinergic overdose | Physostigmine |
6. Indirect Modulators of ACh Release
- Amifampridine (3,4-DAP) and 4-aminopyridine (dalfampridine): block K⁺ channels on nerve terminals → prolonged depolarization → increased ACh release. Used in Lambert-Eaton myasthenic syndrome (amifampridine) and multiple sclerosis walking impairment (dalfampridine).
Sources:
- Katzung's Basic & Clinical Pharmacology, 16th Ed. - Chapters 7 & 8 (Cholinomimetics)
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Chapter 12 (Anticholinesterase Inhibitors)
- Katzung's Basic & Clinical Pharmacology, 16th Ed., Chapter 62 (GI pharmacology)
This is a shared conversation. Sign in to Orris to start your own chat.