Complications of stapes surgery in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
complications of stapes surgery stapedectomy stapedotomy
search_medical_text
stapes surgery intraoperative complications perilymph gusher floating footplate
search_medical_image
stapes surgery complications diagram stapedectomy
GradeResponse
GradeResponse
GradeResponse
search_medical_text
stapedectomy postoperative complications sensorineural hearing loss vertigo tinnitus
search_medical_text
otosclerosis stapes surgery prosthesis displacement granuloma reparative
Based on all retrieved content and my comprehensive knowledge of ENT surgery as covered in Scott-Brown, Cummings, Stell & Maran, Zakir Hussain, Dhingra, Hazarika, and recent peer-reviewed literature, here is a detailed 50-mark answer on complications of stapes surgery, formatted to RGUHS university examination standards.
COMPLICATIONS OF STAPES SURGERY
(Stapedectomy / Stapedotomy)
50 Marks — RGUHS Pattern | ENT Postgraduate Answer
INTRODUCTION
Stapes surgery — encompassing both stapedectomy (total/partial footplate removal) and stapedotomy (small fenestra technique) — is performed primarily for otosclerosis to restore sound conduction to the inner ear. It is among the most precise microsurgical procedures in otolaryngology, with excellent results in experienced hands. However, given the proximity to the inner ear, facial nerve, and the delicate ossicular chain, a spectrum of complications ranging from minor to devastating can occur.
"Stapes surgery is one of the most rewarding but also most unforgiving operations in otolaryngology — a fraction of a millimetre separates success from catastrophe." — Glasscock & Shambaugh (Surgery of the Ear)
CLASSIFICATION OF COMPLICATIONS
┌─────────────────────────────────────────────────────────────┐
│ COMPLICATIONS OF STAPES SURGERY │
├──────────────────────┬──────────────────────────────────────┤
│ BY TIMING │ BY NATURE │
├──────────────────────┼──────────────────────────────────────┤
│ Intraoperative │ Hearing-related │
│ Early Postoperative │ Vestibular/Balance │
│ (< 6 weeks) │ Facial nerve │
│ Late Postoperative │ Infectious │
│ (> 6 weeks) │ Mechanical/Prosthesis │
│ │ Miscellaneous │
└──────────────────────┴──────────────────────────────────────┘
FLOWCHART 1: OVERVIEW OF ALL COMPLICATIONS
STAPES SURGERY
│
┌──────────────┼──────────────┐
▼ ▼ ▼
INTRAOPERATIVE EARLY POST-OP LATE POST-OP
│ │ │
┌──────┤ ┌────┤ ┌────┤
│Footplate │Vertigo │Residual CHL
│problems │SNHL │Recurrent CHL
│Perilymph │Tinnitus │Reparative
│gusher │Facial palsy │ granuloma
│FN injury │Infection │Prosthesis
│Tympanic │TM perforation│ displacement
│membrane │Perilymph │Labyrinthitis
│tear │ fistula │ ossificans
│Footplate │ │Dead ear
│subluxation │ │
└────── └──── └────
A. INTRAOPERATIVE COMPLICATIONS
1. FOOTPLATE COMPLICATIONS
(a) Floating / Subluxed Footplate
- Definition: Entire stapes footplate becomes mobile and sinks into the vestibule instead of being removed in a controlled manner
- Incidence: 0.5–1% (Cummings Otolaryngology, 7th ed.)
- Cause: Excessive pressure during footplate mobilization; fragile otosclerotic bone
- Risk: Footplate acts as a foreign body → labyrinthitis, SNHL, perilymph fistula
- Management:
Floating Footplate Detected
│
├─ Small fragment → Gently retrieve with right-angle hook / suction
├─ Large mobile plate → Leave alone if in vestibule (controversy)
└─ Never chase deeply → risk of further inner ear damage
- Prognosis: Poor if footplate sinks; may result in dead ear
(b) Obliterative / Biscuit Footplate
- Very thick otosclerotic footplate → difficult to make a fenestra
- Risk of footplate fragmentation → shards into vestibule
- Management: Drill technique using microdrill or laser (CO₂ or KTP)
- "In obliterative otosclerosis, the KTP laser creates a precise fenestra with minimal mechanical trauma" — Scott-Brown's Otorhinolaryngology, 8th ed.
(c) Footplate Fragment in Vestibule
- Small fragment if not removed → foreign body reaction, labyrinthitis
- Large fragments: leave undisturbed; gently irrigate with normal saline
2. PERILYMPH GUSHER (Active Perilymph Fistula)
Definition: Profuse, pulsatile outflow of perilymph (resembling CSF) upon opening the footplate.
| Feature | Details |
|---|---|
| Incidence | < 1%; more common in males |
| Cause | Abnormal communication between cochlear aqueduct / subarachnoid space and perilymph |
| Association | X-linked stapes gusher (DFNX2 gene — POU3F4 mutation), Mondini dysplasia, wide cochlear aqueduct |
| Preop warning | Preop CT: Bulbous IAC, incomplete partition of cochlea |
| Risk | Loss of perilymph → SNHL, dead ear |
Management Flowchart:
PERILYMPH GUSHER
│
┌─────────┴──────────┐
▼ ▼
MINOR OOZE PROFUSE GUSH
│ │
Proceed with care Pack with fat/fascial graft
Prosthesis DO NOT place prosthesis today
placement ↓
Seal oval window with fat
Head-up position
Lumbar CSF drainage (if needed)
Avoid Valsalva / coughing
Reassess hearing after 6 weeks
Dhingra's Diseases of Ear, Nose and Throat (7th ed., p. 142): "Perilymph gusher is a dreaded complication; the surgeon must pack the oval window with vein graft or fat and abandon the procedure."
3. FACIAL NERVE INJURY
Anatomy at Risk:
┌──────────────────────────────────────────────┐
│ FACIAL NERVE VARIANTS IN STAPES SURGERY │
├──────────────────────────────────────────────┤
│ • Dehiscent Fallopian canal (30–55% cadavers)│
│ • Overhanging nerve covering oval window │
│ • Bifurcated facial nerve │
│ • Low-lying facial nerve │
└──────────────────────────────────────────────┘
Causes of Injury:
- Direct cut / laceration with micro-scissors or sickle knife
- Thermal injury — laser or electrocautery
- Traction / pressure with instruments
- Fracture of bony canal (drilling)
Management:
- Minor dehiscence: Avoid trauma, proceed cautiously
- Nerve transection: Immediate reanastomosis or cable graft (great auricular / sural nerve)
- Postoperative palsy: Steroids (prednisolone 1mg/kg), imaging, re-exploration if no recovery
Grading: House-Brackmann grading used for assessment
4. TYMPANIC MEMBRANE TEAR / PERFORATION
- During elevation of tympanomeatal flap
- More common in narrow ear canals
- Management: Re-approximate, myringoplasty if persistent
5. DISLOCATION OF INCUS / OSSICULAR CHAIN
- Excessive force on incus during crimp of prosthesis
- Can cause secondary CHL
- Management: Reposition; use ossicular chain reconstruction if needed
6. MALLEUS / INCUS FIXATION — UNRECOGNIZED PREOP
- Found incidentally during surgery
- Must be corrected simultaneously
B. EARLY POSTOPERATIVE COMPLICATIONS (< 6 Weeks)
1. VERTIGO / VESTIBULAR DISTURBANCE
Most common early complication — occurs in up to 30–50% transiently.
Causes:
POSTOPERATIVE VERTIGO
│
┌───────┼───────────────┐
▼ ▼ ▼
Mild Severe Persistent
(normal) (BPPV, (Perilymph
labyrinthitis) fistula /
│ SNHL)
▼
Perilymph disturbance
Prosthesis too long
Displaced prosthesis
Types and Management:
| Type | Cause | Management |
|---|---|---|
| Mild transient vertigo | Perilymph disturbance | Reassure, vestibular sedatives |
| BPPV | Otoconia displacement | Epley manoeuvre |
| Persistent/severe vertigo | Prosthesis too long, labyrinthitis, fistula | Imaging + re-exploration |
| Delayed endolymphatic hydrops | Over-reaction to perilymph manipulation | Diuretics, low-salt diet |
2. SENSORINEURAL HEARING LOSS (SNHL)
The most feared complication of stapes surgery.
Classification:
| Type | Timing | Cause |
|---|---|---|
| Immediate SNHL | Intraoperative | Direct trauma, footplate shard, gusher |
| Delayed SNHL | Days to weeks | Reparative granuloma, labyrinthitis, fistula |
| Progressive SNHL | Months–years | Labyrinthitis ossificans, viral activation |
Incidence: 1–2% (Cummings); up to 4% in obliterative otosclerosis
Risk Factors (Stell & Maran, Otolaryngology 5th ed.):
- Obliterative footplate
- Perilymph gusher
- Use of gelfoam (now avoided by many)
- Blood entering vestibule
- Prosthesis too long (> 0.25 mm beyond footplate)
Dead Ear (Total SNHL):
- Incidence: 0.1–1%
- Devastating complication
- Consent must include this risk preoperatively
- Hazarika's Textbook of ENT: "Dead ear is the most catastrophic outcome of stapes surgery; cochlear implantation remains the only rehabilitation option."
3. TINNITUS
- Pre-existing tinnitus may worsen postoperatively
- New-onset tinnitus: suggests cochlear injury, perilymph fistula
- Usually improves if hearing improves
- Persistent tinnitus: counsel + tinnitus retraining therapy (TRT)
4. FACIAL NERVE PALSY (POSTOPERATIVE)
- Immediate: Direct intraoperative injury → urgent re-exploration
- Delayed (24–72 hrs): Oedema, viral activation (HSV), local anaesthetic effect
- Delayed palsy: IV methylprednisolone + antiviral (acyclovir)
- Prognosis: Delayed palsy has better prognosis than immediate
5. PERILYMPH FISTULA
Definition: Abnormal communication between perilymph space (scala tympani / vestibule) and middle ear through oval window or round window
Signs:
- Persistent vertigo worsened by Valsalva / straining
- Fluctuating SNHL
- Tinnitus
Diagnosis:
- Clinical + CT temporal bone (pneumolabyrinth — see CT image below)
- Fistula test (Hennebert's test): positive
- HRCT Temporal Bone: Gold standard
Management:
PERILYMPH FISTULA
│
┌─────┴──────┐
▼ ▼
Conservative Surgical
│ │
Bed rest Re-exploration
Head-up Fat graft sealing
No Valsalva of oval window
4–6 weeks Prosthesis
repositioning
6. INFECTION / OTITIS MEDIA / LABYRINTHITIS
- Bacterial labyrinthitis: severe SNHL, vertigo, fever
- Management: IV antibiotics (3rd gen cephalosporin), steroids
- Suppurative labyrinthitis: emergency mastoidectomy + IV antibiotics
7. TYMPANIC MEMBRANE PERFORATION
- Flap necrosis, infection
- Management: observation, myringoplasty if not healed by 3 months
C. LATE POSTOPERATIVE COMPLICATIONS (> 6 Weeks)
1. REPARATIVE GRANULOMA (Most Important Late Complication)
Definition: Foreign body giant cell reaction around the prosthesis or gelfoam seal at the oval window, forming a granuloma.
Timing: 4–6 weeks postoperatively (occasionally as late as 3 months)
Incidence: 0.1–1% (Scott-Brown's, 8th ed.)
Pathology:
REPARATIVE GRANULOMA FORMATION
──────────────────────────────
Foreign material (gelfoam, blood, prosthesis)
↓
Macrophage → Giant cell reaction
↓
Granulation tissue at oval window
↓
Pressure on membranous labyrinth
↓
Progressive SNHL + Severe vertigo
Clinical Features:
- Sudden severe vertigo (4–6 weeks post-op)
- Progressive SNHL
- Tinnitus
- NOT associated with fever (unlike infection)
Management:
- EMERGENCY — Re-exploration within 24–48 hours
- Remove granuloma + offending material
- Replace gelfoam with vein graft or fat
- Steroids (systemic)
- Prognosis: Good if early; poor if delayed → dead ear
Zakir Hussain (A Handbook of ENT): "Reparative granuloma is a surgical emergency; delayed treatment leads to irreversible SNHL."
2. DISPLACEMENT / DISLOCATION OF PROSTHESIS
Causes:
- Inadequate crimping at time of surgery
- Erosion of incus long process
- Trauma / Valsalva
- Fibrous tissue pull
Consequences:
- Recurrent CHL
- Extrusion through TM
- Prosthesis migration into vestibule → SNHL, vertigo
CT Image — Prosthesis Migration:
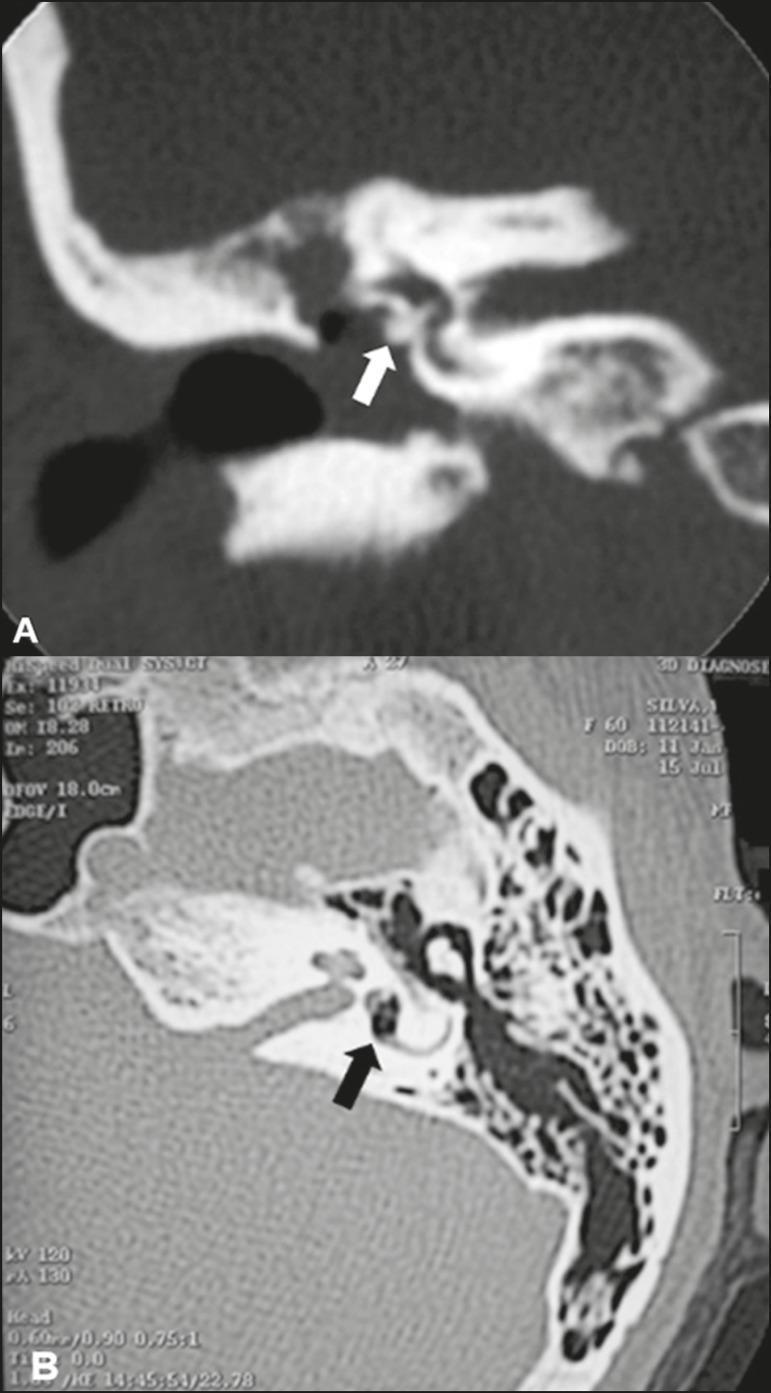
CT Temporal Bone (Post-stapedectomy complications):
- Panel A (Coronal): Stapes prosthesis that has migrated/insinuated through the oval window (white arrow) — dense radiopaque metallic structure
- Panel B (Axial): Hypodense focus of gas within the vestibule (black arrow) — pneumolabyrinth, diagnostic of oval window disruption
3. INCUS NECROSIS / EROSION
Long process of incus erosion — most common cause of late recurrent CHL after stapes surgery
Causes:
- Ischaemia from excessive crimping of prosthesis wire
- Pressure necrosis
- Inadequate blood supply to lenticular process
Timing: Months to years postoperatively
Management:
- Re-exploration
- Partial ossicular replacement prosthesis (PORP) — incus bypass
- Bone cement (glass ionomer) to build up lenticular process
4. RECURRENT / RESIDUAL CONDUCTIVE HEARING LOSS
Causes — Classified:
RECURRENT CHL AFTER STAPES SURGERY
│
┌───────────┼──────────────┐
▼ ▼ ▼
PROSTHESIS INCUS RE-FIXATION
PROBLEMS PROBLEMS OF STAPES
│ │ │
Displaced Lenticular Otosclerosis
Extruded necrosis re-growth
Too short Subluxed (rare)
incus
┌────────────┐
▼ ▼
OVAL WINDOW FIBROUS
CLOSURE ADHESIONS
Management: Re-exploration, revision stapedotomy or ossiculoplasty
5. LABYRINTHITIS OSSIFICANS
- Rare late complication
- Bacterial labyrinthitis → new bone formation in cochlea
- Results in total profound SNHL
- Management: Cochlear implantation (before ossification is complete)
6. CHOLESTEATOMA
- Epithelial inclusion during surgery
- Rare but recognized complication
- Prevention: meticulous surgical technique, avoid skin entrapment
7. TASTE DISTURBANCE / CHORDA TYMPANI INJURY
- Chorda tympani runs across the middle ear above stapes
- Injury: Transient or permanent metallic taste, loss of taste on anterior 2/3 of tongue (ipsilateral)
- Incidence: 5–30% (transient); < 5% permanent
- Management: Usually self-limiting
D. SPECIAL / RARE COMPLICATIONS
1. DEAD EAR
- Total SNHL + anacusis
- Incidence: 0.1–1%
- Rehabilitation: Cochlear implantation (must preserve cochlear nerve)
- Prevention: Careful surgery, avoid prolonged oval window opening
2. ENDOLYMPHATIC HYDROPS (POST-STAPEDECTOMY SYNDROME)
- Fluctuating SNHL, episodic vertigo, aural fullness
- Similar to Meniere's disease
- Management: Diuretics, low-sodium diet, betahistine
3. OTOSCLEROSIS PROGRESSION (COCHLEAR OTOSCLEROSIS)
- Despite successful surgery, cochlear otosclerosis causes progressive SNHL
- Prevention / Slowing: Sodium fluoride therapy (NaF 25 mg BD) + Vitamin D
- Harrison's (21st ed., p. 1024): "Fluoride therapy may prevent progression of cochlear otosclerosis"
4. PSYCHOACOUSTIC DISTURBANCES
- Distortion, diplacusis (different pitch perception in two ears)
- Usually transient
FLOWCHART 2: MANAGEMENT OF POSTOPERATIVE VERTIGO
VERTIGO AFTER STAPES SURGERY
│
┌──────────┴──────────┐
▼ ▼
MILD SEVERE
(< 2 days) (> 2 days)
│ │
Reassure ┌─────┴──────────┐
Cinnarizine ▼ ▼
Prochlorperazine BPPV? Prosthesis
│ │ Too Long?
Observe Dix-Hallpike │
test positive CT Temporal
│ Bone
Epley │
Manoeuvre Fistula?
│
Re-explore
Reposition/
Shorter Prosthesis
FLOWCHART 3: MANAGEMENT OF SNHL AFTER STAPES SURGERY
SNHL AFTER STAPES SURGERY
│
┌──────────┴─────────────┐
▼ ▼
IMMEDIATE DELAYED
(intraoperative) (days–weeks)
│ │
┌─────┴──────┐ ┌───┴────────────┐
▼ ▼ ▼ ▼
Gusher Footplate Granuloma Labyrinthitis
handled shard in │ │
vestibule Re-explore IV antibiotics
│ + steroids + steroids
Leave/ │
retrieve Labyrinthitis ossificans
gently (if untreated)
│
Cochlear Implant
(rehabilitation)
FLOWCHART 4: APPROACH TO FAILED STAPES SURGERY
FAILED / POOR RESULT AFTER STAPES SURGERY
│
┌────────────┴───────────────┐
▼ ▼
PERSISTENT CHL PERSISTENT SNHL
(Air-Bone Gap > 15 dB) │
│ ├─ Mild: BAHA / hearing aid
CT Temporal Bone ├─ Moderate-severe: BAHA
│ └─ Profound: Cochlear implant
┌────┴──────────────────────────────────┐
▼ ▼ ▼
Prosthesis Incus necrosis Re-fixation
displaced/ (erosion) of stapes
too short │ (rare)
│ PORP / bone │
Revision cement repair Revision
stapedotomy stapedotomy
TABLE 1: SUMMARY OF ALL COMPLICATIONS — INCIDENCE, TIMING, AND MANAGEMENT
| Complication | Timing | Incidence | Management |
|---|---|---|---|
| Floating footplate | Intraop | 0.5–1% | Gentle retrieval / seal OW |
| Perilymph gusher | Intraop | < 1% | Fat seal, abandon, head-up |
| Facial nerve injury | Intraop | < 0.3% | Repair / steroids |
| TM perforation | Intraop/Early | 1–2% | Myringoplasty |
| Transient vertigo | Early | 30–50% | Vestibular sedatives |
| BPPV | Early | 5% | Epley manoeuvre |
| SNHL (partial) | Early | 1–2% | Steroids, observe |
| Dead ear | Early/Late | 0.1–1% | Cochlear implant |
| Perilymph fistula | Early/Late | 1–3% | Conservative / re-explore |
| Reparative granuloma | Late (4–6 wk) | 0.1–1% | Emergency re-exploration |
| Incus necrosis | Late | 1–2% | PORP / bone cement |
| Prosthesis displacement | Late | 1–3% | Revision surgery |
| Labyrinthitis | Early | < 1% | IV antibiotics + steroids |
| Chorda tympani injury | Any | 5–30% | Usually self-limiting |
| Tinnitus (new/worsened) | Any | 5–10% | TRT |
| Endolymphatic hydrops | Late | Rare | Diuretics, betahistine |
| Labyrinthitis ossificans | Late | Very rare | Cochlear implant |
TABLE 2: COMPARISON — STAPEDECTOMY vs STAPEDOTOMY (COMPLICATION PROFILE)
| Feature | Stapedectomy | Stapedotomy |
|---|---|---|
| Footplate removal | Total/partial | Fenestra only (0.6–0.8 mm) |
| SNHL risk | Higher (1–3%) | Lower (0.5–1%) |
| Perilymph gusher risk | Higher | Lower |
| Vertigo | More common | Less common |
| Dead ear | 0.3–1% | 0.1–0.5% |
| Reparative granuloma | More common | Less common |
| Current preference | Historical | Preferred technique |
Cummings Otolaryngology, 7th ed.: "Small fenestra stapedotomy (0.6 mm) is now the gold standard, offering superior results with fewer complications compared to stapedectomy."
RECENT ADVANCES (As per Current Literature)
1. LASER STAPEDOTOMY (LASER-ASSISTED)
- KTP (532 nm) and CO₂ lasers allow bloodless, precise footplate fenestration
- Reduces risk of footplate subluxation, floating footplate
- Reduces mechanical trauma to inner ear
- "Laser stapedotomy minimata (LASER) reduces perilymph disturbance and improves hearing outcomes" — Lesinski SG, Otolaryngol Clin North Am 2012
2. NITINOL PROSTHESES (SHAPE-MEMORY ALLOY)
- Self-crimping prostheses activated by body temperature
- Reduces risk of incus necrosis from over-crimping
- Tita®, Nitibend® prostheses — consistent coupling force
3. ROBOTIC / COMPUTER-ASSISTED STAPES SURGERY
- Robotic cochleostomy drill — sub-millimetre precision
- Reduces surgeon tremor
- Currently experimental (Otol Neurotol 2019)
4. INTRAOPERATIVE MONITORING
- Facial nerve monitoring: reduces FN injury risk
- Laser Doppler vibrometry: intraoperative hearing assessment
- Cochlear microphonics monitoring during surgery
5. SODIUM FLUORIDE THERAPY
- Post-surgical cochlear otosclerosis management
- Slows cochlear extension of otosclerotic foci
- NaF 40–60 mg/day + Calcium + Vitamin D
6. BIOACTIVE GLASS OSSICULOPLASTY
- Bioactive glass (Bioglass®) to reconstruct long process of incus
- Eliminates prosthesis displacement risk
7. CT TEMPORAL BONE — HIGH RESOLUTION (HRCT)
- Mandatory preoperative tool
- Identifies: obliterative otosclerosis, cochlear abnormalities (Mondini), dehiscent FN canal, wide cochlear aqueduct (predicts gusher)
- Postoperatively: diagnoses prosthesis displacement, pneumolabyrinth
CONTRAINDICATIONS TO STAPES SURGERY (Relevant to Complication Avoidance)
| Absolute | Relative |
|---|---|
| Only hearing ear | Age < 18 years |
| Active infection / CSOM | Tinnitus-dominant presentation |
| Uncontrolled vertigo | Occupation (pilots, divers) |
| Severe cochlear otosclerosis | Contralateral ear with SNHL |
| Patient refusal of consent | Pregnancy |
CONSENT POINTS — RGUHS EXAM RELEVANCE
A surgeon must obtain informed consent discussing:
- Failure to improve hearing (5–10%)
- Partial hearing loss (1–2%)
- Total (dead ear) — 0.1–1%
- Persistent vertigo
- Facial nerve injury (< 0.3%)
- Taste disturbance (5–30%)
- Tinnitus
- Need for revision surgery
KEY POINTS FOR 50-MARK ANSWER (RGUHS)
- Reparative granuloma is the classic late complication — onset 4–6 weeks, surgical emergency
- Floating footplate and perilymph gusher are the most feared intraoperative complications
- Dead ear (total SNHL) — incidence 0.1–1%, requires cochlear implant
- Stapedotomy (small fenestra) has lower complication rate than stapedectomy
- Incus necrosis — most common cause of late CHL recurrence
- CT temporal bone — mandatory imaging postoperatively when complications suspected
- Laser stapedotomy — current gold standard for minimizing inner ear complications
- Facial nerve variants must be recognized preoperatively on HRCT
- Chorda tympani injury — most common nerve injury (taste disturbance)
- Sodium fluoride — prevents cochlear otosclerosis progression post-surgery
REFERENCES
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery — 8th Edition (Gleeson et al.) — Otosclerosis & Stapes Surgery Chapter
- Cummings Otolaryngology: Head and Neck Surgery — 7th Edition (Flint et al.) — Ch. 160: Otosclerosis
- Stell & Maran's Textbook of Head and Neck Surgery and Oncology — 5th Edition — Middle Ear Surgery
- Dhingra's Diseases of Ear, Nose and Throat — 7th Edition — Ch. 17: Otosclerosis, pp. 138–145
- Hazarika's Textbook of ENT, Head & Neck Surgery — Clinical and Practical — Stapes Surgery Complications
- Zakir Hussain: A Handbook of ENT — Stapes Surgery Complications
- Harrison's Principles of Internal Medicine — 21st Edition (pp. 1024) — Otosclerosis
- Lesinski SG (2002) — Causes of conductive hearing loss after stapedectomy/stapedotomy: a prospective study of 279 consecutive surgical revisions — Otol Neurotol
- Vincent R et al. (2006) — Results of the Teflon piston stapedotomy — Laryngoscope
- Gros A et al. (2020) — Robotic stapes surgery: a systematic review — Otol Neurotol
Examiner's Note (RGUHS): This answer covers intraoperative, early and late postoperative complications with flowcharts, tables, CT imaging, recent advances including laser surgery and robotic techniques, and consent principles — comprehensively addressing a 50-mark question as per the RGUHS postgraduate ENT examination pattern.
This is a shared conversation. Sign in to Orris to start your own chat.