fully detailed structred notes on ascending tracts ( use standard physiology books as your source)
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Now I have comprehensive information from multiple authoritative textbooks. Let me compile the fully detailed structured notes.
Ascending Tracts of the Spinal Cord
Fully Detailed Structured Notes
Sources: Guyton & Hall Medical Physiology; Neuroanatomy through Clinical Cases (Blumenfeld); Gray's Anatomy for Students; Adams & Victor's Principles of Neurology; Localization in Clinical Neurology (Brazis); Neuroscience: Exploring the Brain (Bear et al.)
Overview
Sensory information from the periphery ascends to the brain via two major systems:
| System | Location in Cord | Modalities | Consciousness |
|---|---|---|---|
| Dorsal Column-Medial Lemniscal (DCML) | Posterior funiculus | Fine touch, vibration, proprioception, pressure discrimination | Conscious |
| Anterolateral System | Anterolateral funiculus | Pain, temperature, crude touch, tickle, itch, sexual sensation | Conscious |
| Spinocerebellar Tracts | Lateral funiculus | Proprioception, muscle spindle/Golgi tendon organ signals | Subconscious |
The spinal cord cross-section diagram below shows the location of all major ascending tracts:
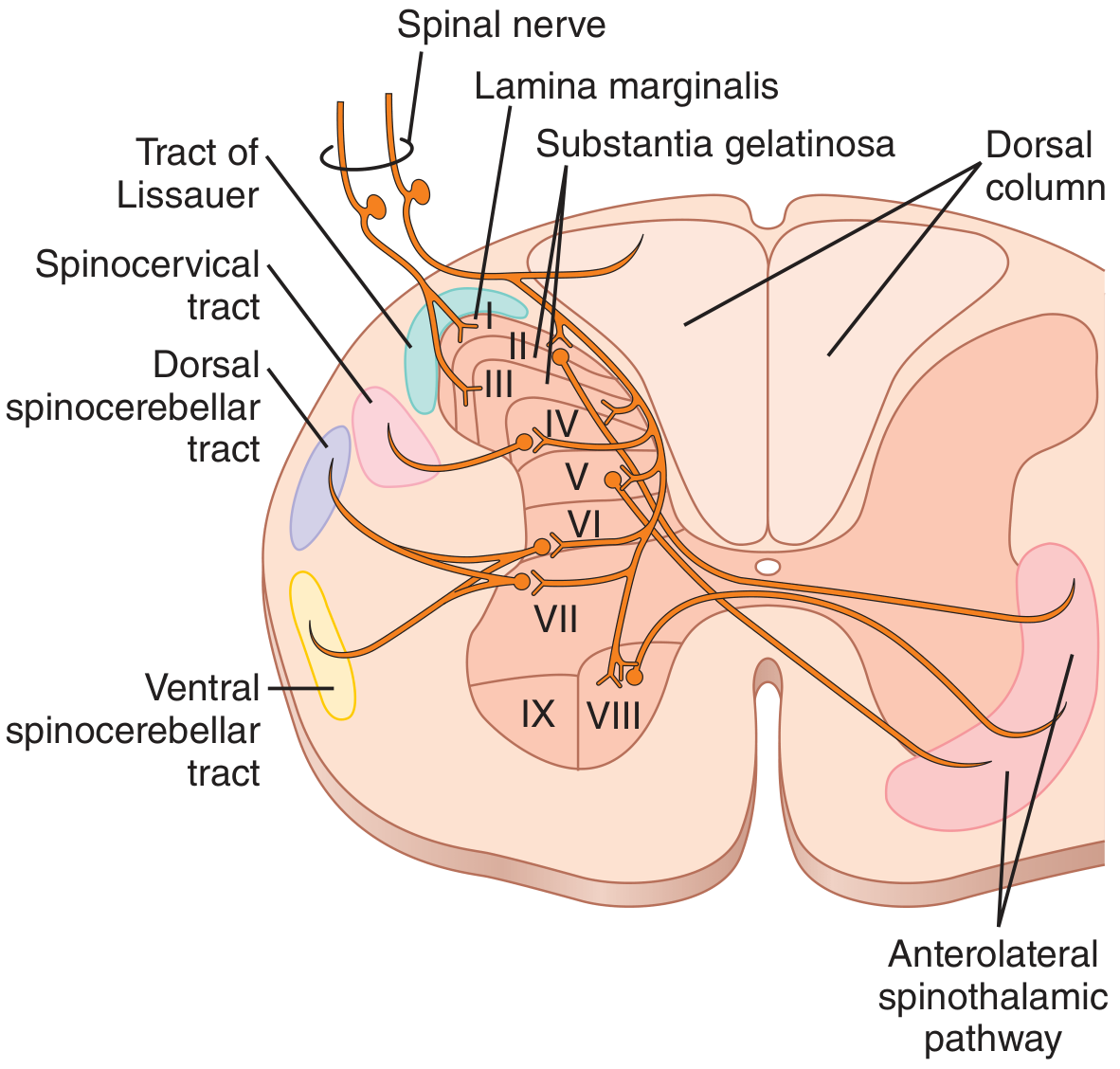
I. Dorsal Column-Medial Lemniscal (DCML) System
A. Modalities Carried
(Guyton & Hall, Ch. 48)
- Touch sensations requiring high degree of localization
- Fine gradations of touch intensity
- Vibratory (phasic) sensations
- Sensations of movement against the skin
- Joint position sense (conscious proprioception)
- Fine pressure discrimination
- Two-point discrimination, stereognosis, graphesthesia
B. First-Order Neurons (Primary Afferents)
- Cell bodies: Dorsal root ganglion (spinal ganglion cells) - pseudounipolar neurons
- Fiber type: Large, heavily myelinated A-beta fibers (Group II)
- Entry: Medial bundle of the dorsal root
- Behavior on entry: On entering the spinal cord, each large fiber bifurcates into a medial branch and a lateral branch
- The medial branch immediately turns upward in the dorsal column, ascending all the way to the dorsal medulla WITHOUT synapsing
- The lateral branch enters the dorsal horn and synapses locally (for reflexes and to give rise to some spinocerebellar fibers)
C. Fascicular Organization (Somatotopy)
The dorsal columns are divided into two named fasciculi:
| Fasciculus | Also Called | Spinal Levels of Origin | Location in Dorsal Column | Nucleus in Medulla |
|---|---|---|---|---|
| Fasciculus gracilis | Goll's column | Sacral, lumbar, lower 6 thoracic (T7-T12) - lower body | Medial | Nucleus gracilis |
| Fasciculus cuneatus | Burdach's column | Upper 6 thoracic (T1-T6) and all cervical - upper body, arms | Lateral | Nucleus cuneatus |
Key rule (Localization in Clinical Neurology): Fibers from lower parts of the body lie toward the center of the cord; those entering at progressively higher levels form successive layers laterally.
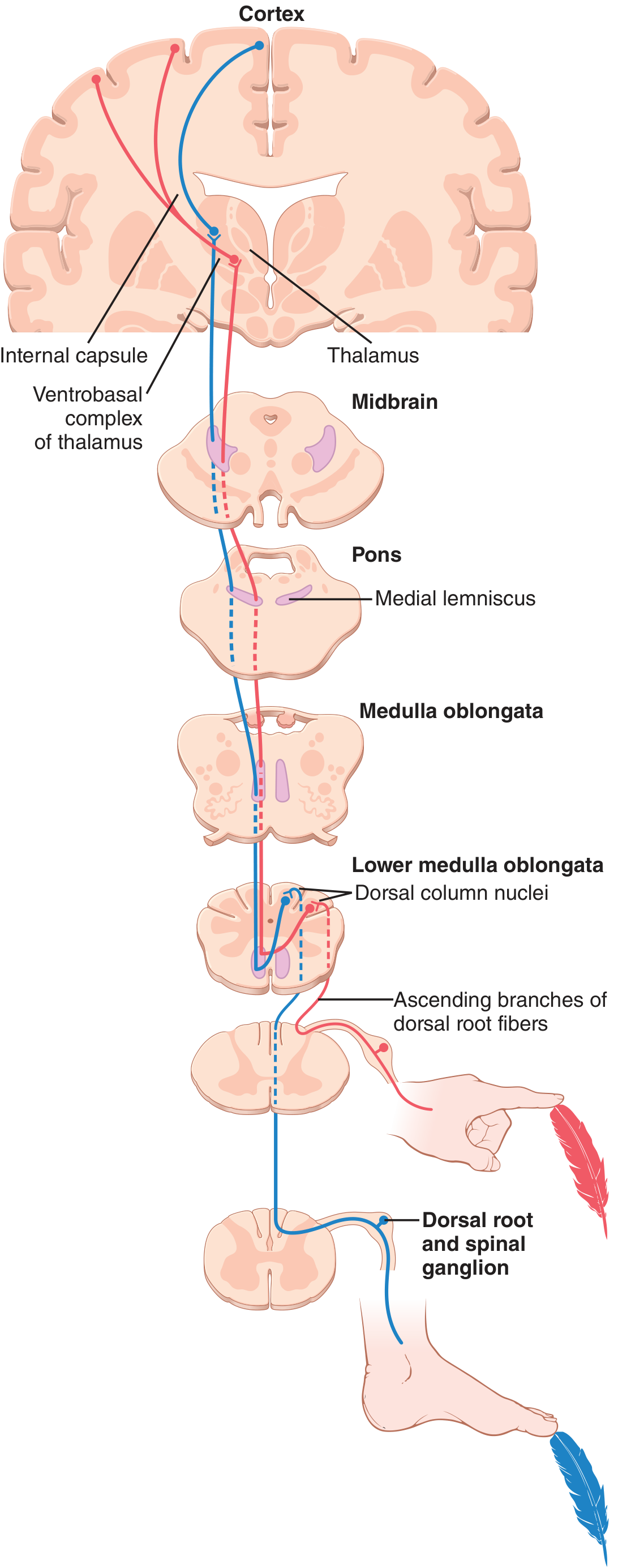
D. Second-Order Neurons
- Cell bodies: Nucleus gracilis and nucleus cuneatus in the caudal medulla
- Axonal behavior: These axons cross the midline as internal arcuate fibers (decussation in the lower medulla)
- After crossing, they form the medial lemniscus on the contralateral side
- The medial lemniscus ascends through medulla, pons, and midbrain, picking up additional fibers from the trigeminal sensory nuclei (for the face) along the way
- Position of medial lemniscus:
- In the medulla: vertical, paramedian
- In the pons: rotates to a horizontal orientation
- In the midbrain: lateral tegmentum
- Somatotopy in the thalamus: Lower limb = most lateral VPL; upper limb = more medial; face = VPM (ventral posteromedial nucleus)
E. Third-Order Neurons
- Cell bodies: Ventral posterolateral nucleus (VPL) of the thalamus
- Projection: Via the posterior limb of the internal capsule → primary somatosensory cortex (postcentral gyrus, Brodmann areas 3, 1, and 2)
- Left side of body → right thalamus and right cortex (due to decussation in medulla)
Diagram - DCML pathway from spinal cord to cortex (Guyton & Hall):
II. Anterolateral System
The anterolateral system consists of three tracts, all running in the anterolateral white matter. They share a common first-order neuron arrangement but differ in their second-order targets.
A. Modalities Carried (Guyton & Hall)
- Pain (sharp and dull/diffuse)
- Thermal sensations (warm and cold)
- Crude touch and pressure (with only coarse localization)
- Tickle and itch sensations
- Sexual sensations
II-A. Lateral Spinothalamic Tract (Neospinothalamic Tract)
This is the primary, fast pain and temperature pathway.
First-Order Neurons
- Cell bodies: Dorsal root ganglion
- Fiber types: Aδ (thinly myelinated, sharp/fast pain + cold) and C fibers (unmyelinated, slow/burning pain + warmth)
- Entry: Lateral bundle of the dorsal root → enter Lissauer's tract (posterolateral tract of Lissauer) where axon collaterals ascend or descend 1-2 spinal segments before synapsing
- Synaptic targets in dorsal horn: Lamina I (marginal zone) and Lamina V (deeper dorsal horn)
Second-Order Neurons
- Cell bodies: Predominantly laminae I and V of the dorsal horn
- Decussation: Axons cross obliquely through the anterior (ventral) white commissure, traveling over 2-3 spinal cord segments to the contralateral side
- After crossing, they ascend in the anterolateral white matter as the lateral spinothalamic tract
- Somatotopic organization (important clinically):
- Sacral fibers = most lateral/posterior
- Cervical fibers = most medial/anterior
- New fibers from higher levels add on medially as they join
- The tract passes through the medulla (lateral aspect, between the inferior olive and inferior cerebellar peduncle), pons (just lateral to medial lemniscus), and midbrain
- Terminates in: VPL nucleus of thalamus
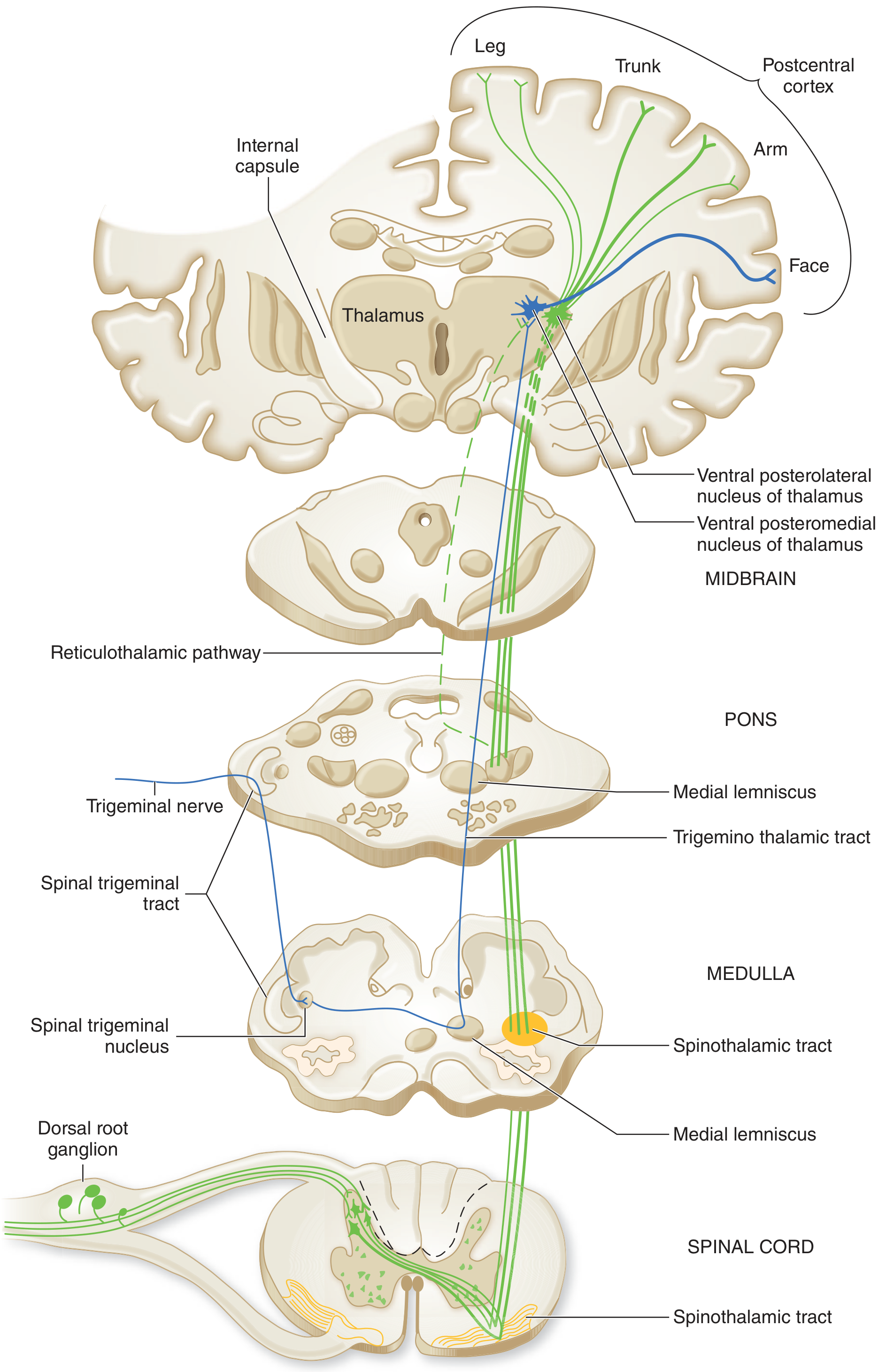
Third-Order Neurons
- VPL → posterior limb of internal capsule → primary somatosensory cortex (postcentral gyrus, areas 3,1,2)
- This pathway conveys discriminative aspects of pain: location, quality, and intensity (the "sensory-discriminative" component)
- Also projects to VPI (ventral posterior inferior nucleus) and posterior thalamus
Diagram - Spinothalamic and trigeminothalamic tracts with brainstem nuclei (Adams & Victor):
II-B. Spinoreticulothalamic Tract (Paleospinothalamic Pathway)
(Adams & Victor; Neuroanatomy through Clinical Cases)
- Fibers run medial to the neospinothalamic tract in the anterolateral funiculus
- Second-order axons do NOT go directly to thalamus. Instead they terminate on:
- Nucleus gigantocellularis (medullary reticular formation)
- Parabrachial nuclei (pons)
- Periaqueductal gray (PAG) matter
- Hypothalamus
- Intralaminar and medial thalamic nuclei (centromedian nucleus), NOT VPL
- From intralaminar nuclei → diffuse projections to entire cerebral cortex and limbic system
- Function: Conveys the affective-motivational component of pain (the unpleasant emotional quality), behavioral arousal, and the experience of diffuse, poorly localized pain from deep and visceral structures (gut, peritoneum, periosteum)
- Also thought to subserve autonomic responses to pain
II-C. Spinomesencephalic Tract (Spinotectal Tract)
- Second-order axons terminate on:
- Periaqueductal gray (PAG) matter of the midbrain
- Superior colliculi (tectum)
- Function: Central modulation of pain (PAG is the key site of endogenous opioid-mediated analgesia); also mediates reflex orientation responses to noxious stimuli (via superior colliculus)
II-D. Ventral Spinothalamic Tract
(Localization in Clinical Neurology; Gray's Anatomy for Students)
- Distinct from the lateral spinothalamic but travels in the same anterolateral region
- Carries light (crude) touch
- First-order fibers enter, bifurcate in Lissauer's zone, synapse on dorsal horn neurons (laminae VI and VII)
- Second-order neurons cross via ventral white commissure → ascend as ventral spinothalamic tract
- Terminates in VPL thalamus
- Note: Light touch is therefore carried by BOTH the ventral spinothalamic tract AND the dorsal columns-medial lemniscal pathway. This is why pure dorsal column lesions do not abolish light touch completely.
Summary Table: Anterolateral Tracts
| Tract | Modality | 2nd-Order Target | Key Function |
|---|---|---|---|
| Lateral spinothalamic (neospinothalamic) | Sharp pain, temp, crude touch | VPL thalamus → cortex | Discriminative (location, quality, intensity) |
| Spinoreticulothalamic (paleospinothalamic) | Diffuse/slow pain, visceral pain | Reticular formation → intralaminar thalamus → limbic | Affective-motivational, arousal, suffering |
| Spinomesencephalic | Nociception | PAG, superior colliculus | Endogenous pain modulation, reflex orientation |
| Ventral spinothalamic | Light/crude touch | VPL thalamus → cortex | Crude tactile localization |
III. Spinocerebellar Tracts
These tracts transmit unconscious proprioceptive and somatosensory information to the cerebellum for coordination of movement. They operate entirely below the level of consciousness. There are four tracts total: two for the lower extremity and two for the upper extremity.
Key concept (Guyton & Hall): Spinocerebellar pathways can transmit impulses at velocities up to 120 m/sec - the fastest conduction speed in the entire CNS. This speed is necessary for instantaneous feedback to the cerebellum during movement.
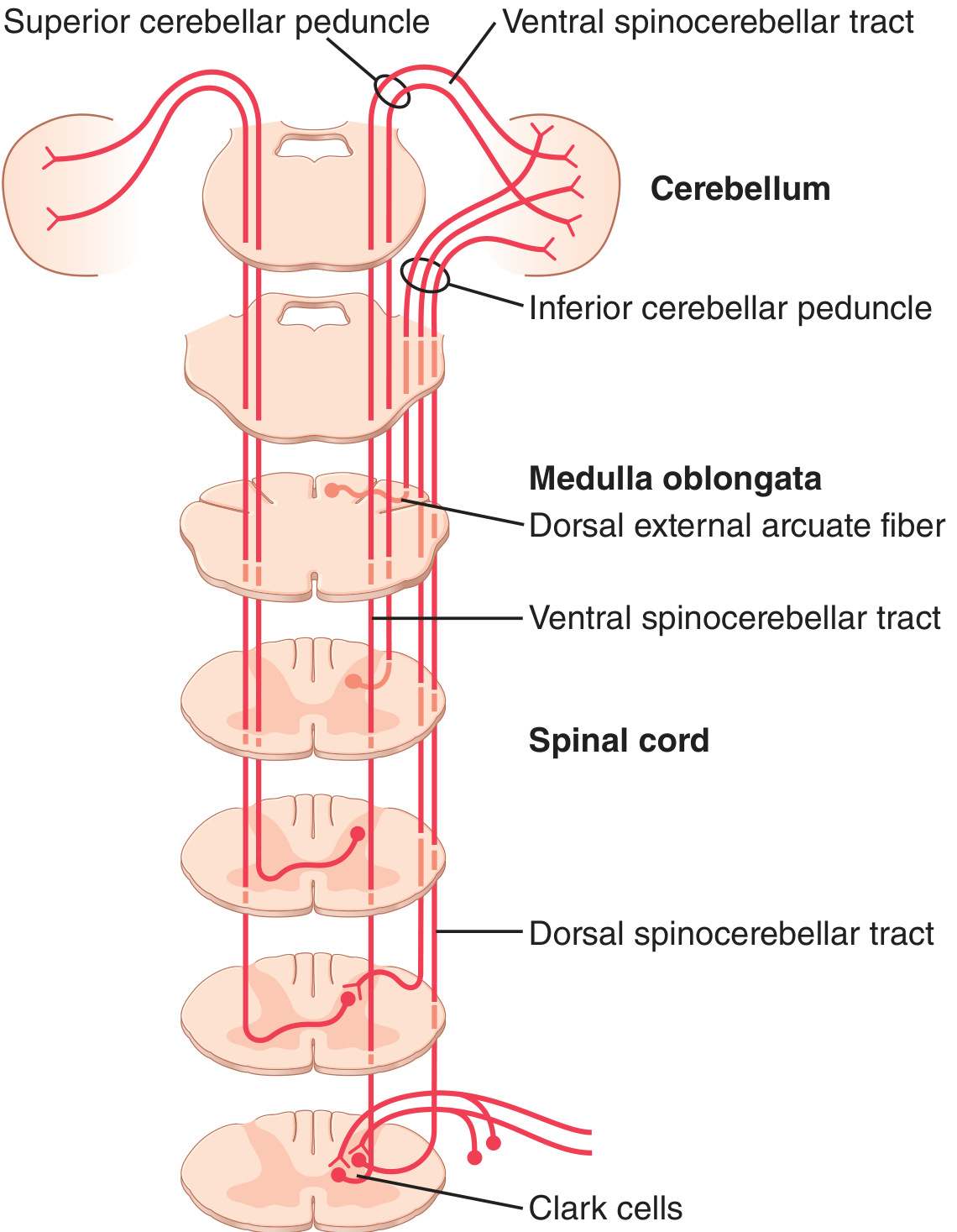
III-A. Dorsal Spinocerebellar Tract (DSCT)
(Neuroanatomy through Clinical Cases; Guyton & Hall)
- Lower extremity equivalent
- Origin of first-order signals: Muscle spindles, Golgi tendon organs, large tactile receptors of skin, and joint receptors - all from the lower extremities and trunk
- First-order neuron cell bodies: Dorsal root ganglion. Large-diameter proprioceptive fibers enter via dorsal root → ascend briefly in the fasciculus gracilis
- Second-order neuron cell bodies: Nucleus dorsalis of Clark (Clarke's column), a column of cells in the dorsomedial intermediate zone of the spinal cord, present from C8 to L2-L3
- Signals from below L2 must first ascend in the fasciculus gracilis to reach Clarke's column
- Course: Fibers from Clarke's column do NOT cross; they ascend ipsilaterally in the dorsolateral funiculus (lateral to the lateral corticospinal tract)
- Peduncle: Enters the cerebellum via the inferior cerebellar peduncle (restiform body)
- Termination: Ipsilateral cerebellar vermis and intermediate hemisphere
- Function: Provides the cerebellum with rapid feedback about the momentary status of: (1) muscle contraction, (2) tendon tension, (3) positions and rates of body movement, (4) forces acting on body surfaces
III-B. Cuneocerebellar Tract
- Upper extremity equivalent of the DSCT
- Origin: Proprioceptors and mechanoreceptors from the upper extremities and neck
- First-order neurons: Large-diameter fibers enter dorsal roots → ascend ipsilaterally in the fasciculus cuneatus
- Second-order neuron cell bodies: External (accessory/lateral) cuneate nucleus in the medulla (located just lateral and rostral to the main cuneate nucleus); this is the upper-extremity analog of Clarke's column
- Course: Fibers ascend ipsilaterally as cuneocerebellar fibers
- Peduncle: Enters the cerebellum via the inferior cerebellar peduncle
- Termination: Ipsilateral cerebellum
Both DSCT and cuneocerebellar tracts reach the ipsilateral cerebellum - this explains why cerebellar lesions cause ipsilateral limb ataxia.
III-C. Ventral Spinocerebellar Tract (VSCT)
(Neuroanatomy through Clinical Cases; Guyton & Hall)
- Lower extremity equivalent - carries interneuronal/efference copy signals
- Origin: Does NOT primarily carry peripheral sensory input. Receives signals from:
- Spinal cord interneurons reflecting activity in descending motor pathways (corticospinal, rubrospinal)
- Internal spinal motor pattern generators
- These signals constitute the "efference copy" of anterior horn motor drive
- Second-order neuron cell bodies: "Spinal border cells" along the outer edge of the central gray matter, and scattered neurons in the intermediate zone (lamina VII)
- Course: Axons cross in the ventral commissure → ascend in the ventral spinocerebellar tract (just ventral to DSCT, peripheral to anterolateral systems)
- Peduncle: Enters the cerebellum via the superior cerebellar peduncle → then crosses back again (second decussation) to reach the cerebellum ipsilateral to where the pathway began
- Net result: "Double-crossed" = information arrives ipsilaterally to the cerebellum
- Function: Tells the cerebellum which motor commands have arrived at the anterior horns
III-D. Rostral Spinocerebellar Tract (RSCT)
- Upper extremity equivalent of the VSCT
- Least well characterized of the four spinocerebellar tracts
- Carries information about activity of spinal interneurons for the upper extremity
- Enters the cerebellum via both the inferior and superior cerebellar peduncles
Summary Table: Spinocerebellar Tracts
| Tract | Extremity | First-Order Relay Nucleus | Peduncle to Cerebellum | Decussation | Primary Input |
|---|---|---|---|---|---|
| Dorsal spinocerebellar (DSCT) | Lower | Clarke's column (C8-L2) | Inferior cerebellar peduncle | None (ipsilateral) | Muscle spindles, GTO, skin receptors |
| Cuneocerebellar | Upper | External cuneate nucleus (medulla) | Inferior cerebellar peduncle | None (ipsilateral) | Muscle spindles, GTO (arm, neck) |
| Ventral spinocerebellar (VSCT) | Lower | Spinal border cells (lamina VII) | Superior cerebellar peduncle | Double-crossed (net ipsilateral) | Spinal interneurons, efference copy |
| Rostral spinocerebellar (RSCT) | Upper | Spinal cord neurons | Inferior + superior cerebellar peduncles | Net ipsilateral | Spinal interneurons (arm) |
Diagram - Dorsal and Ventral Spinocerebellar Tracts (Guyton & Hall):
IV. Additional Minor Ascending Tracts
(Localization in Clinical Neurology; Adams & Victor)
Spinoreticular Tract
- Travels in the anterolateral funiculus
- Projects to the reticular formation of the brainstem
- Relays to intralaminar thalamic nuclei (centromedian nucleus)
- Functions in pain modulation, arousal; overlaps significantly with paleospinothalamic fibers
- May be collaterals of spinothalamic fibers or an independent system (debate remains)
Spinohypothalamic Tract
- Direct pathway in the anterolateral funiculus to the hypothalamus
- Mediates autonomic and neuroendocrine responses to pain and noxious stimuli (e.g., stress hormones, cardiovascular changes)
Spinocervical Tract
- Ascends in the dorsolateral funiculus (visible in the spinal cord cross-section image above)
- First-order neurons synapse in dorsal horn; second-order neurons ascend to the lateral cervical nucleus (C1-C2)
- From there, fibers cross and join the medial lemniscus → VPL thalamus
- Carries tactile and proprioceptive information; well developed in some mammals, less prominent in humans
Spino-Olivary Tract
- Carries signals from cutaneous and proprioceptive receptors to the inferior olivary nucleus
- Inferior olive then relays to the cerebellum via climbing fibers (inferior cerebellar peduncle)
V. Comparative Summary of Major Systems
| Feature | DCML | Lateral Spinothalamic | Spinocerebellar |
|---|---|---|---|
| Modality | Fine touch, vibration, proprioception | Pain, temperature | Unconscious proprioception |
| First synapse | Nucleus gracilis/cuneatus (medulla) | Dorsal horn (laminae I, V) | Clarke's column / ext. cuneate |
| Decussation site | Lower medulla (internal arcuate fibers) | Spinal cord (ant. commissure), 2-3 levels above entry | None (DSCT) or double-cross (VSCT) |
| Side of ascent | Ipsilateral in cord, contralateral in brainstem | Contralateral from entry level | Ipsilateral (net) |
| Thalamic relay | VPL (ventrobasal complex) | VPL + intralaminar nuclei | None (terminates in cerebellum) |
| Cortical destination | Somatosensory cortex (areas 3,1,2) | Somatosensory cortex + limbic | None (subconscious) |
| Clinical lesion effect | Loss of vibration, proprioception, 2-point discrimination ipsilateral below lesion | Loss of pain + temperature contralateral, 2-3 levels below lesion | Ipsilateral limb ataxia |
VI. Clinical Correlations
Brown-Séquard Syndrome (Hemisection of spinal cord)
- Ipsilateral below lesion: Loss of DCML modalities (fine touch, vibration, proprioception) + ipsilateral motor weakness (UMN)
- Contralateral below lesion: Loss of pain and temperature (spinothalamic crosses 2-3 segments above, so loss begins 2-3 levels below lesion)
- Crude touch preserved bilaterally (dual pathway)
Syringomyelia
- Central canal expansion disrupts crossing fibers in the anterior commissure
- Bilateral loss of pain and temperature at the affected levels (cape distribution in cervical syrinx)
- DCML and motor pathways initially spared (suspended sensory loss)
Subacute Combined Degeneration (Vit. B12 deficiency)
- Demyelination of dorsal columns and lateral corticospinal tracts
- Loss of vibration, proprioception, two-point discrimination (DCML modalities)
- Positive Romberg sign
Tabes Dorsalis (neurosyphilis)
- Selective degeneration of dorsal roots and dorsal columns
- Loss of DCML modalities: vibration, proprioception, ataxia
- Lancinating ("lightning") pains despite dorsal column degeneration (via surviving spinothalamic fibers)
Sources: Guyton & Hall Textbook of Medical Physiology (14e); Neuroanatomy through Clinical Cases, 3rd Ed. (Blumenfeld); Gray's Anatomy for Students; Adams & Victor's Principles of Neurology, 12th Ed.; Localization in Clinical Neurology, 8th Ed. (Brazis et al.)
This is a shared conversation. Sign in to Orris to start your own chat.