Hi
Hi! How can I help you today?
WBCs and It's types
Reading File
Finding Sources
Searching Images
types of white blood cells leukocytes diagram
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of White Blood Cells (WBCs) / Leukocytes and their types:
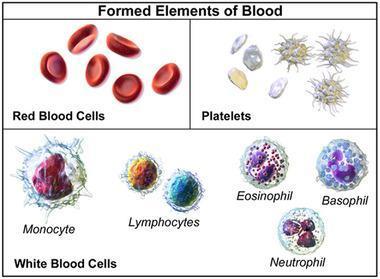
White Blood Cells (Leukocytes)
WBCs leave the blood and migrate to tissues where they perform various activities related to immunity. There are normally 4,500–11,000 leukocytes/µL of blood in adults (higher in infants and young children).
They are divided into two major groups based on the presence of cytoplasmic granules:
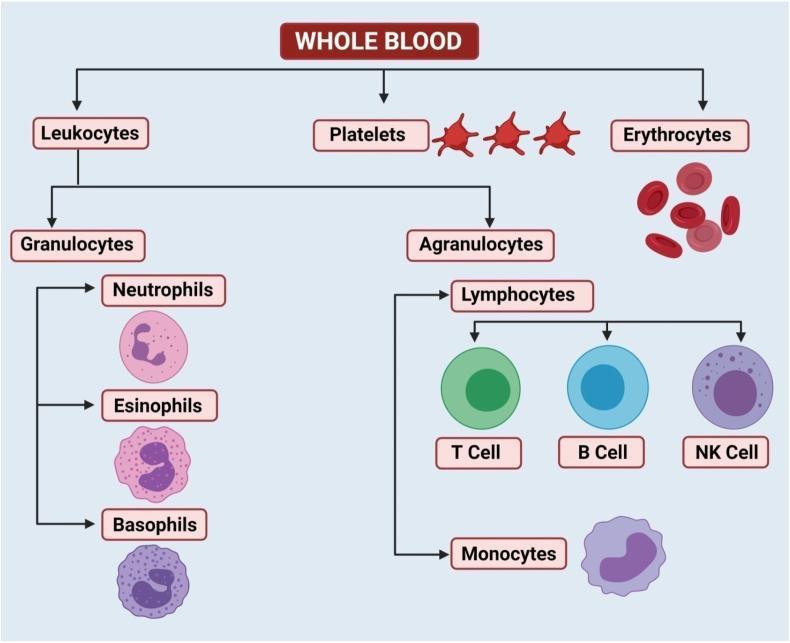
Group 1: Granulocytes
Contain two types of granules: azurophilic granules (lysosomes) and specific granules (which bind differently to stains). They all have polymorphic (multi-lobed) nuclei and are terminally differentiated cells with a short lifespan.
1. Neutrophils
| Feature | Detail |
|---|---|
| Nucleus | 3–5 lobes |
| Granules | Faint/light pink |
| Differential count | 50–70% (most abundant WBC) |
| Lifespan | 1–4 days in tissues |
| Function | Kill and phagocytose bacteria — first responders to infection |
2. Eosinophils
| Feature | Detail |
|---|---|
| Nucleus | Bilobed |
| Granules | Red/dark pink (large, prominent) |
| Differential count | 1–4% |
| Lifespan | 1–2 weeks |
| Function | Kill helminthic (worm) and other parasites; modulate local inflammation; involved in allergic reactions |
3. Basophils
| Feature | Detail |
|---|---|
| Nucleus | Bilobed or S-shaped |
| Granules | Dark blue/purple (obscure the nucleus) |
| Differential count | 0.5–1% (rarest granulocyte) |
| Lifespan | 1–3 days |
| Function | Modulate inflammation; release histamine during allergic responses |
Group 2: Agranulocytes
Contain no specific granules (only scattered azurophilic granules/lysosomes). Nuclei are spherical or indented, but not lobulated.
4. Lymphocytes
| Feature | Detail |
|---|---|
| Nucleus | Spherical, large, densely stained |
| Differential count | 20–40% |
| Lifespan | Hours to many years |
| Function | Effector and regulatory cells of adaptive immunity |
| Subtypes | T cells (cell-mediated immunity), B cells (antibody production), NK cells (natural killer cells — innate cytotoxicity) |
5. Monocytes
| Feature | Detail |
|---|---|
| Nucleus | Indented or C/kidney-shaped |
| Size | Largest WBC |
| Differential count | 2–8% |
| Lifespan | Hours to years |
| Function | Circulate in blood and enter tissues → differentiate into macrophages and other mononuclear phagocytic cells |
Key Concept: Diapedesis
All leukocytes can leave blood vessels at sites of infection/injury through a process called diapedesis — squeezing through endothelial cell junctions into surrounding tissue, guided by cytokines (e.g., IL-1, TNF-α) and chemotaxis.
Quick Summary Table
| WBC Type | Group | % in Blood | Key Function |
|---|---|---|---|
| Neutrophil | Granulocyte | 50–70% | Bacterial phagocytosis |
| Eosinophil | Granulocyte | 1–4% | Anti-parasitic; allergy |
| Basophil | Granulocyte | 0.5–1% | Histamine release; allergy |
| Lymphocyte | Agranulocyte | 20–40% | Adaptive immunity (T, B, NK cells) |
| Monocyte | Agranulocyte | 2–8% | Precursor to macrophages |
— Junqueira's Basic Histology, 17e; Histology: A Text and Atlas with Correlated Cell and Molecular Biology
WBCs and it's function and it's types physiology
Reading File
Finding Sources
Finding Sources
Searching Images
WBC leukocyte physiology function immunity
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
leukocyte types neutrophil lymphocyte monocyte eosinophil basophil blood smear histology
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Now I have rich content from Guyton & Hall and Ganong's. Let me compile the full physiological answer.
White Blood Cells (WBCs / Leukocytes) — Physiology, Types & Functions
WBCs are the mobile units of the body's protective system. They are formed in the bone marrow (granulocytes, monocytes, some lymphocytes) and lymphoid tissue (lymphocytes, plasma cells), then transported in blood to wherever they are needed. Their real value is that most are specifically transported to areas of infection and inflammation, providing rapid and potent defense.
Normal count: 4,000–11,000 WBCs/µL of blood in adults.
Genesis of WBCs (Leukopoiesis)
Two major lineages arise from the multipotential hematopoietic stem cell:
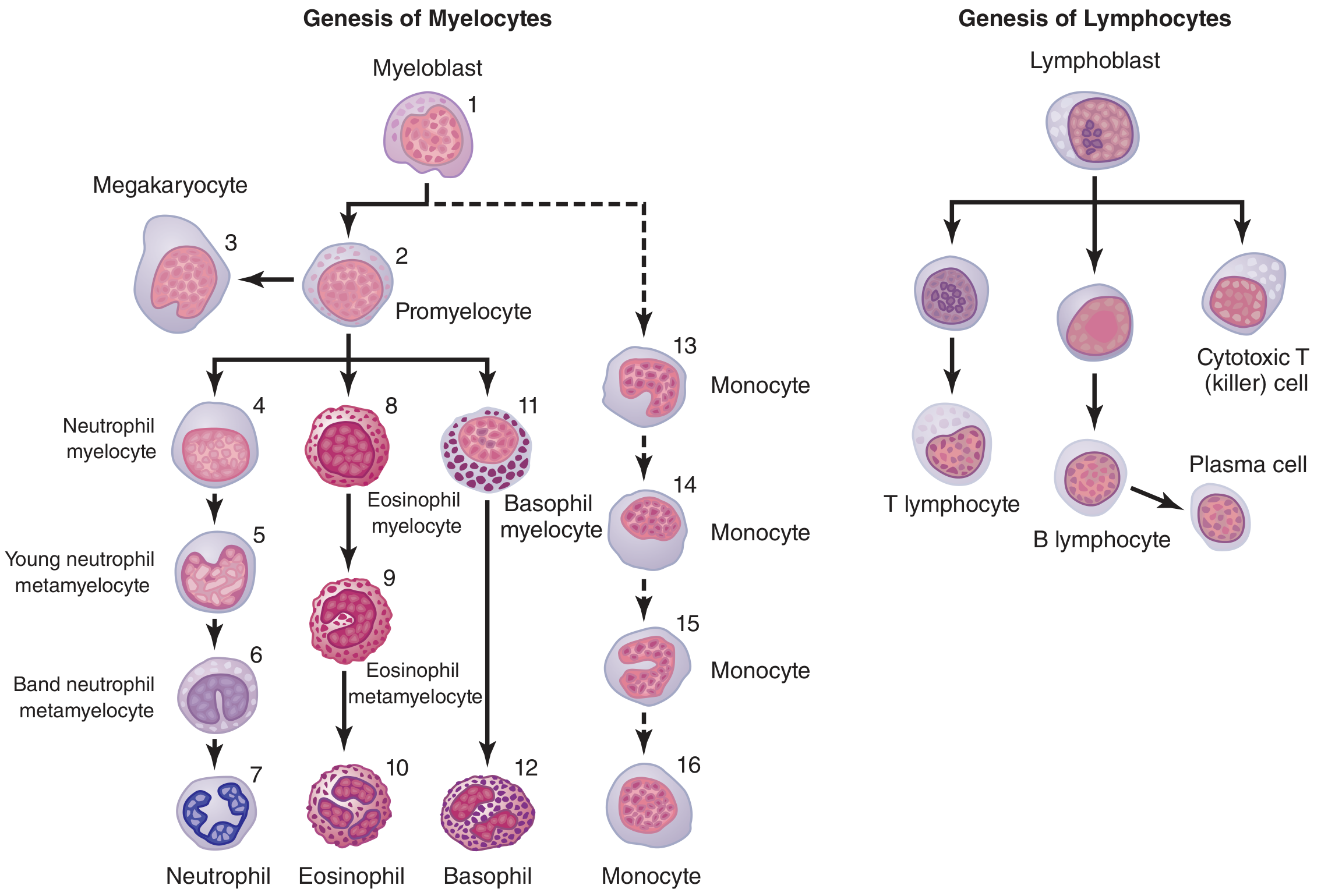
| Lineage | Precursor | Cells Produced |
|---|---|---|
| Myelocytic | Myeloblast → Promyelocyte | Neutrophils, Eosinophils, Basophils, Monocytes |
| Lymphocytic | Lymphoblast | T lymphocytes, B lymphocytes → Plasma cells, NK cells |
Classification & Normal Differential Count
| WBC Type | % in Blood | Absolute Count/µL |
|---|---|---|
| Neutrophils | 50–70% | 3,000–6,000 |
| Lymphocytes | 20–40% | 1,500–4,000 |
| Monocytes | 2–8% | 300–600 |
| Eosinophils | 1–4% | 150–300 |
| Basophils | 0.4% | 0–100 |
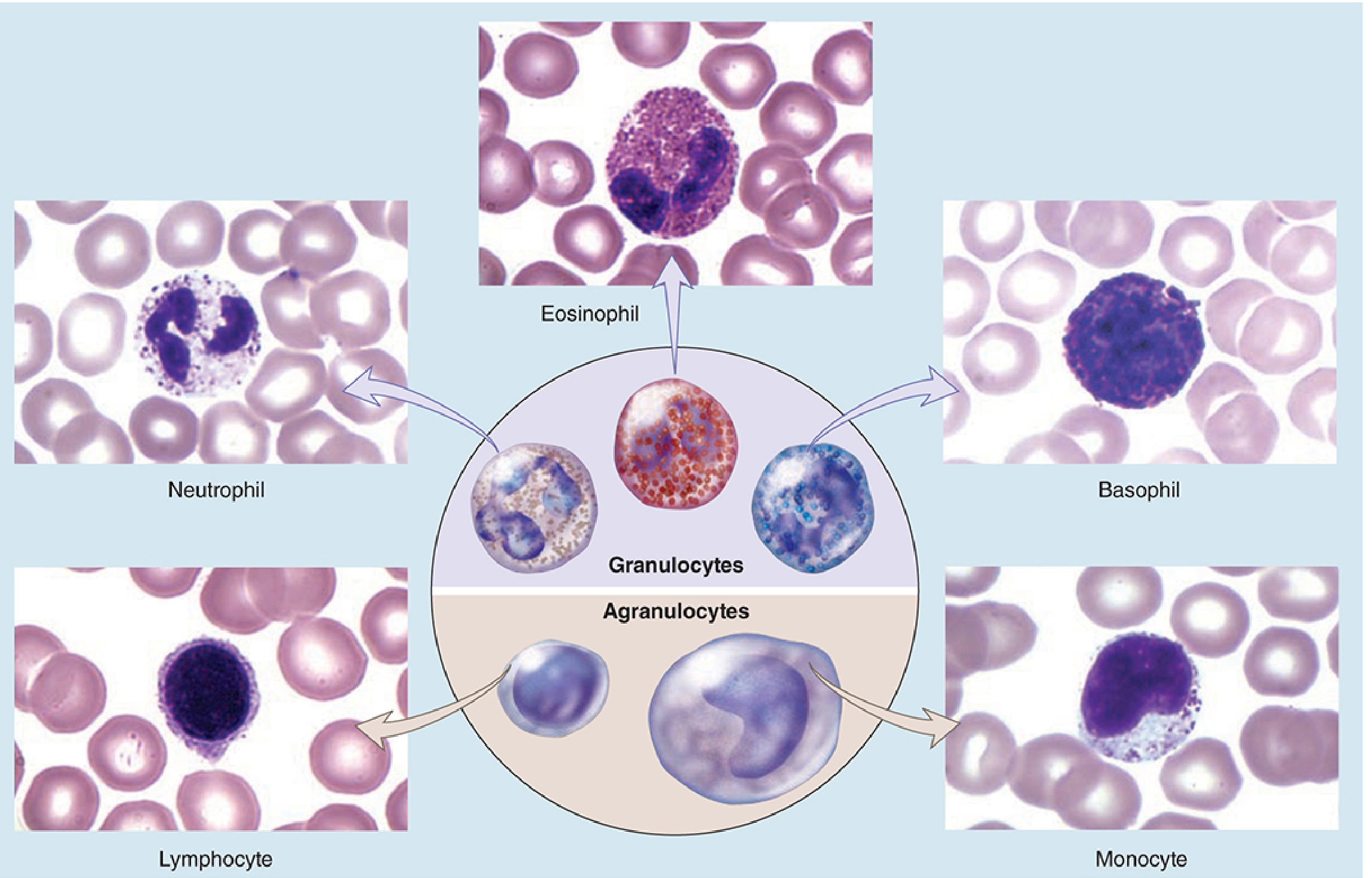
Group 1: Granulocytes (Polymorphonuclear Leukocytes / PMNs)
Contain prominent cytoplasmic granules (lysosomes + specific granules) and multi-lobed nuclei. All are terminally differentiated and short-lived.
1. 🔵 Neutrophils (62%)
Morphology: 3–5 lobed nucleus; faint/light pink granules; 10–12 µm diameter.
Physiology & Functions:
- First responders to bacterial infection — arrive at infection sites within minutes
- Perform phagocytosis: engulf and digest bacteria, fungi, debris
- Move by ameboid motion at up to 40 µm/min through tissue
- Exit blood vessels by diapedesis (extravasation) — squeezing through endothelial gaps
- Are guided to infection sites by chemotaxis — respond to chemical signals up to 100 µm away (bacterial toxins, complement fragments, tissue breakdown products)
- Contain myeloperoxidase, lactoferrin, defensins, and elastase in granules for killing pathogens
- Release neutrophil extracellular traps (NETs) — chromatin webs that trap/kill bacteria
- Lifespan: Only 1–4 days in tissues; billions die by apoptosis daily
2. 🔴 Eosinophils (2.3%)
Morphology: Bilobed nucleus; large, bright red/pink granules (contain major basic protein, eosinophil cationic protein).
Physiology & Functions:
- Primary defense against helminthic (worm) parasites — release toxic granule contents onto parasite surfaces
- Important in allergic reactions and asthma — migrate to sites of IgE-mediated reactions
- Modulate inflammation — produce prostaglandins, leukotrienes, cytokines
- Phagocytose antigen-antibody complexes
- Lifespan: 1–2 weeks in tissues
3. 🟣 Basophils (0.4%)
Morphology: Bilobed or S-shaped nucleus (often obscured by granules); large dark blue/purple granules.
Physiology & Functions:
- Release histamine → vasodilation and increased vascular permeability during allergic reactions
- Release heparin → prevents blood clotting locally and helps transport fat particles
- Release serotonin, leukotrienes (slow-reacting substances of anaphylaxis) → bronchoconstriction
- Bear IgE receptors on their surface → activated in Type I hypersensitivity (anaphylaxis, asthma)
- Functionally similar to mast cells in connective tissue
- Lifespan: 1–3 days
Group 2: Agranulocytes
No specific granules; only scattered azurophilic granules (lysosomes). Nuclei spherical or indented, not lobulated.
4. 🟤 Lymphocytes (30%)
Morphology: Large round nucleus; scant cytoplasm; 6–15 µm diameter.
Physiology & Functions:
The main cells of adaptive (specific) immunity. Three major subtypes:
| Subtype | Origin/Maturation | Key Functions |
|---|---|---|
| T cells | Thymus | Cell-mediated immunity; cytotoxic T cells kill infected/cancer cells; helper T cells regulate immune responses via cytokines |
| B cells | Bone marrow | Humoral immunity; differentiate into plasma cells that secrete antibodies (immunoglobulins) |
| NK cells | Bone marrow | Innate cytotoxicity — kill virus-infected and tumor cells without prior sensitization |
- Memory cells formed after first exposure → faster response on re-exposure (basis of vaccination)
- Lifespan: Hours to many years (memory cells survive decades)
5. 🟠 Monocytes (5.3%)
Morphology: Largest WBC (12–20 µm); kidney-shaped or C-shaped nucleus; abundant agranular cytoplasm.
Physiology & Functions:
- Circulate in blood for 10–20 hours, then enter tissues and differentiate into macrophages (diameter increases 5-fold to 60–80 µm)
- Macrophages are extremely potent phagocytes — the tissue-based second line of defense
Tissue-specific macrophage types:
| Location | Name | Function |
|---|---|---|
| Skin/connective tissue | Histiocytes | Local infection defense |
| Lymph nodes | Lymph node macrophages | Filter and destroy particles in lymph |
| Lungs | Alveolar macrophages | Phagocytose inhaled particles |
| Liver | Kupffer cells | Filter bacteria from portal blood (phagocytose a bacterium in <0.01 sec) |
| Brain | Microglia | CNS immune surveillance |
| Spleen/bone marrow | Splenic macrophages | Remove old RBCs and systemic pathogens |
Key Physiological Mechanisms
Diapedesis & Chemotaxis
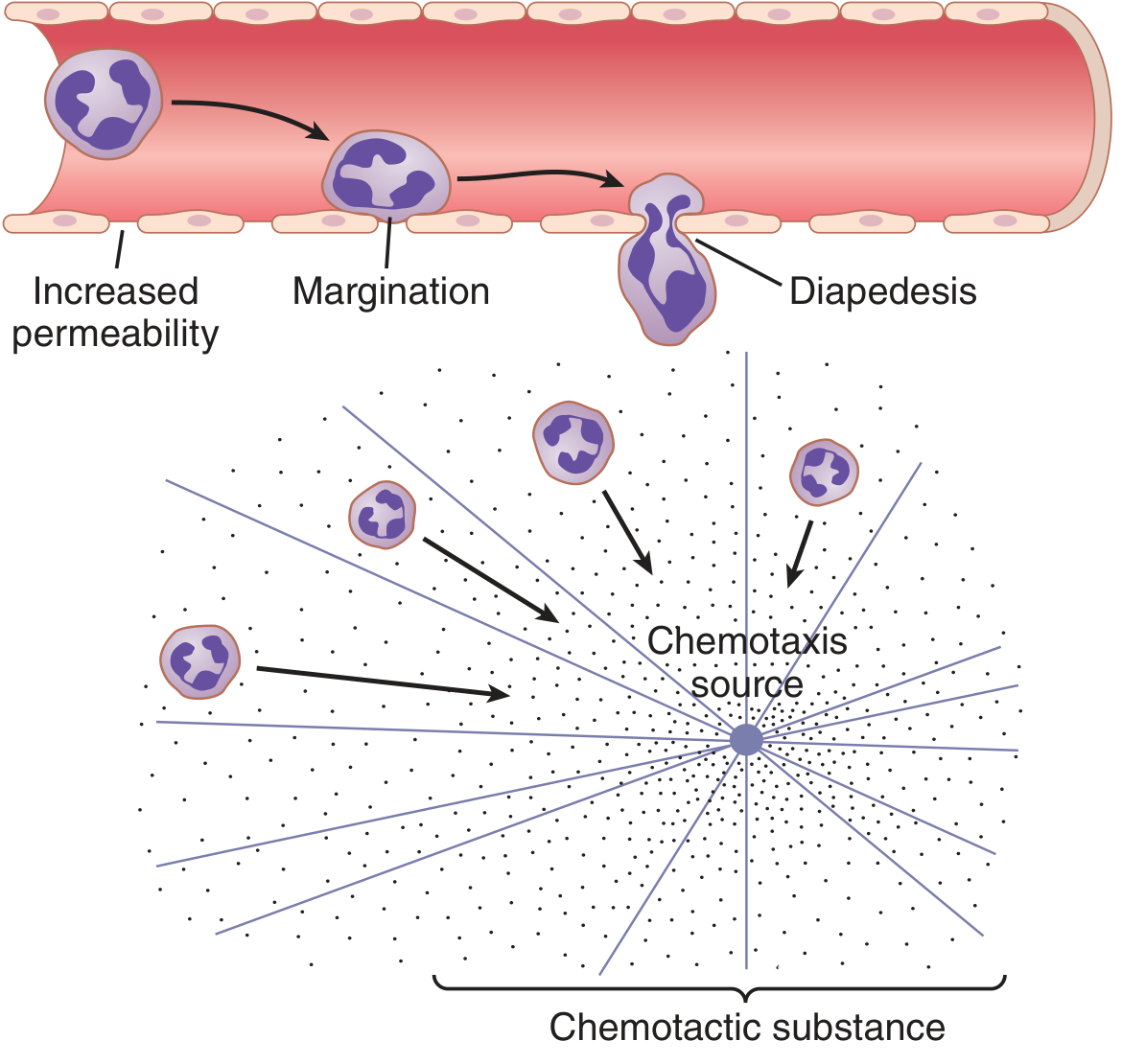
- Margination — WBCs adhere to vessel endothelium near infection site (P-selectin/ligand interactions)
- Diapedesis — WBCs squeeze through endothelial gaps into tissue
- Chemotaxis — WBCs migrate toward infection guided by chemical gradients (bacterial toxins, complement products, cytokines like IL-1, TNF-α)
- Phagocytosis — engulf and destroy pathogens using reactive oxygen species, enzymes, and antimicrobial proteins
- Opsonization — antibodies (IgG) and complement (C3b) coat bacteria, making them easier to phagocytose
Lifespan of WBCs
| WBC | Blood Lifespan | Tissue Lifespan |
|---|---|---|
| Neutrophils | 6–8 hours | 1–4 days |
| Monocytes | 10–20 hours | Months–years (as macrophages) |
| Eosinophils | ~5 hours | 1–2 weeks |
| Basophils | Hours | 1–3 days |
| Lymphocytes | Hours | Hours–decades |
Clinical Significance
| Condition | WBC Change | Cause |
|---|---|---|
| Leukocytosis | Total WBC >11,000/µL | Infection, inflammation, stress |
| Leukopenia | Total WBC <4,000/µL | Bone marrow suppression, viral infection |
| Neutrophilia | ↑ Neutrophils | Bacterial infection, steroids |
| Eosinophilia | ↑ Eosinophils | Parasitic infection, allergy, asthma |
| Lymphocytosis | ↑ Lymphocytes | Viral infection (EBV, CMV) |
| Monocytosis | ↑ Monocytes | Chronic infection (TB), inflammatory disorders |
— Guyton and Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology, 26th Ed; Junqueira's Basic Histology, 17th Ed
What is thymus and it's function it's role in immunity
Reading File
Finding Sources
Searching Images
thymus anatomy histology cortex medulla T cell maturation
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Explain Mechanism Of Pathogenesis
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Excellent - I now have rich content from Robbins Pathologic Basis of Disease. Here is the comprehensive explanation:
Mechanism of Pathogenesis
Pathogenesis is defined as the sequence of molecular, biochemical, and cellular events that lead to the development of disease - in other words, it is the mechanism of disease. It explains how underlying causes (etiology) produce the morphologic and clinical manifestations we observe.
The concept rests on a fundamental principle first stated by Rudolf Virchow, the father of modern pathology:
"Individuals are sick because their cells are sick."
The Four Pillars of Disease (Pathology Framework)
Every disease can be understood through four interconnected concepts:
| Concept | Definition | Example |
|---|---|---|
| Etiology | The initiating cause of disease | Bacterial infection, gene mutation, toxin |
| Pathogenesis | The mechanism/sequence of events leading to disease | How bacteria trigger inflammation → tissue destruction |
| Morphologic Changes | Structural alterations in cells/tissues | Necrosis, fibrosis, tumor formation |
| Clinical Manifestations | Symptoms & signs resulting from the above | Fever, pain, organ dysfunction |
Step 1 — Etiology (The Initiating Cause)
All causes of disease fall into two broad categories:
A. Genetic Causes
- Inherited mutations (e.g., cystic fibrosis gene CFTR)
- Acquired mutations (somatic mutations in cancer)
- Gene variants/polymorphisms that increase susceptibility
B. Environmental Causes
- Infectious agents - bacteria, viruses, parasites, fungi, prions
- Physical agents - radiation, trauma, extreme temperature, electricity
- Chemical agents - drugs, toxins, alcohol, cigarette smoke, pollutants
- Nutritional deficiencies - vitamins, proteins, minerals
- Immunologic factors - autoimmunity, hypersensitivity reactions
Most common diseases (cancer, atherosclerosis, diabetes) are multifactorial - they arise from environmental insults acting on a genetically susceptible individual.
Step 2 — Cellular Response to Stress (The Core Pathogenic Mechanism)
When a cell faces a stressful or injurious stimulus, it goes through a spectrum of responses:
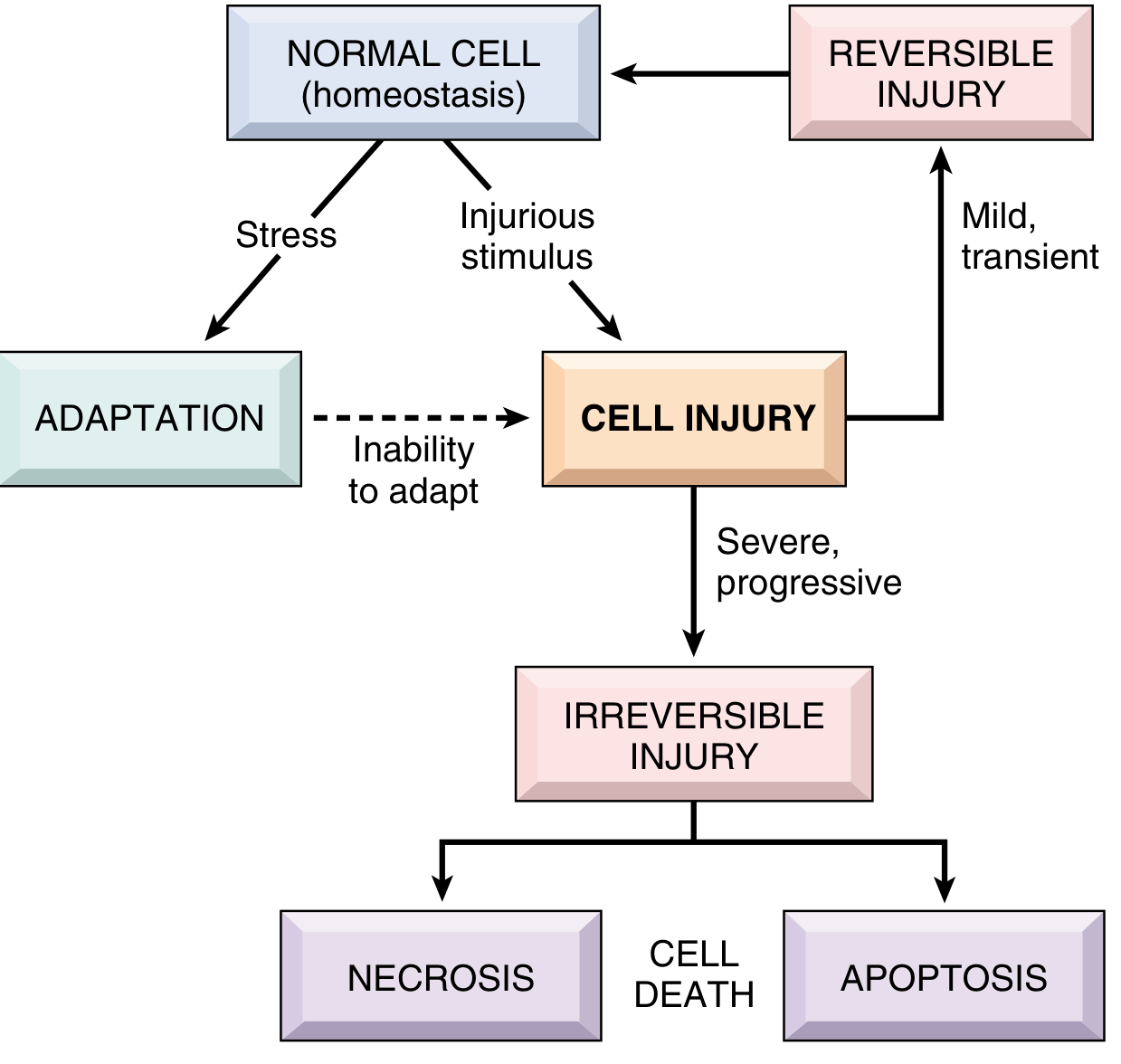
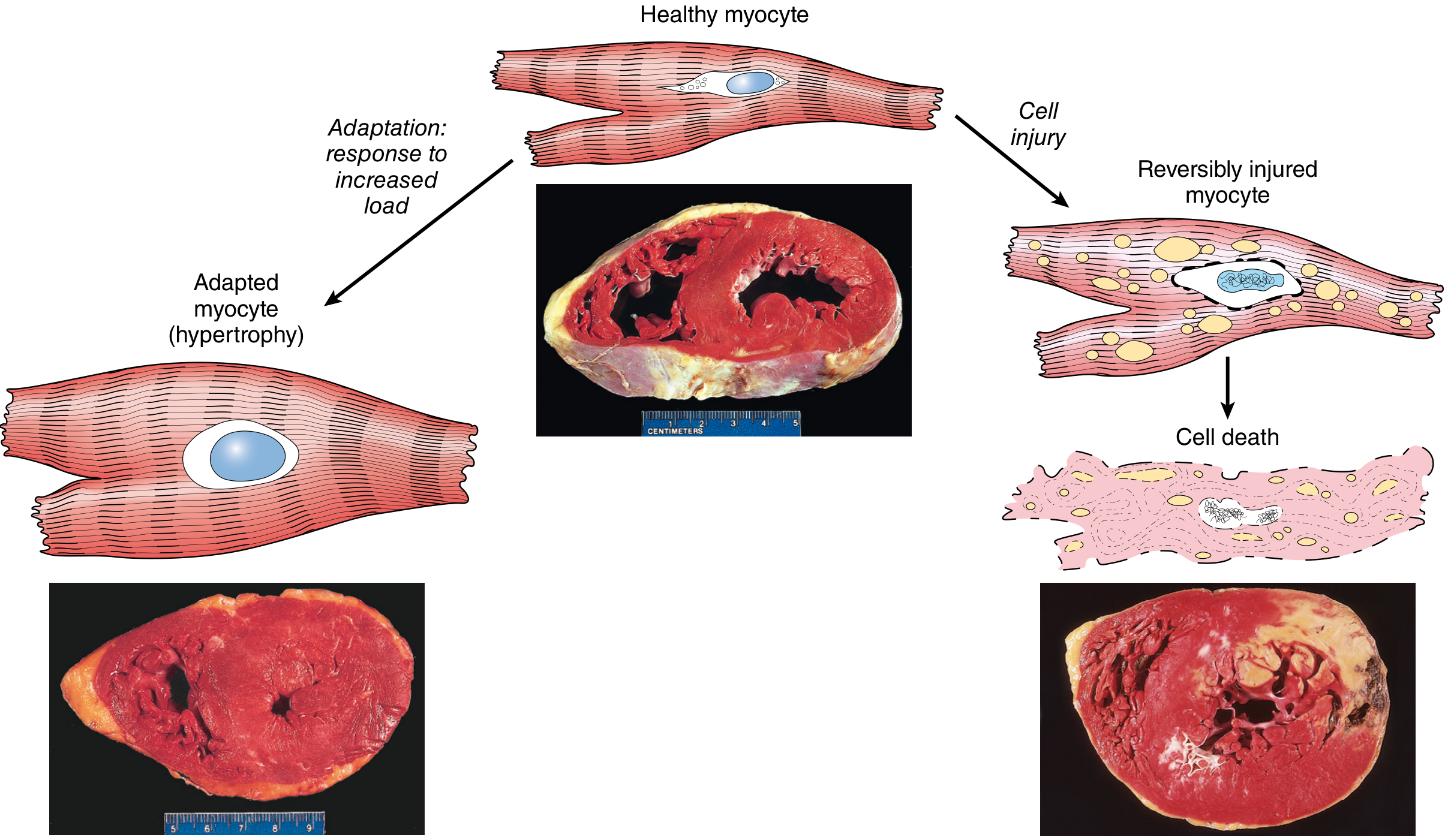
2A. Cellular Adaptation (Reversible - Cell Survives)
When stress is within manageable limits, cells adapt by changing their function or structure. These changes are reversible when the stress is removed.
| Type | Definition | Example |
|---|---|---|
| Hypertrophy | Increase in cell size | Cardiac muscle enlargement in hypertension |
| Hyperplasia | Increase in cell number | Endometrial hyperplasia with excess estrogen |
| Atrophy | Decrease in cell size & metabolic activity | Muscle wasting from disuse |
| Metaplasia | Change in cell type (one mature cell → another) | Columnar → squamous cells in smoker's bronchus (Barrett's esophagus) |
2B. Reversible Cell Injury
If stress exceeds adaptive capacity, injury begins. At this stage, if the stimulus is removed, the cell can recover.
Features of reversible injury:
- Cellular swelling (most common early sign)
- Fatty change (lipid accumulation in cells)
- Plasma membrane blebbing and loss of microvilli
- Mitochondrial swelling
- Dilation of the endoplasmic reticulum
- Clumping of nuclear chromatin
Mechanism: The primary event is usually failure of the sodium-potassium ATPase pump (due to ATP depletion), causing sodium and water to accumulate → cell swelling.
2C. Irreversible Cell Injury → Cell Death
If injury is severe or persistent, the cell crosses a "point of no return" and dies. There are two main pathways:
Step 3 — Two Pathways of Cell Death
🔴 Pathway 1: NECROSIS (Pathological Death)
Necrosis is a pathologic, uncontrolled form of cell death caused by external injury. It always triggers inflammation.
Mechanism:
- Severe injury → membrane disruption
- Intracellular enzymes and proteins leak out into surrounding tissue
- Leaked contents trigger inflammatory response (redness, swelling, pain)
- Macrophages and neutrophils arrive to clean up debris
Morphologic features:
- Eosinophilic (pink) cytoplasm on H&E staining (due to loss of RNA)
- Nuclear changes: pyknosis (shrinkage) → karyorrhexis (fragmentation) → karyolysis (dissolution)
- Breakdown of plasma and organelle membranes
- Myelin figures (whorled phospholipid masses)
Patterns of Necrosis:
| Pattern | Mechanism | Where it Occurs |
|---|---|---|
| Coagulative | Protein denaturation preserves cell architecture | Heart, kidney (infarction) |
| Liquefactive | Enzymatic digestion of dead cells | Brain, abscess (bacterial infections) |
| Caseous | Combination of coagulative + liquefactive; cheesy appearance | Tuberculosis (granulomas) |
| Fat necrosis | Lipases digest adipose tissue | Pancreas (acute pancreatitis) |
| Gangrenous | Coagulative necrosis + superimposed bacterial infection | Limbs with ischemia + infection |
| Fibrinoid | Antigen-antibody complexes + fibrin deposited in vessel walls | Vasculitis, malignant hypertension |
🟢 Pathway 2: APOPTOSIS (Programmed Death)
Apoptosis is a regulated, controlled self-destruct program. It does not trigger inflammation and is essential for normal physiology.
Mechanism:
- Cell receives a "death signal" (intrinsic or extrinsic pathway)
- Caspase enzymes are activated (the executioner proteins)
- DNA is fragmented by DNAses into a characteristic "ladder" pattern
- Cell shrinks and breaks into apoptotic bodies (membrane-bound fragments)
- Phagocytes recognize "eat me" signals (phosphatidylserine exposure) and engulf them
- No inflammatory response - clean, silent death
When apoptosis occurs physiologically:
- Development (sculpting of fingers, removal of excess neurons)
- Hormone-driven involution (uterine lining during menstruation)
- Elimination of self-reactive lymphocytes (immune tolerance)
- Removal of aged/damaged cells (neutrophils after acute infection resolves)
When apoptosis occurs pathologically:
- Virus-infected cells
- DNA-damaged cells (tumor suppressor p53 activates apoptosis)
- Ischemic injury (e.g., brain after stroke)
Step 4 — Downstream Pathogenic Mechanisms
Once cells are injured or dead, multiple downstream processes perpetuate disease:
🔥 Inflammation
- Necrotic cells release damage-associated molecular patterns (DAMPs)
- Macrophages release cytokines (IL-1, TNF-α, IL-6)
- Neutrophils are recruited → acute inflammation
- If unresolved → chronic inflammation → fibrosis (scarring)
- Chronic inflammation is the pathogenic basis of atherosclerosis, rheumatoid arthritis, IBD, and many cancers
🧬 Genetic/Molecular Dysregulation
- Mutations in proto-oncogenes → oncogenes → uncontrolled cell proliferation → cancer
- Loss of tumor suppressor genes (p53, Rb) → failure of cell cycle control
- Epigenetic changes → gene silencing or overexpression
🛡️ Immune-Mediated Injury
- Type I hypersensitivity (IgE/mast cells): Anaphylaxis, asthma
- Type II (antibody-mediated): Autoimmune hemolytic anemia
- Type III (immune complex): SLE, serum sickness
- Type IV (T cell-mediated): Contact dermatitis, graft rejection, tuberculosis
🧪 Accumulations & Deposits
- Lipid accumulation → fatty liver → cirrhosis
- Abnormal protein folding → amyloidosis
- Calcium deposition → dystrophic calcification
- Glycogen/lipid storage in lysosomal storage disorders
Summary Flowchart
ETIOLOGY (Cause)
↓
Genetic / Environmental Insult
↓
Cellular Stress
↓ ↙ Mild stress → ADAPTATION (hypertrophy, hyperplasia, atrophy, metaplasia)
↓ ↙ Mild/transient → REVERSIBLE INJURY (swelling, fatty change)
↓ ↙ Severe/sustained → IRREVERSIBLE INJURY
↙ ↘
NECROSIS APOPTOSIS
(uncontrolled, (controlled,
inflammatory) non-inflammatory)
↓
Morphological Changes (tissue damage, fibrosis, organ dysfunction)
↓
CLINICAL MANIFESTATIONS (symptoms, signs, disease)
- Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.