take Cummings only as reference and summarize surgical management of OSA
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the key content I need to write a comprehensive summary. Let me compile the full surgical management section from Cummings.
Surgical Management of Obstructive Sleep Apnea
(Cummings Otolaryngology Head and Neck Surgery, Chapter 15)
Indications for Surgery (Box 15.6)
Surgery is considered when:
- AHI >5 and <14 with symptoms or comorbidities
- AHI >15
- Oxyhemoglobin desaturation <90%
- Upper airway resistance syndrome (with objective neurocognitive impairment unresponsive to medical therapy)
- Significant cardiac arrhythmias associated with obstruction
- Unsuccessful or refused medical therapy with patient desire for surgery
- Patient medically stable enough to undergo the recommended procedure
Preoperative Principles
- A staged, stepwise surgical protocol is used. The site of obstruction must be identified in every patient before choosing the procedure.
- Drug-Induced Sleep Endoscopy (DISE) is the optimal method to evaluate airway collapse patterns. In one series, DISE altered the surgical plan in 62% of patients, and 73% had multilevel obstruction.
- Endoscopic studies show that ~100% of OSA patients have retropalatal obstruction, and ~77% have retroglossal obstruction - meaning most patients require multilevel surgical treatment.
- Patients with isolated palatal collapse undergo palatal surgery; those with tongue-base obstruction undergo hypopharyngeal procedures.
- Anesthesia planning is mandatory: use oropharyngeal airway, avoid paralyzing agents until mask ventilation is confirmed, and prepare alternative airway methods. Discuss the possibility of tracheotomy with the patient preoperatively.
- Patients must be screened for cardiovascular disease before surgery.
Surgical Treatment Options (Box 15.7)
1. Nasal Surgery
Procedures: Septoplasty, inferior turbinate reduction, nasal valve reconstruction, adenoidectomy, nasal polyp/tumor resection.
- Nasal obstruction is associated with poor sleep quality, snoring, and OSA.
- Nasal surgery alone is unlikely to significantly improve AHI but restores physiologic nasal breathing and, critically, improves CPAP adherence in patients who previously could not tolerate nasal CPAP.
- Nasal surgery should be considered as an initial step in OSA management primarily to facilitate CPAP use.
2. Palatal Surgery
Uvulopalatopharyngoplasty (UPPP)
- First described by Fujita et al. in 1981 - the most commonly performed surgical procedure for OSA.
- Involves resection of redundant palatal and pharyngeal tissue along with tonsillectomy.
- When used indiscriminately regardless of obesity, retrognathia, or multilevel obstruction, it is often unsuccessful.
- Success rate is markedly dependent on the site of collapse: meta-analyses show success rates of ~52-80% in properly selected patients with isolated palatal obstruction, but much lower in unselected cohorts.
- In patients with non-palatal (lateral wall) collapse patterns identified on DISE, outcomes are worse.
Z-Palatoplasty
- A modification of UPPP that directs the pull on the soft palate in an anterolateral direction, widening the retropalatal space (see Fig. 15.15).
- Designed to address lateral pharyngeal wall collapse in addition to palatal collapse.
Expansion Sphincter Pharyngoplasty (ESP)
- Specifically targets lateral pharyngeal wall collapse (circumferential or lateral pattern on DISE).
- The palatopharyngeus muscle is repositioned laterally and superiorly to expand the velopharyngeal inlet.
Transpalatal Advancement Pharyngoplasty
- Used for select patients, particularly where UPPP is insufficient.
Palatal Radiofrequency Ablation, Pillar Implants, Injection Snoreplasty
- Less invasive options primarily for snoring and mild OSA; generally not sufficient as standalone treatments for moderate-to-severe OSA.
3. Hypopharyngeal / Tongue-Base Surgery
Lingual Tonsillectomy
- Addressed when lingual tonsillar hypertrophy contributes to tongue-base obstruction.
Partial Midline Glossectomy
- Reduces tongue-base volume to improve the retrolingual airway.
Tongue-Base Radiofrequency Ablation
- Delivers radiofrequency energy to the base of tongue to reduce tissue volume via submucosal scarring and contraction.
- Can be performed in staged sessions; generally reserved for mild-to-moderate disease or as adjunct treatment.
Tongue-Suspension Suture
- A suture is passed through the base of tongue and anchored to the mandible to prevent posterior tongue displacement during sleep.
Genioglossus Advancement (Mandibular Osteotomy + Genioglossal Advancement)
- A rectangular osteotomy of the anterior mandible is performed at the geniotubercle to advance the genioglossus muscle attachment anteriorly.
- This tensions the genioglossus, reducing tongue-base obstruction.
- Often combined with UPPP as part of the Riley-Powell-Stanford Phase I protocol.
Hyoid Myotomy and Suspension
- The hyoid bone is released from its attachments (myotomy) and suspended anteriorly to the mandible or thyroid cartilage.
- Expands the hypopharyngeal airway by pulling the tongue base and epiglottis anteriorly.
- Typically combined with other procedures rather than performed alone.
Maxillomandibular Advancement (MMA)
- The most anatomically effective surgical procedure for OSA.
- Both the maxilla and mandible are advanced using Le Fort I osteotomy + bilateral sagittal split ramus osteotomy, typically by 10 mm or more.
- Advancement expands the entire upper airway (retropalatal + retrolingual) by pulling all attached pharyngeal soft tissues anteriorly.
- Meta-analyses show surgical success rates of ~86% and cure rates of ~43%, making it the most effective single surgical procedure.
- Reserved for patients who fail Phase I surgery or those with significant dentofacial/skeletal abnormalities.
- Requires orthognathic planning and carries risks of facial numbness, malocclusion, and prolonged recovery.
4. Hypoglossal Nerve Stimulation (Upper Airway Stimulation)
- Implantable device (e.g., Inspire system - STAR trial) that senses inspiratory effort via a chest wall pressure sensor and delivers timed electrical stimulation to the hypoglossal nerve, increasing genioglossus tone during each inspiration.
- STAR trial (2014): Multicenter prospective trial; demonstrated significant reduction in AHI and improvement in oxygen desaturation index with sustained benefit at 12 months.
- Patient selection criteria: BMI <32 kg/m², AHI 25-65 (moderate-to-severe but not morbidly elevated), non-concentric collapse on DISE (i.e., no complete circumferential velum collapse). AHI ≤50 + BMI ≤32 kg/m² predicts best outcomes.
- In the Van de Heyning series, the success rate was 55% in appropriately selected patients vs. 0% in those who did not meet criteria.
- Advantage: minimally invasive, avoids oropharyngeal scarring, adjustable, reversible.
5. Tracheotomy
- Described at line 1578 of block 4 as a definitive treatment option.
- Bypasses the entire upper airway obstruction and is effectively 100% curative for OSA from upper airway collapse.
- Reserved for patients with severe, life-threatening OSA who have failed all other treatments, or those with complex craniofacial anomalies.
- Carries significant quality-of-life and social concerns.
- Should be discussed with patients preoperatively as a possibility in any airway surgery.
Postoperative Care
- Hospitalization is recommended for most patients after airway surgery.
- ICU admission should be considered for multilevel surgery.
- Nasal CPAP is recommended for the first 2 weeks postoperatively (especially in severe OSA, where the lowest preoperative SpO2 may be as low as 51.5%).
- Follow-up PSG at 3-4 months is recommended to objectively evaluate surgical response.
Surgical Algorithm Summary
| Phase | Level | Procedure |
|---|---|---|
| Phase I | Nasal | Septoplasty, turbinate reduction (if needed to enable CPAP) |
| Phase I | Palatal | UPPP / Z-palatoplasty / ESP + tonsillectomy |
| Phase I | Tongue base | Genioglossus advancement + hyoid myotomy/suspension |
| Phase II | Skeletal | Maxillomandibular advancement (if Phase I fails) |
| Adjunct | Neurostimulation | Hypoglossal nerve stimulation (selected patients) |
| Rescue | Bypass | Tracheotomy |
The key principle from Cummings is that surgical success depends on correct identification of the obstruction site (using DISE or endoscopy) and tailoring the procedure to the individual patient's anatomy, rather than applying UPPP uniformly to all OSA patients.
- Cummings Otolaryngology Head and Neck Surgery, Chapter 15 (Sleep Apnea and Sleep Disorders), pp. 305-320
GIVE DIAGRAMS FOR A FEW OF THESE SURGERIES TO DRAW IN EXAM
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Now I have all the key Cummings figures. Let me present them organized by surgery with clear exam-focused annotations.
Surgical Diagrams for OSA - from Cummings
1. Modified Mallampati / Friedman Staging - Patient Selection for UPPP
(Fig. 15.13 - Cummings)
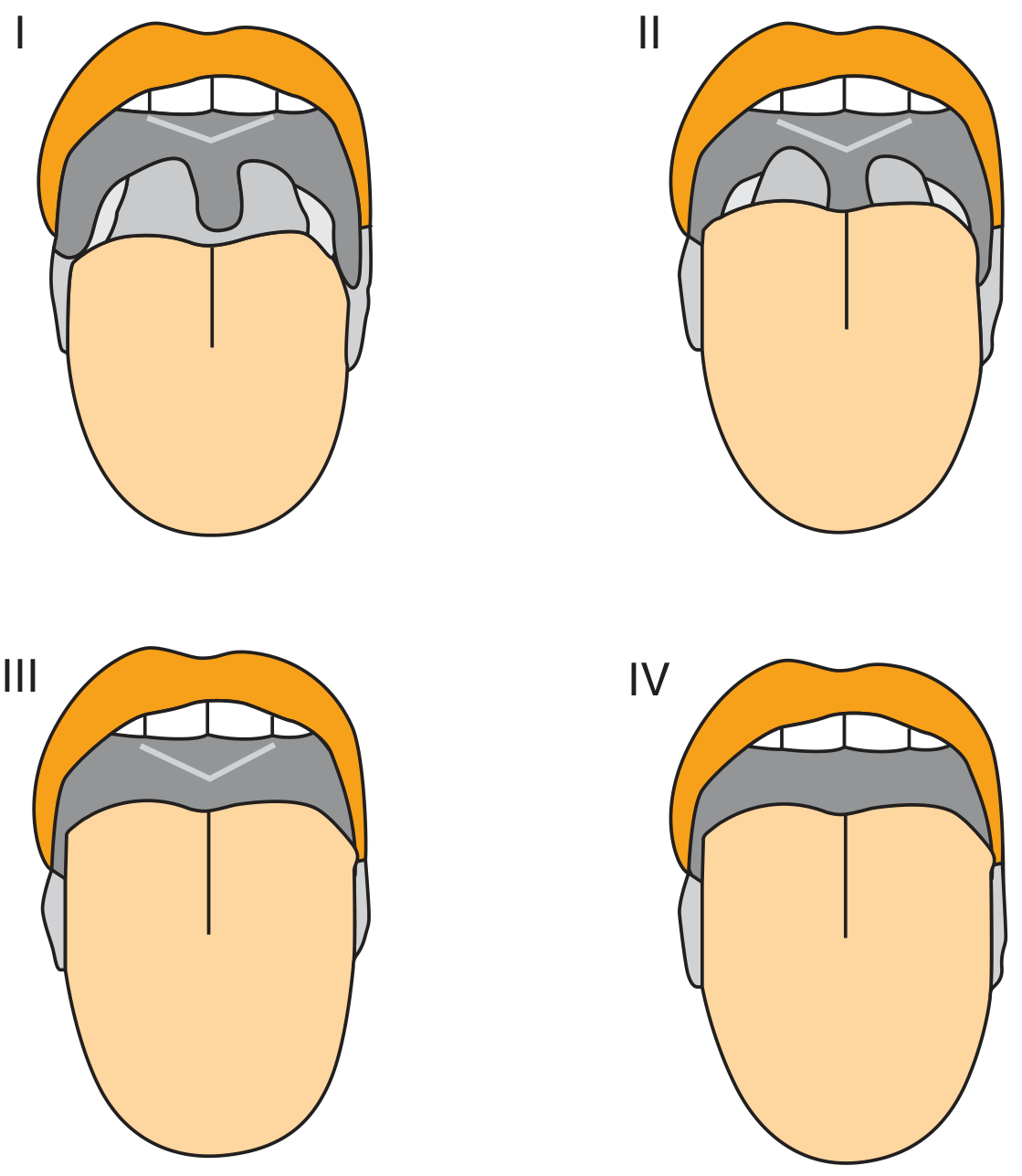
How to draw this in exams:
Draw 4 open-mouth views showing the soft palate progressively more obscured by the tongue:
- Grade I - Entire uvula + tonsils visible → UPPP success ~80%
- Grade II - Partial uvula visible → UPPP success ~40%
- Grade III - Only soft + hard palate seen (no uvula) → UPPP success ~8%
- Grade IV - Only hard palate seen
Combined with tonsil size and BMI = Friedman staging for UPPP patient selection
2. Z-Palatoplasty (Soft Palate Anterolateral Repositioning)
(Fig. 15.15 - Cummings)
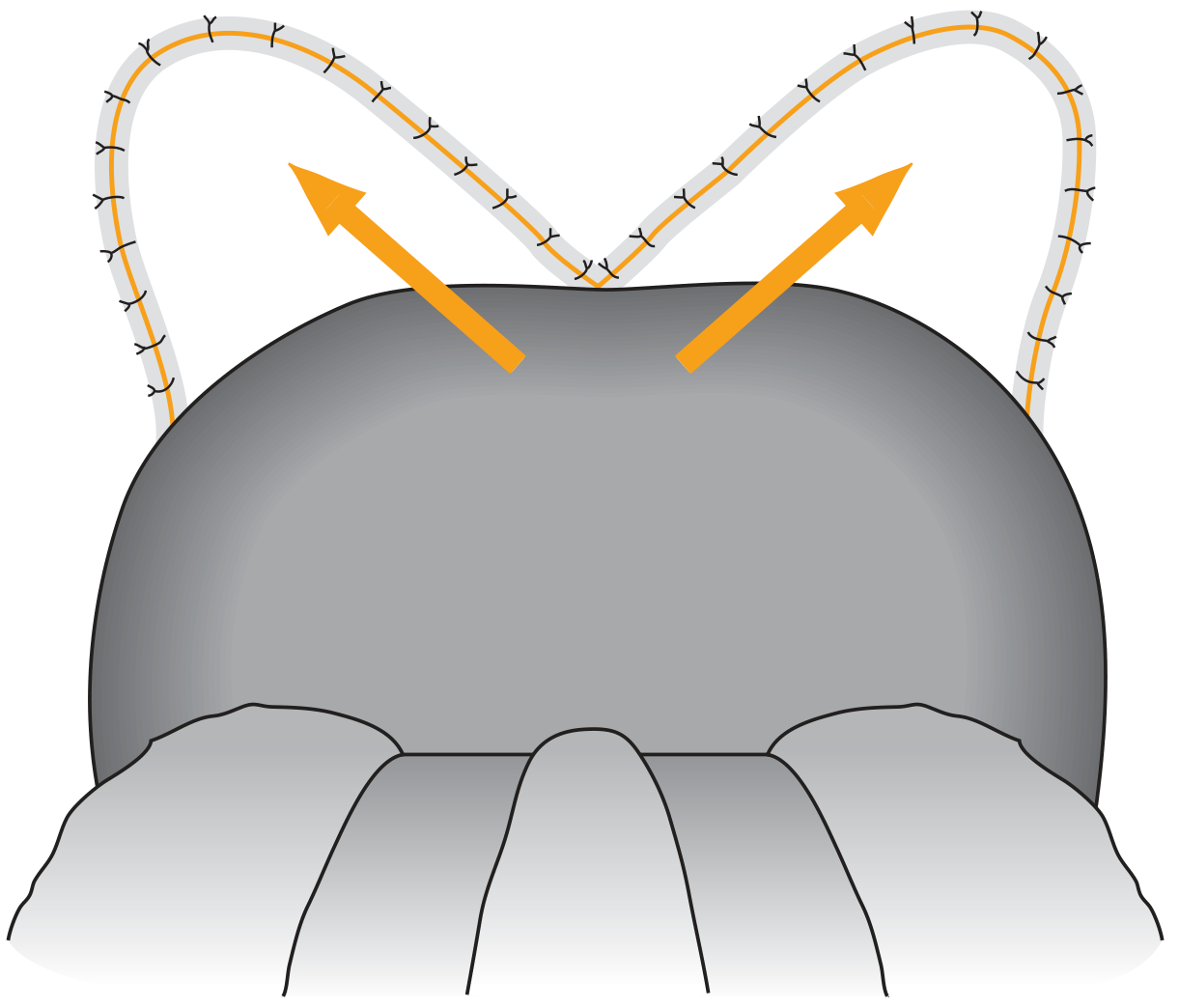
How to draw this in exams:
- Draw soft palate (dome shape, viewed from above/behind)
- Show bilateral incisions on either side forming a Z-pattern
- Draw bilateral suture lines curving anterolaterally (arrows pointing up-and-outward)
- The key point: vectors of pull are anterolateral, not just posterior - this widens the retropalatal space by pulling the soft palate forward and to the sides, not just tightening it posteriorly
- Label: "Widened retropalatal space" in the center
3. Expansion Sphincter Pharyngoplasty (ESP)
(Fig. 15.16 - Cummings)
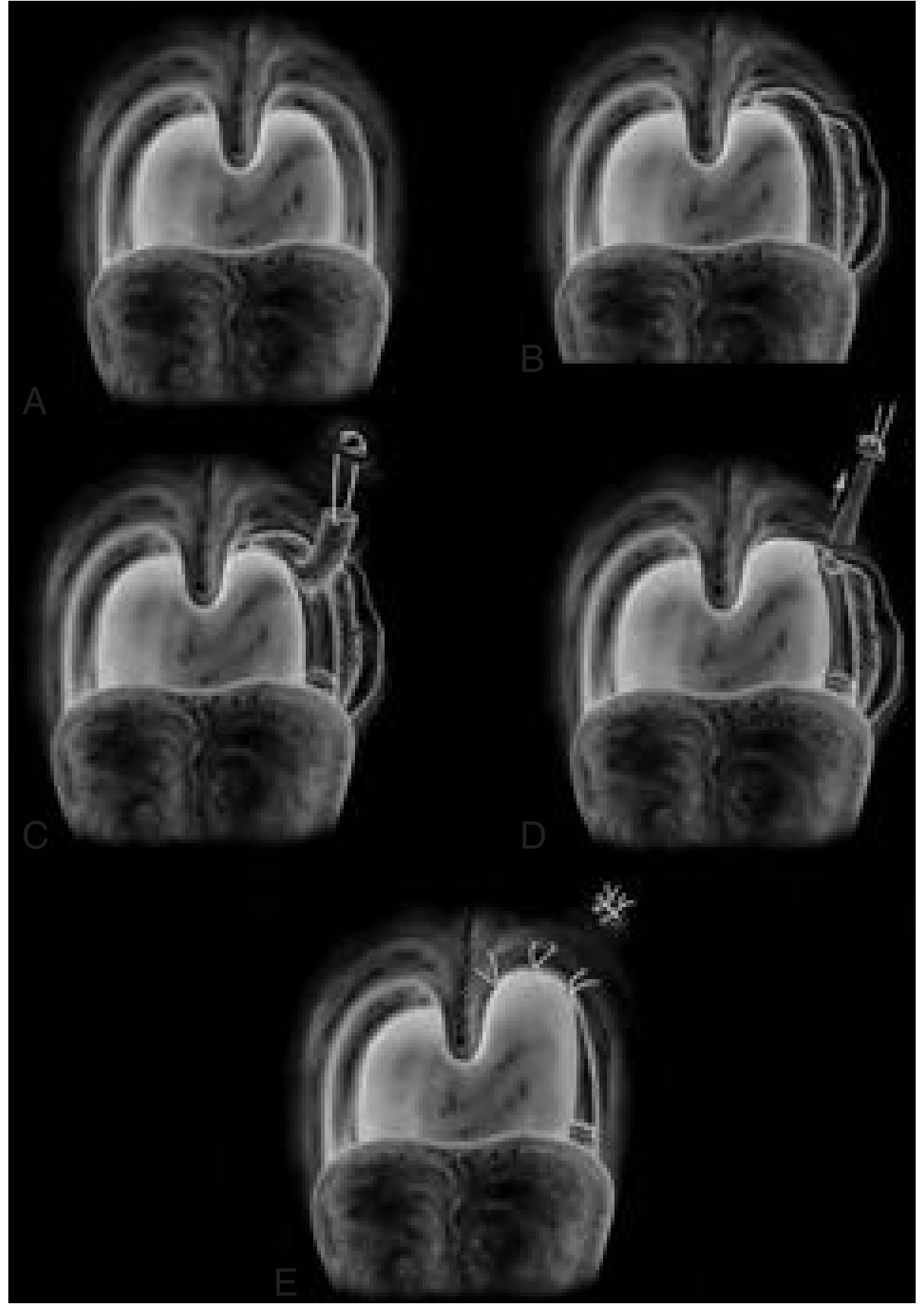
Steps to draw in exams (A→E):
- A - Normal oropharynx with tonsils in fossa
- B - Tonsillectomy done; palatopharyngeus (vertical muscle) exposed
- C - Palatopharyngeus elevated off posterior pillar
- D - Muscle rotated superolaterally toward the hamulus
- E - Suture suspension anchoring the muscle to the hamulus → pharyngeal inlet widened laterally
Key label: "Lateral pharyngeal wall expansion" - specifically targets circumferential/lateral collapse pattern on DISE
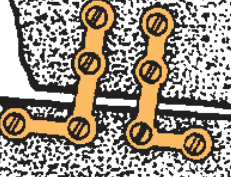
4. Genioglossal Advancement - Rectangular Geniotubercle Osteotomy
(Fig. 15.17 - Cummings)
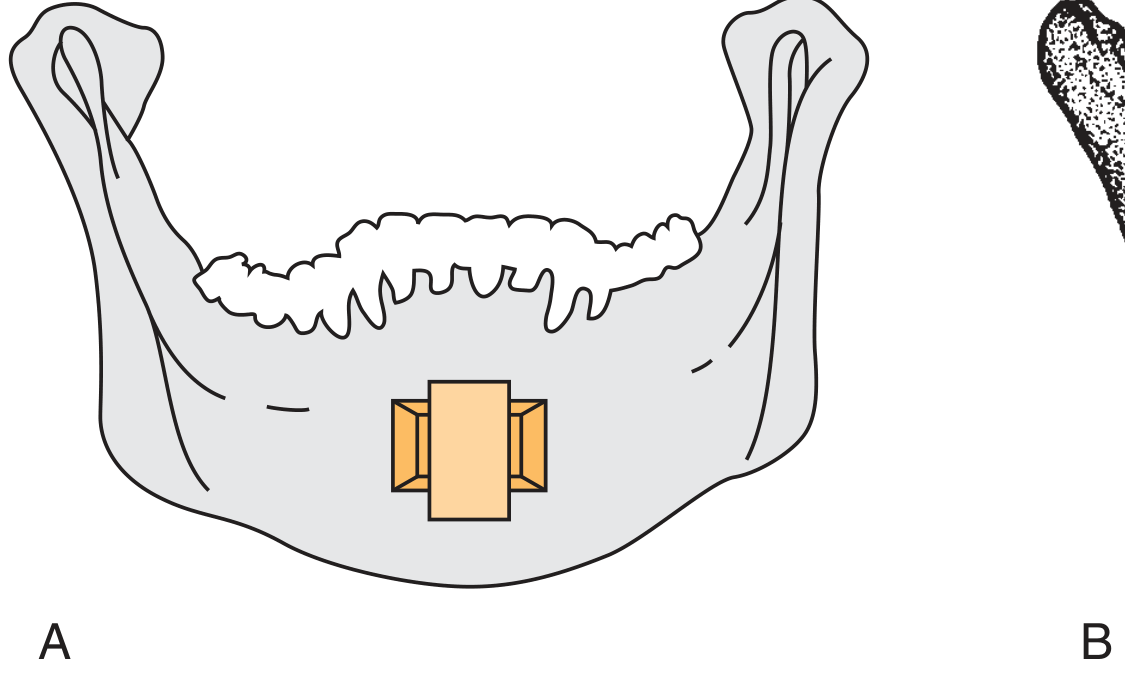
How to draw this in exams:
- Draw the mandible (horseshoe shape, anterior view)
- Mark a rectangular box at the midline symphysis (the geniotubercle)
- Show the fragment being rotated outward (anteriorly) - the fragment is turned 90° to create bony overlap
- Fix with a single inferior miniscrew
- Label: "Genioglossus muscle attachment advanced anteriorly" → tensions the tongue base → prevents posterior displacement during sleep
Draw lateral view too: show tongue being pulled forward by the tensioned muscle
5. Hyoid Myotomy and Suspension
(Fig. 15.18 - Cummings)
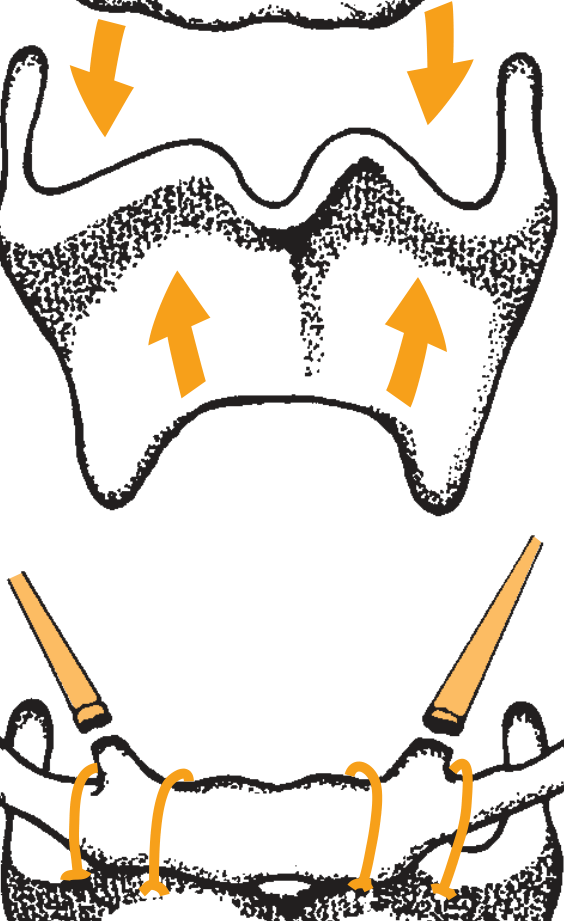
How to draw this in exams (2 parts):
Top diagram (myotomy):
- Draw hyoid bone (U-shaped) with infrahyoid muscles attaching below
- Show downward arrows from mandible onto hyoid (compressing) and upward arrows from thyroid cartilage
- The hyoid is released from its muscular attachments (myotomy) - draw dotted cut lines through the infrahyoid muscles below the hyoid
Bottom diagram (suspension):
- Show hyoid being suspended superiorly with sutures (draw suture loops passing through hyoid body)
- Anchor sutures pass to the inferior mandible (hyoid-to-mandible) or thyroid cartilage (hyoidthyroidopexy)
- Result: entire tongue base and epiglottis pulled anteriorly, expanding the hypopharyngeal airway
6. Maxillomandibular Advancement (MMA)
(Fig. 15.19 - Cummings)
How to draw this in exams (lateral skull view):
- Draw lateral skull profile
- Draw Le Fort I line (horizontal cut through maxilla above the teeth)
- Draw bilateral sagittal split line through the mandibular ramus
- Show both jaws advanced at least 10 mm anteriorly with arrows
- Show rigid plate fixation (miniplates + screws) at both osteotomy sites
- Optional: show previous genioglossal advancement screw at symphysis
- Draw a before/after airway outline: narrow posterior airspace → widened airspace after advancement
- Label: "All attached pharyngeal soft tissues pulled forward en bloc"
Most effective surgical procedure for OSA - success rate ~86%
Quick Reference: Which Diagram to Draw for Which Question
| If asked about... | Draw... |
|---|---|
| Patient selection for UPPP | Friedman/Mallampati staging (4 grades) |
| Palatal surgery for lateral collapse | Z-palatoplasty vectors OR ESP steps A-E |
| Tongue-base / hypopharyngeal surgery | Genioglossal advancement (rectangular osteotomy) |
| Hyoid / epiglottis obstruction | Hyoid myotomy + suspension (2-part diagram) |
| Most effective OSA surgery | MMA lateral view (Le Fort I + BSSO, 10mm advance) |
All figures from Cummings Otolaryngology Head and Neck Surgery, Chapter 15, pp. 313-319
This is a shared conversation. Sign in to Orris to start your own chat.