Cutaneous drugs reaction derma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cutaneous drug reactions"[MeSH Terms] AND "drug hypersensitivity"[MeSH Terms]
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content. Let me compile the full, detailed answer.
Cutaneous Drug Reactions (Adverse Cutaneous Drug Reactions / CARs)
The skin is one of the most common targets for adverse drug reactions. Up to 8% of hospitalized patients experience cutaneous adverse reactions (CARs), which account for ~2% of dermatology consultations and ~5% of inpatient dermatology admissions. Fatalities from drug reactions (systemic + cutaneous) in inpatients range from 0.1%-0.3%.
Pathomechanisms
The central immunologic event in severe cutaneous drug reactions involves a drug-MHC complex that activates CD8+ T cells, which then cause keratinocyte cell death via apoptosis and necroptosis:
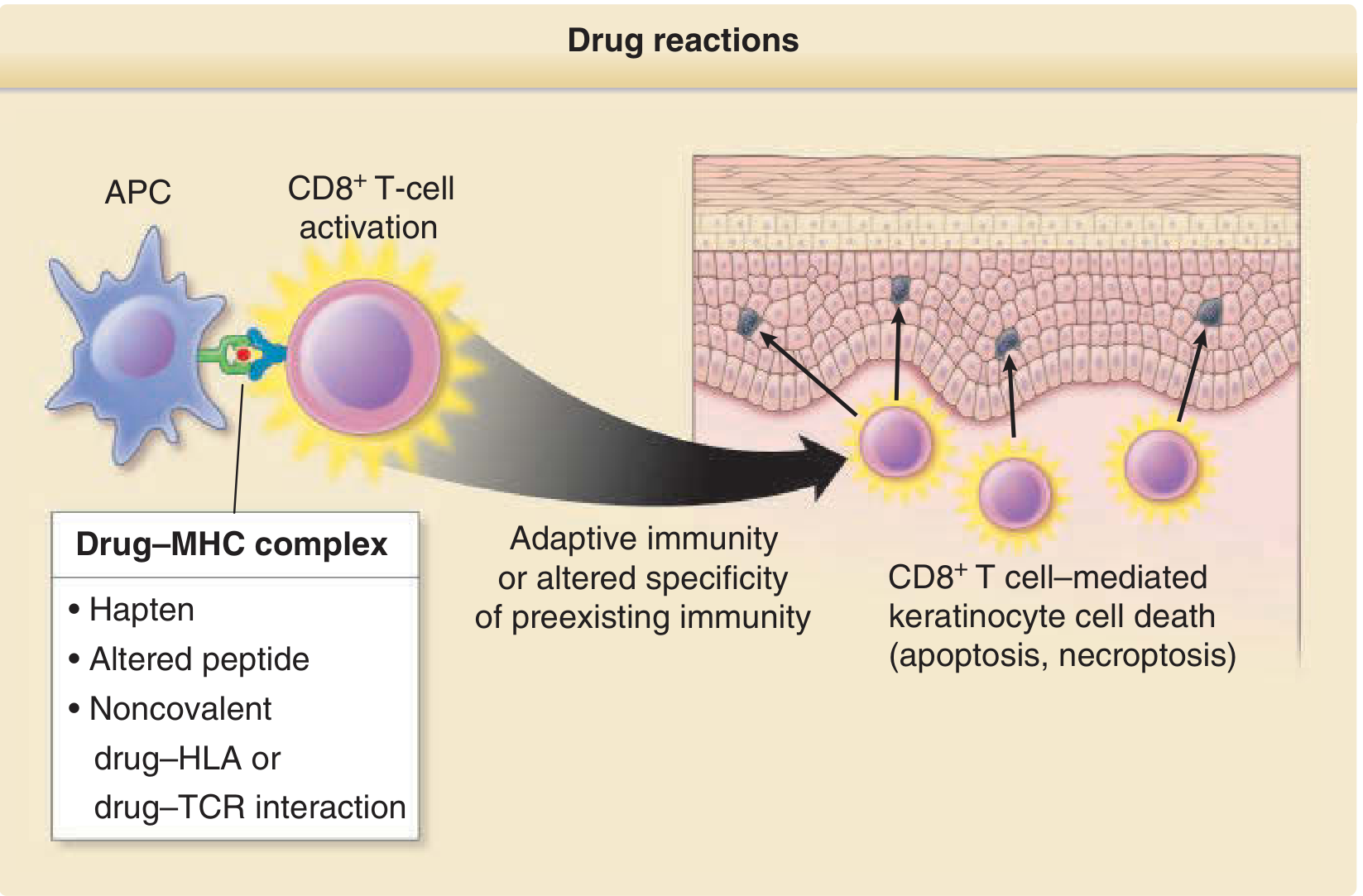
Figure: Canonical or aberrant activation of T cells triggered by a culprit drug results in T cell-mediated keratinocyte cell death in severe drug reactions such as SJS and TEN. (Fitzpatrick's Dermatology)
Three proposed models of T-cell activation:
- Hapten model - drug acts as a hapten, binding covalently to protein, forming a complete antigen
- Altered peptide model - drug modifies self-peptides presented by MHC
- Pharmacologic interaction (p-i concept) - drug binds noncovalently to drug-HLA or drug-TCR, triggering immune response without prior sensitization
Classification of Cutaneous Drug Reactions
Non-Severe (Common) Reactions
| Type | Features | Common Culprits |
|---|---|---|
| Exanthematous (Morbilliform) | Most common; maculopapular, measles-like; starts centrally, spreads peripherally; begins 4-21 days after starting drug | Penicillins, ampicillin, sulfonamides, allopurinol, carbamazepine |
| Urticaria / Angioedema | Transient, pruritic, edematous wheals; can be IgE-mediated (within 1 hour) or delayed | NSAIDs, aspirin, penicillin, opioids, ACE inhibitors (angioedema) |
| Fixed Drug Eruption (FDE) | Discrete, recurrent lesions at the same site each time the drug is taken; post-inflammatory hyperpigmentation; CD8+ TRM cells persist at sites | Tetracycline, NSAIDs, sulfonamides, paracetamol, trimethoprim |
| Lichenoid | Purple, flat-topped papules resembling lichen planus | Antimalarials, gold, thiazides, captopril, NSAIDs |
| Photosensitivity | Phototoxic (dose-dependent, UVA) vs. photoallergic (immunologic, UVA) | Tetracyclines (phototoxic), fluoroquinolones, amiodarone, thiazides |
| Acneiform | Follicular eruption without comedones | Corticosteroids, androgens, epidermal growth factor receptor (EGFR) inhibitors |
| Psoriasiform | Psoriasis-like plaques; may precipitate or worsen psoriasis | Beta-blockers, lithium, antimalarials, TNF inhibitors |
| Drug-Induced Lupus | ANA+, anti-histone antibodies; resolves on stopping drug | Hydralazine, procainamide, isoniazid, minocycline |
| Hyperpigmentation | Diffuse or localized skin/mucous membrane pigmentation | Minocycline (blue-gray), amiodarone, antimalarials, bleomycin |
Severe Cutaneous Adverse Reactions (SCARs)
SCARs are potentially life-threatening immune-mediated reactions. The main SCARs are:
- Anaphylaxis
- Acute Generalized Exanthematous Pustulosis (AGEP)
- DRESS / DIHS
- Generalized Bullous Fixed Drug Eruption
- Stevens-Johnson Syndrome (SJS)
- Toxic Epidermal Necrolysis (TEN)
- Anticoagulant-induced skin necrosis
1. Stevens-Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN)
SJS and TEN are on a spectrum:
- SJS: epidermal detachment <10% BSA
- SJS/TEN overlap: 10-30% BSA
- TEN: >30% BSA
Key features:
- Prodrome: fever, flu-like symptoms, burning eyes
- Targetoid lesions - atypical flat targets with dusky center
- Painful mucosal erosions (oral, ocular, genital) in >90%
- Nikolsky sign positive (skin shears off with lateral pressure)
- Epidermis separates at the dermal-epidermal junction
- Mortality: SJS ~5%, TEN ~25-30%
Pathomechanism: CD8+ T cells accumulate along the dermal-epidermal junction, causing interface dermatitis with keratinocyte apoptosis. Granulysin released by cytotoxic T cells is a key mediator of keratinocyte death.
Common drugs: Allopurinol (#1 worldwide), aromatic anticonvulsants (carbamazepine, phenytoin, phenobarbital), sulfonamides, lamotrigine, oxicam NSAIDs, nevirapine
Genetic predisposition: Strong HLA associations -
- HLA-B*5801 + allopurinol (Han-Chinese, Korean, Thai)
- HLA-B*1502 + carbamazepine (Han-Chinese)
2. DRESS (Drug Reaction with Eosinophilia and Systemic Symptoms) / DIHS
Also called Drug-Induced Hypersensitivity Syndrome (DIHS)
| Feature | Details |
|---|---|
| Onset | 2-8 weeks after starting drug (long latency is distinctive) |
| Rash | Maculopapular/morbilliform, may be >50% BSA (in 45-80%) |
| Facial edema | Very characteristic |
| Fever | >38°C in nearly all |
| Lymphadenopathy | Present |
| Eosinophilia | Hallmark; >1,500/mm³ |
| Atypical lymphocytes | Lymphocytosis with atypical forms |
| Liver involvement | Elevated LFTs; can cause fatal hepatitis |
| Herpesvirus reactivation | HHV-6, HHV-7, EBV, CMV reactivation is characteristic |
| Late sequelae | Autoimmune diseases (Hashimoto thyroiditis, SLE, Type 1 diabetes) months later |
Common drugs: Aromatic anticonvulsants (carbamazepine, phenytoin, phenobarbital), allopurinol, sulfonamides, dapsone, minocycline, lamotrigine
Genetic risk: HLA-B13:01 + dapsone (Asians); HLA-A31:01 + carbamazepine (Europeans)
3. Acute Generalized Exanthematous Pustulosis (AGEP)
- Acute onset of hundreds of non-follicular, sterile pustules on an erythematous background
- Usually starts on face/intertriginous areas, spreads rapidly
- Fever, neutrophilia
- Onset: within 48 hours (much faster than DRESS)
- Resolves spontaneously in ~2 weeks after stopping drug
- Less severe than SJS/TEN or DRESS
- Culprits: Aminopenicillins (#1), cephalosporins, macrolides, diltiazem, hydroxychloroquine
4. Fixed Drug Eruption (FDE)
- Well-demarcated, round/oval, dusky red/violaceous plaques
- Occur at the exact same site with each drug exposure
- Burn/sting, then leave post-inflammatory hyperpigmentation
- Common sites: lips, genitals, perianal region, hands
- Mechanism: CD8+ resident memory T cells (TRM) persisting at prior lesion sites
Features Suggesting a SCAR (Red Flags)
| Cutaneous | Systemic | Laboratory |
|---|---|---|
| Skin pain | High fever | Marked eosinophilia |
| Confluent erythema | Lymphadenopathy | Atypical lymphocytes |
| Facial edema | Arthralgia/arthritis | Leukopenia |
| Blisters / epidermal detachment | Shortness of breath / stridor | Abnormal LFTs / renal function |
| Mucosal erosions | Hypotension | Thrombocytopenia |
| Necrosis | Other visceral involvement | Neutrophilia |
| Palpable purpura | ||
| Urticaria | ||
| Swelling of lips/tongue |
(Adapted from Roujeau & Stern, N Engl J Med 1994)
Immunologic Classification (Gell & Coombs)
| Type | Mechanism | Examples |
|---|---|---|
| Type I (IgE-mediated) | Mast cell degranulation | Urticaria, anaphylaxis (penicillin) |
| Type II (Cytotoxic) | IgG/IgM + complement | Drug-induced hemolytic anemia, thrombocytopenia |
| Type III (Immune complex) | IgG-drug complexes in vessels | Serum sickness, vasculitis, drug fever |
| Type IV (Delayed T-cell) | CD4+/CD8+ T cells | Contact dermatitis, FDE, SJS/TEN, DRESS, AGEP |
Non-immunologic mechanisms also exist: pharmacologic (pseudoallergic reactions to NSAIDs/aspirin via COX-1 inhibition with leukotriene excess), cumulative toxicity, phototoxicity.
Risk Factors
- Immunosuppression: HIV-infected patients have 10-50x greater risk of exanthematous eruptions to sulfonamides
- Specific HLA alleles (see above)
- Polypharmacy (elderly patients)
- Impaired renal, hepatic, or cardiac function (affects drug metabolism)
- Prior drug reaction history
Diagnosis
Approach: Clinical characteristics + chronologic factors (timeline of drug exposure) + literature search
Investigations:
- IgE-specific assays (RAST/ImmunoCAP) - for IgE-mediated reactions
- Prick/intradermal skin tests - for urticaria/angioedema; contraindicated in SJS/TEN
- Patch testing (48h under occlusion on upper back) - for delayed reactions; variable sensitivity
- Lymphocyte transformation test - limited clinical utility
- CBC with differential (eosinophilia, atypical lymphocytes), LFTs, renal function, urinalysis
Rechallenge: Carries risk of more severe reaction; contraindicated after SCARs
Management Principles
- Identify and stop the culprit drug - most critical step, especially in SCARs
- Supportive care - wound care (SJS/TEN), IV fluids, nutritional support, ophthalmology consultation (mucosal involvement)
- Urticaria/angioedema: Antihistamines (H1 blockers); systemic corticosteroids for severe cases; epinephrine for anaphylaxis
- Morbilliform eruptions: Topical corticosteroids, antihistamines; usually self-limited once drug stopped
- SJS/TEN: ICU/burn unit care; cyclosporin (gaining evidence), IVIG (controversial), etanercept; avoid systemic corticosteroids in TEN (increased infection risk)
- DRESS: Systemic corticosteroids are first-line; prolonged taper (3+ months) to prevent relapse; monitor for herpesvirus reactivation and autoimmune sequelae
- AGEP: Stop culprit; topical corticosteroids; spontaneous resolution within ~2 weeks
Drugs With Highest Rates of Cutaneous Reactions
Based on large epidemiological data (Arndt & Jick), the drugs with the highest rates of cutaneous reactions per 1,000 patients include:
- Amoxicillin (~51/1,000)
- Trimethoprim-sulfamethoxazole (~59/1,000)
- Ampicillin (~52/1,000)
- Semisynthetic penicillins
- Aromatic anticonvulsants
- Allopurinol
- Sulfonamides
Low-risk drugs (rates ≤3/1,000) include: prednisone, codeine, warfarin, regular insulin, digoxin, morphine.
Newer Targeted Therapies & Immune Checkpoint Inhibitors (ICIs)
- EGFR inhibitors (cetuximab, erlotinib): Papulopustular acneiform eruption in 50-80%; xerosis, nail changes
- Anti-PD-1/PD-L1 checkpoint inhibitors (nivolumab, pembrolizumab): Wide range of immune-related adverse events (irAEs) - maculopapular rash, pruritus, lichenoid reactions, bullous disorders, vitiligo
- BRAF/MEK inhibitors: Keratoacanthoma-like tumors, hyperproliferative lesions, photosensitivity
- Tyrosine kinase inhibitors (TKIs): Hand-foot skin reaction, hair changes
Sources:
- Dermatology 2-Volume Set 5e (Bolognia et al.), Chapter 21 - Cutaneous Drug Reactions
- Fitzpatrick's Dermatology, Chapter 13 - Drug Reactions
- Barash & Stoelting's Clinical Anesthesia, 9e
This is a shared conversation. Sign in to Orris to start your own chat.