Propylthiouracil Pharmacology 6 marks question for mbbs 2nd yr University exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed. Here is the complete, exam-ready answer:
Propylthiouracil (PTU) - Pharmacology
MBBS 2nd Year | 6 Marks
1. Introduction / Classification
Propylthiouracil (PTU) belongs to the thioamide class of antithyroid drugs. The thioamide group includes:
- Propylthiouracil (PTU)
- Methimazole (Tapazole)
- Carbimazole (converted to methimazole in vivo - used in UK)
The thiocarbamide (-C=S) group is essential for antithyroid activity.
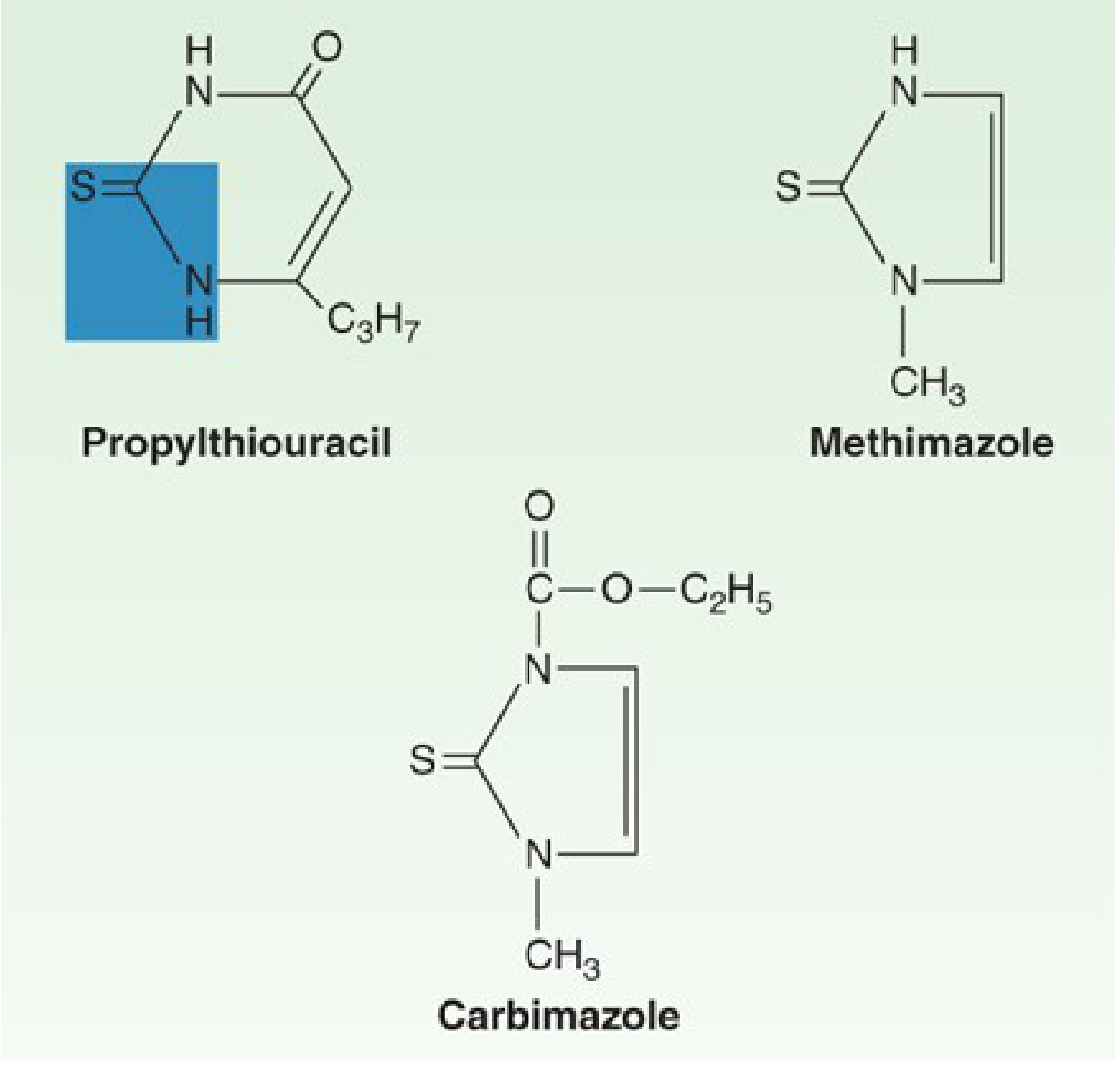
(Katzung's Basic & Clinical Pharmacology, 16e, Fig. 38-5)
2. Mechanism of Action
PTU acts by multiple mechanisms:
| Mechanism | Details |
|---|---|
| Inhibits thyroid peroxidase | Blocks iodination (organification) of tyrosyl residues of thyroglobulin - prevents formation of MIT and DIT |
| Blocks coupling reaction | Prevents coupling of iodotyrosines to form T3 (triiodothyronine) and T4 (thyroxine) |
| Inhibits peripheral deiodination | PTU (but NOT methimazole) inhibits the enzyme 5'-deiodinase, blocking conversion of T4 to the more active T3 in peripheral tissues |
Key point: PTU does NOT block iodide uptake (trapping) by the thyroid gland. Since it inhibits synthesis rather than release, onset is slow - it takes 3-4 weeks before existing T4 stores are depleted.
The extra peripheral deiodination block makes PTU the drug of choice in thyroid storm, where rapid reduction of T3 levels is needed.
3. Pharmacokinetics
| Parameter | PTU |
|---|---|
| Absorption | Rapid; peak serum levels at 1 hour |
| Bioavailability | 50-80% (incomplete absorption + first-pass effect) |
| Plasma protein binding | ~75% (higher than methimazole) |
| Plasma half-life | ~75 minutes (1.5 hours) |
| Volume of distribution | ~0.4 L/kg; concentrated in thyroid gland |
| Excretion | Kidney, mostly as inactive glucuronide within 24 hours |
Despite its short t1/2, PTU is concentrated within the thyroid gland. A single 100 mg dose can inhibit iodine organification by 60% for 7 hours, so dosing every 6-8 hours is used clinically.
Because PTU is heavily protein-bound (~75%), it crosses the placenta less readily than methimazole, making it the preferred antithyroid drug in the first trimester of pregnancy.
4. Therapeutic Uses (Clinical Indications)
- Hyperthyroidism (Graves' disease) - to control thyrotoxicosis while awaiting spontaneous remission, or as long-term therapy
- Thyroid storm - drug of choice; blocks both synthesis AND peripheral T4→T3 conversion, giving faster control
- First trimester of pregnancy - preferred over methimazole (crosses placenta less; methimazole is associated with fetal embryopathy/aplasia cutis)
- Pre-operative preparation for thyroid surgery - to render the patient euthyroid
- Adjunct to radioactive iodine (RAI) - to hasten recovery while awaiting the effect of RAI
Usual dose: 100 mg every 8 hours orally; increased to every 4-6 hours if doses >300 mg/day are needed.
5. Adverse Effects
Common (3-12% of patients):
- Maculopapular pruritic rash (most common - 4-6%)
- Nausea, GI distress (early)
Serious / Dangerous:
| Adverse Effect | Details |
|---|---|
| Agranulocytosis | Most dangerous; occurs in 0.1-0.5% of patients. Granulocyte count <500 cells/mm³. Usually in first 90 days. Rapidly reversible on stopping drug. Patient should report sore throat or fever immediately |
| Fulminant hepatic necrosis | Rare but devastating, ~1 in 10,000 adults. Can cause death or require liver transplant. Black box FDA warning for PTU |
| Aplastic anemia | Rare |
| Lupus-like syndrome / ANCA-positive vasculitis | Long-term PTU use stimulates ANCA (anti-MPO antibodies) formation |
| Hypoprothrombinemia | Rare |
PTU vs. Methimazole Adverse Effect Comparison:
- PTU: Severe hepatitis / fulminant liver failure (black box warning)
- Methimazole: Cholestatic jaundice (more common than PTU); altered sense of taste/smell
- Cross-sensitivity between the two drugs is ~50%
6. Contraindications / Precautions
- Children and adults - avoid PTU unless no alternatives (due to liver failure risk); methimazole preferred
- Second and third trimester of pregnancy - switch to methimazole (PTU-related liver risk to mother; both can cause fetal hypothyroidism)
- Monitor for agranulocytosis; advise patients to report sore throat, fever, or oral ulcers
7. PTU vs. Methimazole - Key Differences (Exam Favourite)
| Feature | PTU | Methimazole |
|---|---|---|
| Potency | Less potent | ~10x more potent |
| Peripheral deiodination block | Yes (T4→T3) | No |
| Protein binding | ~75% | Nil |
| Plasma t1/2 | 75 min | 4-6 h |
| Dosing | Every 6-8 hours | Once daily |
| Drug of choice in thyroid storm | YES | No |
| Drug of choice in 1st trimester | YES | Avoid (embryopathy) |
| Liver toxicity | Severe hepatic necrosis (black box) | Cholestatic jaundice |
| Preferred drug overall | No | YES (for adults, children) |
Summary Mnemonic for PTU Actions: "PTU - 3 STOPS"
- Stops thyroid peroxidase (organification)
- Stops coupling of iodotyrosines
- Stops peripheral conversion of T4 → T3 (unique to PTU)
Sources: Katzung's Basic & Clinical Pharmacology (16e), Goodman & Gilman's Pharmacological Basis of Therapeutics (14e)
This is a shared conversation. Sign in to Orris to start your own chat.