Radial head replacement
Reading File
Finding Sources
Searching PubMed
"radial head replacement" arthroplasty
Finding Sources
Searching PubMed
"radial head" arthroplasty outcomes
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough answer. Here is a complete overview of radial head replacement:
Radial Head Replacement (Arthroplasty)
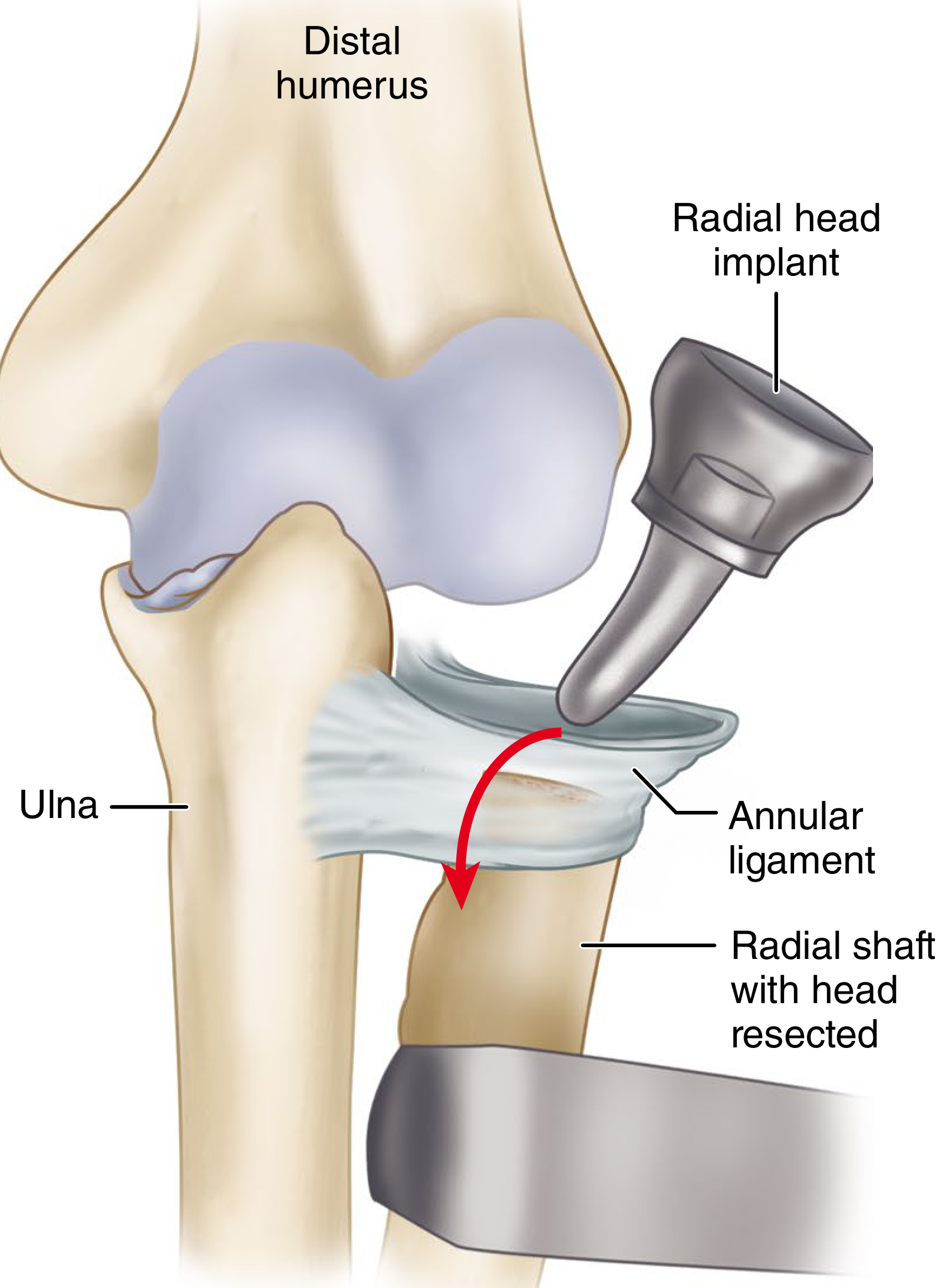
Radial head implant being seated into the proximal radial canal after resection, with the annular ligament incised transversely - Campbell's Operative Orthopaedics 15th Ed 2026
Indications
Radial head replacement is indicated when the radial head cannot be reconstructed by open reduction and internal fixation. Specific scenarios include:
- Comminuted radial head fractures (Mason III/IV) associated with elbow dislocation - the lateral ulnar collateral ligament (LUCL) is typically injured, making prosthetic replacement necessary to stabilize the joint and allow early mobilization
- Terrible Triad injuries (elbow dislocation + radial head fracture + coronoid fracture) - a metal replacement is performed after coronoid fracture fixation, since radial head removal provides excellent coronoid exposure
- Essex-Lopresti lesion (radial head fracture + distal radioulnar joint dislocation) - a prosthesis prevents proximal radial migration that would otherwise occur after simple excision
- Fractures with concomitant medial collateral ligament rupture or coronoid fracture adding to elbow instability
- Situations with significant instability of the elbow, radial forearm axis, or DRUJ from injury or disease
Short-term outcomes of radial head arthroplasty for comminuted fractures have been reported as superior to ORIF at short-term follow-up. - Campbell's Operative Orthopaedics 15th Ed 2026, p.808
Prosthesis Design
Design has evolved considerably over time:
| Type | Features | Notes |
|---|---|---|
| Monoblock | Single-piece metallic head | Original designs; less size-matching ability |
| Modular | Separate head + stem components | Current standard; allows better diameter and height matching |
| Bipolar | Articulating head on a stem | May reduce capitellar wear; some debate on advantage |
| Smooth-stemmed | Non-porous stem | Lower osteolysis rates than porous ingrowth |
| Press-fit | Interference fit in canal | Risk of loosening and osteolysis over time |
| Cemented | Bone cement fixation | Also associated with loosening long-term |
| Silicone | Older design | Abandoned - unacceptably high failure rates |
No evidence supports one metallic design over others, except that silicone prostheses have been definitively abandoned.
Surgical Technique (Campbell's Technique 15.4)
Positioning: Supine with arm board; fluoroscopy used throughout.
Approach:
- Incision begins superior to the lateral epicondyle, extends ~6 cm distally
- Extensor digitorum communis (EDC) split or Kaplan approach - when the LUCL is intact
- Kocher approach (between ECU and anconeus) - when the LUCL is disrupted
Key steps:
- Develop the lateral capsule and expose the radial neck
- If a coronoid fracture is present, repair it first (radial head resection improves coronoid access)
- Incise the annular ligament transversely to expose the radial canal end-on
- Cut the radial neck just proximal to the fracture site
- Prepare the medullary canal with burrs or rasps
- Cut the proximal radial surface flat for full contact with the prosthesis collar
- Achieve a tight press-fit; use trial prosthesis to confirm radiocapitellar contact under fluoroscopy
- Check range of motion (flexion-extension, pronation-supination) and implant tracking
- Insert the final prosthesis
- Repair the LUCL to its isometric point at the capitellar rotation center (suture anchor or drill holes); the ulnohumeral joint must be held reduced during this step
Sizing principles (critical):
- Reassemble excised fragments on the back table to estimate native diameter and thickness
- The native radial head is elliptical and offset; most implants are axisymmetric
- Optimal diameter = minor axis of the ellipse (typically ~2 mm smaller than maximum diameter)
- The proximal edge of the prosthesis should be level with the lateral coronoid edge (native position is 0.9 mm distal to it)
- Avoid overstuffing - more than 2 mm of lengthening increases radiocapitellar contact pressures
- When between sizes, choose the smaller diameter and smaller thickness
"Overlengthening of the radial head is the commonest technical cause of failed radial head arthroplasty." - Rockwood and Green's Fractures in Adults 10th Ed 2025
Lateral decubitus position may be preferred when treating concomitant olecranon or proximal ulna fractures.
Sizing Pitfalls
Incorrect sizing is the most common intraoperative problem. Radiographic parameters are unreliable; the most useful sizing guides are:
- The reassembled excised radial head fragments
- The relationship of the prosthesis to the proximal ulna (lateral coronoid edge)
- Intraoperative fluoroscopy assessing ulnohumeral joint gapping (lateral ulnohumeral gapping = overstuffing)
- Ipsilateral ulnar variance can drop if the head is oversized
An implant that is too large:
- Increases tension on the interosseous membrane
- Causes stiffness and pain
- Produces capitellar wear and erosion of the lateral trochlea
- May prevent proper annular ligament closure
Outcomes
- Good to excellent results in ~80% of patients
- 10-20% reduction in grip/elbow strength
- Pain relief is typically excellent
- Elbow flexion-extension and forearm rotation arcs are within 10-20 degrees of normal
- Ulnohumeral joint stability is generally maintained
- Return to high-demand activities (sports, military) has a more guarded prognosis
Long-term concerns:
- Stem loosening - reported in one-third or more of press-fit designs; causes significant proximal radial osteolysis and typically necessitates removal
- Rigid fixation (porous ingrowth, cemented) is linked to higher complication and revision rates
- Smooth-stemmed implants show lower osteolysis rates than porous ingrowth designs
- Mid-term follow-up (>8 years) with smooth-stemmed modular implants shows preserved good outcomes
Postoperative Management
After prosthesis insertion and LUCL repair, if residual elbow instability remains despite fixation and ligament repair:
- A hinged external fixator or internal joint stabilizing system (internal joint stabilizer, e.g., Orbay et al.) can augment stability
- Tape suture augmentation of the ligament repair is a described reliable technique
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026, pp. 808-810 (Technique 15.4)
- Rockwood and Green's Fractures in Adults 10th Ed 2025, pp. 1669+ (Key Surgical Steps, Pitfalls)
Recent literature (PubMed 2023-2026):
- Monir & Wagner, Hand Clin 2025 - "Updates on Radial Head Arthroplasty in Trauma" [PMID: 41106923]
- Celli et al., Arch Orthop Trauma Surg 2024 - Long-term outcomes with bipolar prosthesis [PMID: 38568386]
- Heifner et al., Hand (NY) 2024 - Revision of failed RHA [PMID: 36752100]
This is a shared conversation. Sign in to Orris to start your own chat.