Angina -Perioperative management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"angina" AND "perioperative management" AND "noncardiac surgery"
Finding Sources
Finding Sources
Searching PubMed
"coronary artery disease" AND "perioperative" AND "noncardiac surgery"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have all the content needed for a comprehensive answer. Let me compile it:
Perioperative Management of Angina
1. Preoperative Risk Stratification
Step 1: Urgency of Surgery
- Emergency surgery: Proceed immediately. Use clinical risk factors to guide perioperative monitoring; no cardiac workup required.
- Elective/urgent surgery: Full stepwise evaluation is warranted.
Step 2: Screen for Active Cardiac Conditions (Unstable Angina = Major Risk)
Patients with any of the following active cardiac conditions must be evaluated and stabilized before elective surgery:
- Unstable angina (ACS) — highest priority; treat per ACS guidelines first
- Decompensated heart failure
- Significant arrhythmias
- Severe valvular disease
"The presence of unstable angina has been associated with a high perioperative risk of myocardial infarction (MI). The perioperative period is associated with a hypercoagulable state and surges in catecholamines." — Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
"Chronic stable (mild to moderate) angina does not seem to increase perioperative risk substantially." — Morgan and Mikhail's Clinical Anesthesiology, 7e
Step 3: Estimate MACE Risk (Clinical + Surgical)
Use the Revised Cardiac Risk Index (RCRI) — 6 independent predictors:
- High-risk surgery (intraperitoneal, intrathoracic, suprainguinal vascular)
- History of ischemic heart disease
- History of congestive heart failure
- History of cerebrovascular disease
- Diabetes mellitus on insulin
- Preoperative creatinine >2.0 mg/dL
RCRI score ≥3 = elevated risk; consider further evaluation or β-blocker therapy.
The ACS NSQIP risk calculator is endorsed as an alternative or supplement to RCRI.
2. Perioperative Assessment Algorithm
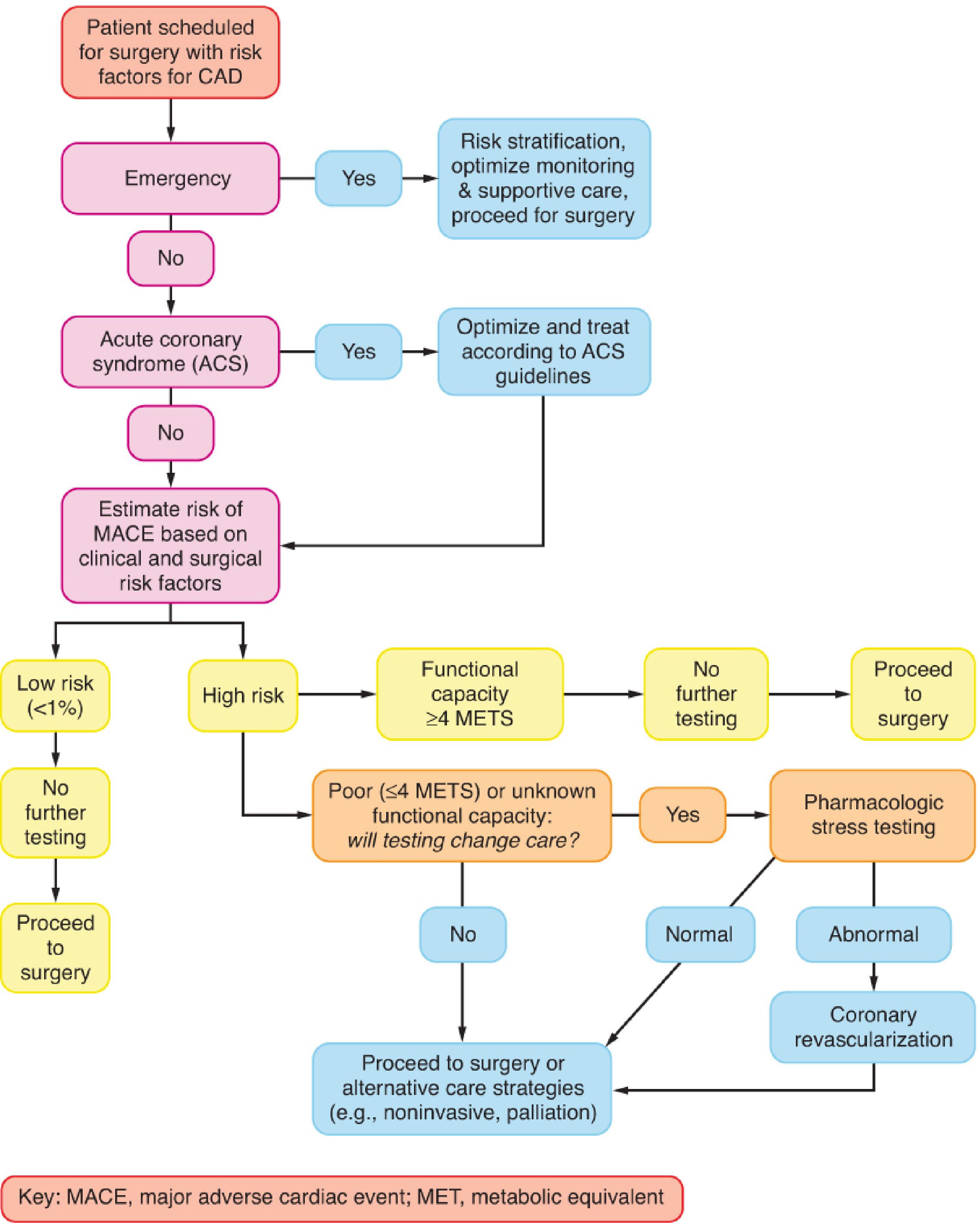
Figure: Stepwise approach to perioperative cardiac assessment for patients with CAD. Modified from ACC/AHA 2014 guideline. — Barash, Clinical Anesthesia, 9e
Functional Capacity Assessment (METs)
- ≥4 METs without symptoms: Proceed to surgery — no further testing needed
- <4 METs or unknown capacity: Further testing warranted only if it will change management
| MET Level | Example Activity |
|---|---|
| 1–2 METs | Eating, dressing, walking slowly |
| 4 METs | Climbing a flight of stairs, walking on level ground at 4 mph |
| >10 METs | Strenuous sports (swimming, tennis) |
3. Preoperative Investigations
| Test | Indication |
|---|---|
| 12-lead ECG | Known CAD, arrhythmia, PAD, cerebrovascular disease; any patient with non-low-risk surgery |
| Echocardiography (TTE) | Dyspnea of unknown origin; prior HF with worsening symptoms; LVEF <35% associated with highest MACE risk |
| Exercise ECG stress test | Suspected CAD; sensitivity 70–80%, specificity 60–75% |
| Pharmacologic stress test (DSE or MPI) | Patients unable to exercise with poor functional capacity (<4 METs) and ≥3 RCRI factors; perform only if results will change management |
| Coronary angiography | If stress test is abnormal and revascularization is being considered |
"A normal dobutamine stress echocardiogram (DSE) or myocardial perfusion imaging (MPI) result suggests a low risk for perioperative cardiac complications." — Barash, Clinical Anesthesia, 9e
4. Perioperative Medication Management
β-Blockers (ACC/AHA Recommendations)
| Recommendation | Class | LOE |
|---|---|---|
| Continue β-blockers in patients already on them chronically | I | B |
| Do NOT start β-blockers on the day of surgery | III: Harm | B |
| In patients with ≥3 RCRI factors, may begin β-blockers before surgery | IIb | B |
| If initiating, begin ≥1 day before surgery to assess safety/tolerability | IIb | B |
"Acutely initiating therapy with β-blockers in at-risk patients who will undergo surgery is no longer recommended." — Morgan and Mikhail's Clinical Anesthesiology, 7e
Key concern: The POISE trial demonstrated that initiating high-dose metoprolol reduced MI but significantly increased stroke and all-cause mortality.
Statins
| Recommendation | Class | LOE |
|---|---|---|
| Continue statins in patients currently on them | I | B |
| Initiate statins in patients undergoing vascular surgery | IIa | B |
| Acute perioperative statin withdrawal is associated with adverse outcomes | — | — |
Antiplatelet Therapy (Aspirin/DAPT)
- Chronic aspirin for CAD: continue perioperatively in most cases unless bleeding risk outweighs benefit
- DAPT in patients with coronary stents: critical — see stent timing below
Nitrates
- Continue long-acting nitrates perioperatively
- Administer sublingual GTN if angina occurs; have IV nitrates available in high-risk cases
- Avoid hypotension (especially with neuraxial anesthesia)
ACE Inhibitors / ARBs
- Continue in patients with HF or LV dysfunction
- Many anesthesiologists hold on the morning of surgery to prevent refractory intraoperative hypotension — an individualized decision
5. Coronary Revascularization Before Noncardiac Surgery
| Recommendation | Class | LOE |
|---|---|---|
| Revascularization is recommended when indicated by existing CPGs (i.e., independent of surgery) | I | C |
| Revascularization NOT recommended solely to reduce perioperative cardiac events | III: No Benefit | B |
Timing of Elective Surgery After PCI
| Intervention | Minimum Delay |
|---|---|
| Balloon angioplasty | 14 days |
| Bare-metal stent (BMS) | 30 days |
| Drug-eluting stent (DES) — optimal | 365 days |
| DES — may consider | 180 days (IIb) |
| Never: within DAPT window if DAPT must be stopped | III: Harm |
"Elective noncardiac surgery should not be performed in patients in whom DAPT will need to be discontinued perioperatively within 30 days after BMS or within 12 months after DES implantation." — Morgan and Mikhail's Clinical Anesthesiology, 7e
6. Intraoperative Management
Anesthetic Goals
- Avoid tachycardia — most important determinant of myocardial O₂ demand; heart rate <80 bpm is the target
- Avoid hypotension — maintain coronary perfusion pressure (MAP ≥65 mmHg)
- Prevent hypertension — avoids increased afterload and wall stress
- Avoid hypothermia — causes shivering and catecholamine surges
Monitoring
- ST-segment monitoring is mandatory: lead II (inferior MI) + lead V5 (anterior MI) detects ~95% of intraoperative ischemia
- Invasive arterial line for high-risk patients undergoing major surgery
- PA catheter / TEE: reserved for high-risk patients with known severe ventricular dysfunction
Anesthetic Technique
- Both regional and general anesthesia are acceptable; neither has been conclusively proven superior
- Neuraxial (epidural/spinal) provides excellent analgesia, blunts sympathetic response — but risk of hypotension must be managed, particularly in tight coronary stenosis
- Avoid high-dose inhalational agents that may cause excessive vasodilation
Treatment of Intraoperative Ischemia
| Trigger | Intervention |
|---|---|
| Tachycardia | β-blocker (IV esmolol/metoprolol) |
| Hypertension | Deepen anesthesia, nitroglycerin, labetalol |
| Hypotension | Vasopressor (phenylephrine), fluid, reduce anesthetic depth |
| ST depression/elevation | IV nitroglycerin; optimize HR and BP |
| Refractory ischemia | Consider stopping surgery; urgent cardiology consult |
7. Postoperative Management
- Troponin monitoring: measure in patients with signs/symptoms suggesting myocardial injury; routine surveillance in high-risk patients is debated but increasingly practiced (MINS — myocardial injury after noncardiac surgery)
- Continue or restart all cardiac medications (β-blockers, statins, nitrates, antiplatelets) promptly
- Adequate analgesia is critical — inadequate pain control causes catecholamine surges and tachycardia
- Epidural analgesia post-major vascular/thoracic surgery blunts sympathoadrenal response
- Monitor for: MI, arrhythmias, acute HF
- Resume DAPT as soon as surgical hemostasis is secured in patients with coronary stents
8. Special Situations
Unstable Angina / NSTEMI Before Planned Surgery
- Postpone all non-emergency surgery
- Treat as ACS: anticoagulation, antiplatelets, β-blockers, nitrates, statins
- Revascularize if indicated; re-assess timing of surgery after stabilization (DES stent timing applies)
Vasospastic (Prinzmetal's) Angina
- Calcium channel blockers and nitrates are the mainstay — continue perioperatively
- Avoid vasoconstrictors (ergotamine, high-dose vasopressors) that may trigger spasm
- Avoid hyperventilation (causes coronary vasoconstriction)
Combination Therapy Caution
"Patients with ventricular dysfunction may not tolerate the combined negative inotropic effect of a β-blocker and a calcium channel blocker together; an ACE inhibitor or ARB is better tolerated. The additive effect of a β-blocker and calcium channel blocker on the AV node may precipitate heart block in susceptible patients." — Morgan and Mikhail's Clinical Anesthesiology, 7e
Summary
| Phase | Key Action |
|---|---|
| Preop | Risk stratify (RCRI/MACE), assess functional capacity, identify unstable angina, optimize medications, determine stent timing |
| Intraop | Avoid tachycardia/hypotension, ST monitoring, continue cardiac drugs, treat ischemia aggressively |
| Postop | Restart medications promptly, adequate analgesia, troponin surveillance, early cardiology involvement if needed |
Sources:
- Morgan and Mikhail's Clinical Anesthesiology, 7e — Chapter 21 (Preoperative Management/CAD)
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e — Chapter 23 (Cardiovascular System/Preoperative Assessment)
- Sabiston Textbook of Surgery, 21e — Chapter 19 (Perioperative Cardiac Assessment)
- Harrison's Principles of Internal Medicine, 22e — Perioperative Cardiac Risk Assessment
This is a shared conversation. Sign in to Orris to start your own chat.