Absorption, biochemical functions and deficiency manifestation of vitamin b12
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
I now have comprehensive, well-sourced information to construct a detailed answer. Let me compile everything:
Vitamin B12 (Cobalamin) - Absorption, Biochemical Functions & Deficiency
1. Structure Overview
Vitamin B12 contains a corrin ring system (resembling the porphyrin ring of heme) with cobalt held at its center by four pyrrole nitrogen coordination bonds. The remaining coordination bonds of cobalt connect to 5,6-dimethylbenzimidazole and, in the commercial form, cyanide (cyanocobalamin).
The two physiologically active coenzyme forms are:
- Methylcobalamin - used in cytosol
- 5'-Deoxyadenosylcobalamin - used in mitochondria
(Lippincott Illustrated Reviews: Biochemistry, p. 1053-1054)
2. Dietary Sources & Body Stores
- Found in liver, red meat, fish, eggs, dairy, and fortified cereals
- Synthesized only by microorganisms - absent in plants, making strict vegans at risk
- Average Western diet provides 5-30 µg/day; RDA is 2.4 µg/day; absorption is 1-5 µg/day
- Total body stores: 2-5 mg (1 mg in liver) - sufficient for 3-5 years, explaining why dietary deficiency takes years to manifest
3. Absorption of Vitamin B12
This is a multi-step process involving several binding proteins:
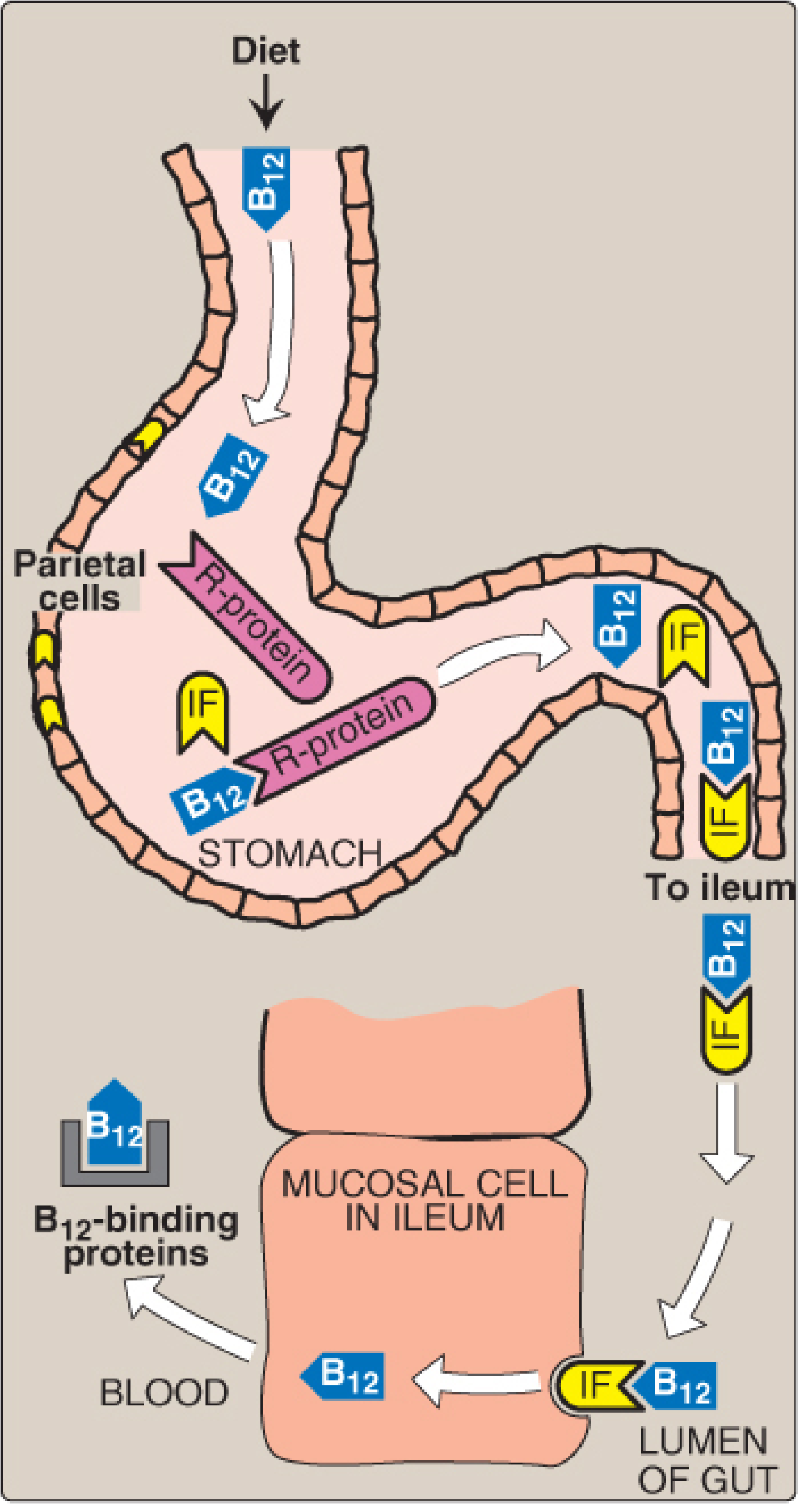
Figure: Absorption of Vitamin B12 (Lippincott Illustrated Reviews: Biochemistry)
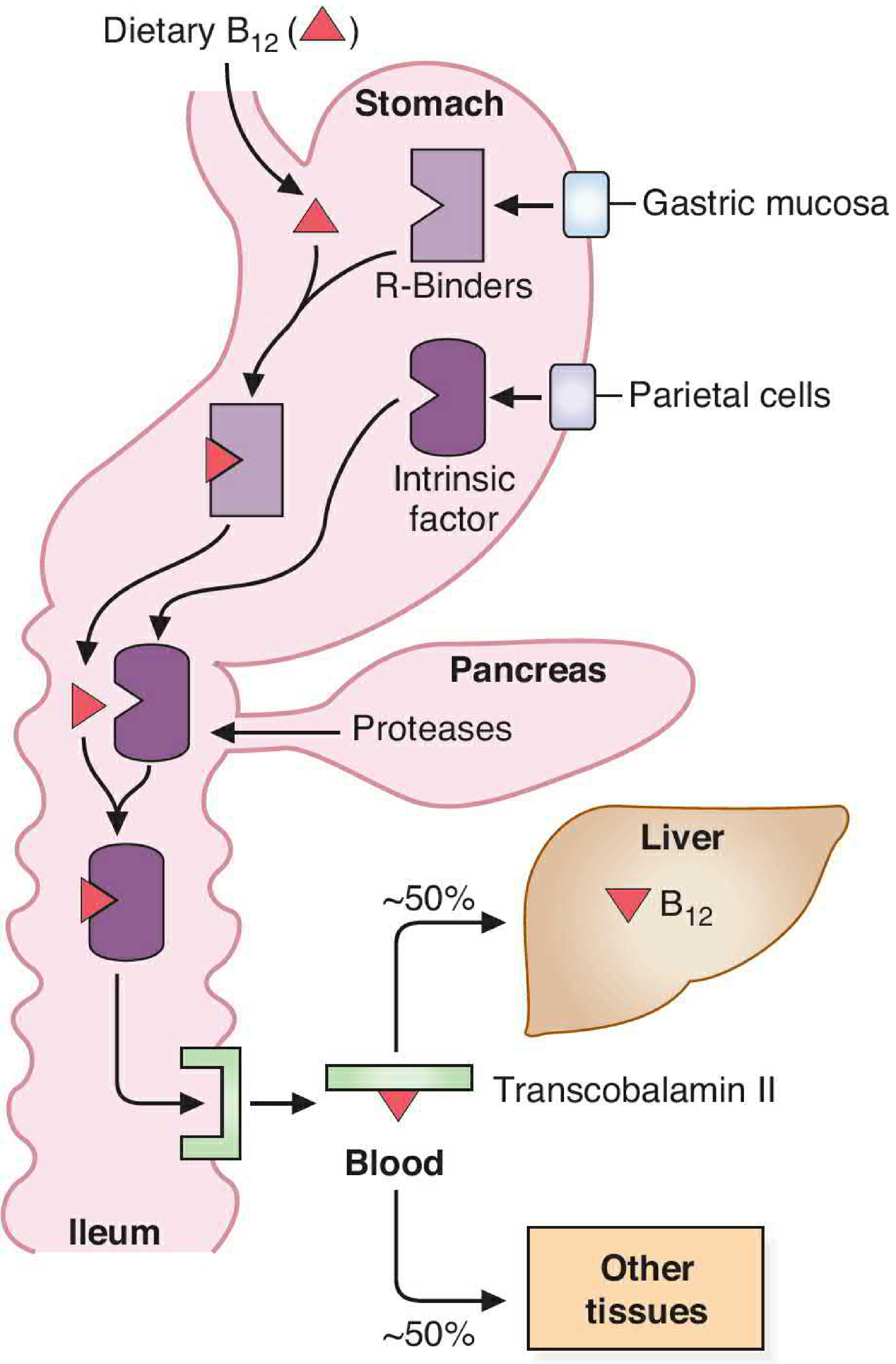
Figure: Absorption, transport, and storage of Vitamin B12 (Basic Medical Biochemistry, 6e)
Step-by-step mechanism:
| Step | Location | Event |
|---|---|---|
| 1. Release from food | Stomach (acidic pH) | Gastric acid releases B12 from dietary proteins. Achlorhydria in the elderly impairs this step. |
| 2. Binding to R-protein (haptocorrin) | Stomach | Free B12 binds to haptocorrins (R-binders) secreted by salivary glands and gastric mucosa. B12 prefers R-protein over intrinsic factor at gastric pH. |
| 3. Pancreatic protease digestion | Small intestine (duodenum) | Pancreatic proteases degrade R-protein, releasing free B12. Pancreatic insufficiency blocks this step. |
| 4. Binding to Intrinsic Factor (IF) | Small intestine | Free B12 binds to intrinsic factor (IF), a glycoprotein secreted by gastric parietal cells. This complex is resistant to digestion. |
| 5. Receptor-mediated uptake | Terminal ileum | The B12-IF complex binds to cubilin (receptor) on ileal mucosal cells. Internalization requires the transmembrane protein amnionless. IF is released; B12 enters the enterocyte. |
| 6. Transport in blood | Portal circulation | Inside the enterocyte, B12 binds to Transcobalamin II (TC II) - the main transport protein. TC II delivers B12 to liver (~50%) and other tissues (~50%). |
| 7. Storage | Liver (primarily) | Stored B12 is released into bile and undergoes efficient enterohepatic recycling in the ileum. |
Note: About 1% of B12 can be absorbed by passive diffusion without IF - the rationale for high-dose oral supplementation even in pernicious anemia.
(Basic Medical Biochemistry, 6e, p. 1390-1391; Lippincott Illustrated Reviews: Biochemistry, p. 1056-1057)
4. Biochemical Functions
Cobalamin is a cofactor for two essential enzymatic reactions:
Reaction 1: Homocysteine → Methionine (Cytosol)
Enzyme: Methionine synthase (homocysteine methyltransferase)
Coenzyme form: Methylcobalamin
Co-substrate: N5-methyl THF (folate)
Coenzyme form: Methylcobalamin
Co-substrate: N5-methyl THF (folate)
- B12 accepts a methyl group from N5-methyl-THF and transfers it to homocysteine, regenerating methionine
- This reaction regenerates THF from N5-methyl-THF - the only reaction that does so
- Methionine is used to form S-adenosylmethionine (SAM), the universal methyl donor for DNA, RNA, and protein methylation
Reaction 2: Methylmalonyl-CoA → Succinyl-CoA (Mitochondria)
Enzyme: Methylmalonyl-CoA mutase
Coenzyme form: 5'-Deoxyadenosylcobalamin
Coenzyme form: 5'-Deoxyadenosylcobalamin
- Converts methylmalonyl-CoA (produced from catabolism of valine, isoleucine, threonine, methionine, and odd-chain fatty acids) to succinyl-CoA, which enters the TCA cycle
- B12 deficiency causes accumulation of methylmalonyl-CoA and its precursor propionic acid, leading to incorporation of abnormal odd-chain and branched fatty acids into cell membranes - including CNS neurons
(Lippincott Illustrated Reviews: Biochemistry, p. 1053; Bradley and Daroff's Neurology, p. 475)
The Folate Trap (Methyl-Folate Trap Hypothesis)
When B12 is deficient, THF cannot be regenerated from N5-methyl-THF. As a result:
- Folate becomes "trapped" as N5-methyl-THF
- N5,N10-methylene-THF (needed for thymidylate synthesis) is depleted
- DNA synthesis in rapidly dividing cells (bone marrow, intestinal mucosa) fails → megaloblastic anemia
This explains why B12 and folate deficiency both cause identical megaloblastic anemia.
5. Deficiency Manifestations
A. Hematological - Megaloblastic Anemia
- Macrocytic (megaloblastic) anemia - impaired DNA synthesis causes large, abnormal red cell precursors (megaloblasts)
- Peripheral blood: hypersegmented neutrophils (>5 lobes), macro-ovalocytes
- Bone marrow: nuclear-cytoplasmic dissociation - large cells with immature nuclei but mature cytoplasm
- Folate supplementation can correct the anemia but masks B12 deficiency, allowing neurological damage to progress - a critical clinical pitfall
B. Neurological - Subacute Combined Degeneration (SCD)
The hallmark neurological syndrome of B12 deficiency is subacute combined degeneration of the spinal cord - involving both the posterior (dorsal) columns and the lateral corticospinal tracts.
The mechanism: Impaired methylmalonyl-CoA mutase → abnormal fatty acid incorporation into myelin membranes → demyelination.
Clinical progression:
- Early: Symmetric paresthesias (tingling, "pins and needles") in hands first, then feet; the hands are typically affected before the lower limbs
- Sensory signs: Loss of vibration sense (most consistent sign), impaired proprioception, sensory ataxia - large fiber modalities affected preferentially
- Motor signs: Weakness (initially proximal legs), spasticity, hyperreflexia, upgoing plantars (Babinski); paradoxically, reflexes may initially be absent (neuropathy component)
- Gait: Initially ataxic, later ataxic + spastic; Romberg's sign positive
- Late/severe: Paraplegia, dementia, psychosis ("megaloblastic madness"), optic neuropathy with centrocecal scotomata
Lhermitte's sign (electric shock sensation down the spine on neck flexion) may occur.
MRI: T2 hyperintensity in posterior ± lateral columns of the cord.
CNS damage from B12 deficiency is irreversible once established. At least 50% of patients have some permanent neurological deficit even with treatment.
(Adams and Victor's Neurology, 12e, p. 1176; Harrison's Internal Medicine 22e, p. 3655)
C. Other Manifestations
| System | Feature |
|---|---|
| GI | Glossitis (smooth, red, sore tongue - "beefy red tongue"), angular stomatitis, anorexia, diarrhea |
| Psychiatric | Irritability, depression, cognitive decline, dementia, frank psychosis |
| Ophthalmic | Optic neuropathy, bilateral centrocecal scotomata |
| Autonomic | Urinary sphincter dysfunction, impotence |
| Labs | Elevated methylmalonic acid (MMA) and homocysteine - most sensitive markers; anemia and macrocytosis may be absent in up to 40% of neurological cases |
6. Common Causes of Deficiency
| Cause | Mechanism |
|---|---|
| Pernicious anemia | Autoimmune destruction of gastric parietal cells → no IF. Anti-parietal cell antibodies in ~90%, anti-IF antibodies in ~60% |
| Dietary (vegans, strict vegetarians) | No animal product intake |
| Gastrectomy / gastric bypass | Loss of parietal cells and IF |
| Ileal resection / Crohn's disease | Loss of absorption site |
| Pancreatic insufficiency | R-protein not degraded; B12 can't bind IF |
| Achlorhydria / PPI use | B12 not released from food proteins |
| Bacterial overgrowth | Bacteria consume B12 before absorption |
| Fish tapeworm (Diphyllobothrium latum) | Parasite competes for B12 |
| Nitrous oxide (N2O) | Irreversibly oxidizes cobalt in cobalamin, inactivating methionine synthase - causes acute SCD even with normal serum B12 |
7. Diagnosis & Treatment
- Serum B12 levels - can be falsely normal (up to 40% of neurological cases lack anemia/macrocytosis)
- Serum methylmalonic acid (MMA) - elevated; most specific metabolic marker
- Serum homocysteine - elevated (but also elevated in folate deficiency)
- Schilling test - classically used to evaluate B12 absorption (determines if deficiency is due to lack of IF)
- Anti-parietal cell and anti-IF antibodies confirm pernicious anemia
Treatment:
- Pernicious anemia / malabsorption: Cyanocobalamin 1000 µg IM weekly × 4 weeks, then monthly for life
- Dietary deficiency / food-cobalamin malabsorption: Oral cyanocobalamin 1000 µg/day (1% passive absorption compensates for lack of IF)
- Folate + B12 should both be given until the specific cause is established
Sources:
- Lippincott Illustrated Reviews: Biochemistry, 8th ed., pp. 1053-1058
- Basic Medical Biochemistry: A Clinical Approach, 6e, pp. 1389-1392
- Adams and Victor's Principles of Neurology, 12th ed., pp. 1175-1178
- Harrison's Principles of Internal Medicine, 22e (2025), p. 3655
- Bradley and Daroff's Neurology in Clinical Practice, p. 475
This is a shared conversation. Sign in to Orris to start your own chat.