Gullen beery syndrome every detail
Guillain-Barré syndrome complete overview pathophysiology clinical features treatment
"Guillain-Barre syndrome"[MeSH Terms] AND review
Guillain-Barré Syndrome (GBS) - Complete Overview
You likely meant Guillain-Barré syndrome (often phonetically rendered as "Gullen beery" or "Ghee-yan Bah-ray"). Here is every detail from authoritative sources.
1. Definition
- Also called: Acute Inflammatory Demyelinating Polyradiculoneuropathy (AIDP) in its classic form
- Named after: Georges Guillain, Jean Alexandre Barré, and André Strohl, who described the key features in 1916: motor weakness, areflexia, paresthesias, and CSF albuminocytological dissociation
2. Epidemiology
| Feature | Data |
|---|---|
| Annual incidence | ~1-2 per 100,000 population |
| Sex ratio | Males > Females (1.5:1) |
| Age distribution | All ages; incidence increases with age |
| <18 years | ~0.8 per 100,000 |
| >60 years | ~3.2 per 100,000 |
| Seasonality | Nonseasonal (except AMAN in northern China: summer epidemics) |
| Mortality | 1%-5% (down from 33% before positive-pressure ventilation) |
| Long-term disability | Up to 20% of hospitalized survivors |
- Bradley and Daroff's Neurology in Clinical Practice, p. 2663
3. Pathophysiology
Trigger - Molecular Mimicry
Immune Mechanisms (Dual)
- T cell-mediated immunity: Activated macrophages, guided by sensitized T cells, invade the endoneurium and strip myelin from axons. Transfer of these T cells to naive animals reproduces the lesion in animal models.
- Antibody-mediated (humoral) immunity: Circulating IgG and IgM antibodies bind to myelin and axonal antigens, activating the classical complement pathway. Macrophage cytoplasmic processes penetrate the basement membrane of Schwann cells (especially at the nodes of Ranvier) and physically strip myelin lamellae - which are then engulfed by macrophages.
Key Pathogen Associations
| Organism | Notes |
|---|---|
| Campylobacter jejuni | Strongest association; capsular antigens mimic nerve gangliosides; linked to AMAN subtype |
| Epstein-Barr virus | Common trigger |
| Cytomegalovirus (CMV) | Common trigger |
| Mycoplasma pneumoniae | Upper respiratory illness |
| Zika virus | Epidemiologically significant |
| HIV | Also implicated |
| SARS-CoV-2 | Reported association (including post-COVID) |
| Vaccines | Rarely: influenza, varicella-zoster, non-mRNA COVID vaccines |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1126-1127
- Robbins & Kumar Basic Pathology, p. 809
4. Morphology / Histology
-
Macroscopic: Nerve roots appear swollen, most prominently at the proximal spinal roots
-
Light microscopy (H&E): Perivenular and endoneurial infiltration by macrophages, variable lymphocytes, and few plasma cells
-
Key lesion: Segmental demyelination and remyelination of peripheral nerves - most prominent close to the nerve roots
-
Electron microscopy: Macrophage processes penetrate Schwann cell basement membrane at nodes of Ranvier, extend between myelin lamellae, and strip the myelin sheath from the axon - remnants are engulfed by macrophages
-
Axonal damage: Secondary axonal injury occurs (more prominent in severe disease and in AMAN/AMSAN subtypes)
-
Since both spinal nerve roots AND peripheral nerves are affected, GBS is technically classified as a radiculoneuropathy
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1126-1127
5. Classification - Subtypes and Variants
Common Subtypes
| Subtype | Features |
|---|---|
| AIDP (Acute Inflammatory Demyelinating Polyradiculoneuropathy) | Classic form; most common in Europe and North America; demyelinating; lymphocytic infiltration of myelin sheath |
| AMAN (Acute Motor Axonal Neuropathy) | Pure motor paralysis, sensory function intact; axonal (not demyelinating); first described in northern China; summer epidemics in children/young adults; strong association with C. jejuni; most common axonal form in Asia |
| AMSAN (Acute Motor-Sensory Axonal Neuropathy) | Involves both motor and sensory axons; severe; poor recovery |
Rare Variants
| Variant | Key Features |
|---|---|
| Miller-Fisher Syndrome (MFS) | Ophthalmoplegia + Ataxia + Areflexia (the triad); 6% of GBS in Western countries, up to 18% in Taiwan; associated with anti-GQ1b antibodies |
| Ataxic variant (acute ataxic neuropathy) | Prominent ataxia |
| Pharyngeal-cervical-brachial variant | Weakness of pharyngeal, cervical, and brachial muscles |
| Facial diplegia with paresthesias | Bilateral facial palsy |
| Multiple cranial neuropathy variant | Multiple cranial nerve palsies |
| Paraparetic variant | Predominantly lower limb weakness |
| Acute pandysautonomia | Severe autonomic dysfunction |
- Bradley and Daroff's Neurology in Clinical Practice, p. 2663
6. Clinical Features
Symptom Timeline
- Antecedent event: Infection 1-4 weeks before neurological onset
- Onset: Weakness and/or paresthesias, often worse in hands and fingers
- Progression: Symptoms worsen over days to 4 weeks (usually <2 weeks to nadir)
- Plateau: Reached within 4 weeks in the vast majority
- Recovery: Begins 2-4 weeks after progression stops; may take weeks to a year
Motor Features
- Ascending, fairly symmetrical weakness: Begins in lower limbs, ascends proximally, may involve arms, facial/oropharyngeal muscles, and respiratory muscles
- Less commonly, weakness can be descending (starting in upper limbs or cranial muscles)
- Severity: ranges from mild (ambulatory) to near-total quadriplegia
- Areflexia/hyporeflexia: The invariable hallmark; may be absent very early
- Respiratory failure in 9%-30% of hospitalized patients (requiring mechanical ventilation)
Cranial Nerve Involvement (45%-75% of cases)
- Bilateral facial palsy: Most common cranial nerve finding (>50%)
- Extraocular muscle weakness (less common)
- Lower cranial nerve involvement: dysphagia, dysarthria
- Rare: facial myokymia, pseudotumor cerebri with papilledema
Sensory Features
- Sensory loss is NOT a prominent feature
- Usually limited to distal impairment of vibration sense
- Pain (moderate to severe): extremities, interscapular area, or back - occurs in ~70% during acute phase; may persist for a year in one-third
- Dysesthetic pain (burning/tingling) is less common
Autonomic Dysfunction (~65% of hospitalized patients)
-
Orthostatic hypotension
-
Urinary retention
-
Gastrointestinal atony
-
Episodic or sustained hypertension
-
Sinus tachycardia, tachyarrhythmias
-
Anhidrosis or episodic diaphoresis
-
Acral vasoconstriction
-
Sudden cardiac arrest (from excessive vagal activity)
-
Bradley and Daroff's Neurology in Clinical Practice, p. 2663-2664
7. Diagnostic Criteria
Required Features
- Progressive weakness of both legs and arms (more than one limb)
- Areflexia or hyporeflexia
Clinical Features Supportive of Diagnosis
- Progression over days to 4 weeks
- Relative symmetry of symptoms
- Mild sensory symptoms
- Bifacial palsies
- Autonomic dysfunction
- Absence of fever at onset
- Recovery beginning 2-4 weeks after progression ceases
- Muscle or radicular back/limb pain
Features that Argue Against Diagnosis
- Persistent asymmetry
- Bladder/bowel dysfunction at onset (not later)
- CSF pleocytosis >50 cells/mm³
- Sharp sensory level
8. Investigations
Cerebrospinal Fluid (CSF) - "Albuminocytological Dissociation"
- Protein: Elevated (>45 mg/dL) - due to altered permeability of microvasculature in inflamed spinal roots
- WBC: <10 cells/mm³ (typically mononuclear) - inflammatory cells remain confined to the roots and do not enter CSF
- This combination of high protein + low cell count is the classic CSF finding
- If WBC >100 cells/mm³, consider: HIV, Lyme disease, syphilis, sarcoidosis, TB meningitis, leukemic infiltration
Electrodiagnostic Studies (EMG/NCS)
- AIDP: Reduced conduction velocities, prolonged distal latencies, conduction blocks - features of demyelination
- AMAN/AMSAN: Reduced compound muscle action potential amplitudes with relatively preserved conduction velocities - features of axonal injury
- Nerve conduction velocities are slowed due to multifocal myelin destruction
MRI
- Enhancement of affected nerve roots (used to rule out alternative diagnoses, not primary diagnostic)
Nerve Biopsy
- Mononuclear inflammatory infiltrate
- Segmental demyelination and remyelination
Serum Antibodies
-
Anti-GQ1b antibodies: Highly specific for Miller-Fisher syndrome
-
Anti-GM1, anti-GD1a: Associated with AMAN
-
Tintinalli's Emergency Medicine, p. 1201-1202; Robbins, Cotran & Kumar, p. 1127
9. Treatment
Step 1: Respiratory Monitoring (Most Critical)
- Vital capacity (VC) <15 mL/kg (normal: 60-70 mL/kg)
- Declining one-breath count (unable to count 1-25 on single breath)
- PaO₂ <70 mm Hg on room air
- Bulbar dysfunction (difficulty breathing, swallowing, or speech)
- Aspiration
Warning: Avoid succinylcholine (depolarizing neuromuscular blocker) for intubation - risk of severe hyperkalemic response due to upregulated acetylcholine receptors in denervated muscle. Use non-depolarizing agents instead.
Step 2: Immunotherapy (Two Equivalent Options)
| Treatment | Mechanism | Notes |
|---|---|---|
| Intravenous Immunoglobulin (IVIg) | Suppresses immune response, neutralizes pathogenic antibodies | More widely available, easier to administer; adverse effects: thromboembolism, aseptic meningitis |
| Plasma Exchange (Plasmapheresis) | Removes circulating pathogenic antibodies directly | Adverse effects: hemodynamic instability, small increase in relapse rate; full recovery still more likely |
- Neither is superior to the other
- Combining both offers no additional benefit
- Corticosteroids: NOT beneficial and may be harmful - should NOT be used
Step 3: Supportive Care
- Cardiovascular monitoring (for autonomic instability)
- DVT prophylaxis
- Nutritional support
- Physical and occupational therapy
- Pain management
ICU Admission Criteria
- Inability to stand
- Inability to lift the head
- Inability to lift the elbows
- Insufficient cough
- Time from onset to hospital admission <7 days
- Elevated liver enzymes
- Tintinalli's Emergency Medicine, p. 1202
10. Prognosis
| Outcome | Percentage |
|---|---|
| Full or near-full recovery | ~80% |
| Mortality (respiratory paralysis, autonomic instability, cardiac arrest) | 2%-5% |
| Long-term disability at follow-up | Up to 20% of hospitalized survivors |
| Relapse rate | ~3% (higher with plasma exchange) |
- Recovery can take weeks to over a year
- AMAN may have faster or slower recovery than AIDP depending on severity
- AMSAN has the worst prognosis among subtypes
- Age, rapid progression, and need for ventilation are poor prognostic factors
11. Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Myasthenia gravis | Fatigability, no sensory involvement, normal reflexes early |
| Transverse myelitis | Spinal cord level, early bladder/bowel involvement, MRI cord lesion |
| Botulism | Descending paralysis, dilated fixed pupils, food/wound history |
| Critical illness polyneuropathy | ICU setting, preceded by critical illness |
| Acute HIV neuropathy | Risk factors, + serology |
| Tick paralysis | Ascending paralysis, but tick found |
| Hypokalemic periodic paralysis | Low K⁺, episodic, no sensory signs |
| Diphtheria | Palatal palsy first, diphtheria membrane |
| Poliomyelitis | Fever, CSF pleocytosis, no sensory symptoms, asymmetric |
| Lyme neuroborreliosis | Tick exposure, erythema migrans, facial palsy |
12. Distinction from CIDP
| Feature | GBS | CIDP |
|---|---|---|
| Time course | Acute (nadir in ≤4 weeks) | Chronic (progresses >2 months) |
| Sensory involvement | Minor | Prominent mixed sensorimotor |
| Course | Monophasic | Relapsing-remitting or progressive |
| Treatment | IVIg or plasma exchange (acute) | IVIg, steroids, plasma exchange (ongoing) |
| Associated conditions | Preceded by infection | Paraproteinemias, lymphoid neoplasms, HIV |
13. Recent Evidence (2023-2026)
- Ascending weakness + Areflexia = core features
- Immune mediated (T-cell + antibody)
- Demyelinating (classic AIDP) or Axonal (AMAN, AMSAN)
- Preceded by infection (C. jejuni, CMV, EBV, Zika, SARS-CoV-2)
Create a clinical summary document on GBS for quick reference
mkdir -p /home/daytona/workspace/gbs-clinical-summary && ls /home/daytona/worksp…
~/gbs-clinical-summary/create_gbs_doc.js
const {
Document, Packer, Paragraph, TextRun, Table, TableRow, TableCell,
HeadingLevel, AlignmentType, BorderStyle, WidthType, ShadingType,
VerticalAlign, PageNumber, Footer, Header, TabStopType, TabStopPosition,
UnderlineType
} = require('docx');
const fs = require('fs');
// ── Color palette ──────────────────────────────────────────────
const NAVY = "1A3A6B";
const TEAL = "006B6B";
const RED = "C0392B";
const LIGHT_BLUE_BG = "D6E4F0";
const LIGHT_GREEN_BG = "D5F5E3";
const LIGHT_RED_BG = "FADBD8";
const LIGHT_YELLOW_BG = "FEF9E7";
const LIGHT_GRAY_BG = "F2F3F4";
const WHITE = "FFFFFF";
const DARK = "1C1C1C";
const MID = "555555";
// ── Helper: section heading paragraph ─────────────────────────
function sectionHeading(text, color = NAVY) {
return new Paragraph({
spacing: { before: 260, after: 80 },
border: { bottom: { style: BorderStyle.SINGLE, size: 8, color: color, space: 4 } },
children: [
new TextRun({
text,
bold: true,
size: 26,
color,
font: "Calibri",
}),
],
});
}
// ── Helper: sub-heading ────────────────────────────────────────
function subHeading(text, color = TEAL) {
return new Paragraph({
spacing: { before: 180, after: 60 },
children: [
new TextRun({
text,
bold: true,
size: 22,
color,
font: "Calibri",
}),
],
});
}
// ── Helper: body paragraph ────────────────────────────────────
function body(text, { bold = false, color = DARK, indent = false } = {}) {
return new Paragraph({
indent: indent ? { left: 360 } : undefined,
spacing: { before: 40, after: 40 },
children: [
new TextRun({ text, bold, size: 19, color, font: "Calibri" }),
],
});
}
// ── Helper: bullet ────────────────────────────────────────────
function bullet(text, level = 0) {
return new Paragraph({
bullet: { level },
spacing: { before: 30, after: 30 },
indent: { left: 360 + level * 240, hanging: 240 },
children: [
new TextRun({ text, size: 19, color: DARK, font: "Calibri" }),
],
});
}
// ── Helper: colored alert box (simulate with shaded paragraph) ──
function alertBox(label, text, bgColor, labelColor = RED) {
return new Paragraph({
spacing: { before: 100, after: 100 },
shading: { type: ShadingType.CLEAR, fill: bgColor },
border: {
left: { style: BorderStyle.SINGLE, size: 16, color: labelColor, space: 8 },
},
indent: { left: 240 },
children: [
new TextRun({ text: label + " ", bold: true, size: 19, color: labelColor, font: "Calibri" }),
new TextRun({ text, size: 19, color: DARK, font: "Calibri" }),
],
});
}
// ── Helper: table cell (shaded header) ───────────────────────
function headerCell(text, bgColor = NAVY, textColor = WHITE) {
return new TableCell({
shading: { type: ShadingType.CLEAR, fill: bgColor },
verticalAlign: VerticalAlign.CENTER,
margins: { top: 80, bottom: 80, left: 120, right: 120 },
children: [
new Paragraph({
alignment: AlignmentType.CENTER,
children: [new TextRun({ text, bold: true, size: 19, color: textColor, font: "Calibri" })],
}),
],
});
}
function dataCell(text, bgColor = WHITE, bold = false, textColor = DARK) {
return new TableCell({
shading: { type: ShadingType.CLEAR, fill: bgColor },
verticalAlign: VerticalAlign.CENTER,
margins: { top: 60, bottom: 60, left: 120, right: 120 },
children: [
new Paragraph({
children: [new TextRun({ text, bold, size: 18, color: textColor, font: "Calibri" })],
}),
],
});
}
// ══════════════════════════════════════════════════════════════
// DOCUMENT CONTENT
// ══════════════════════════════════════════════════════════════
const children = [];
// ── TITLE BLOCK ───────────────────────────────────────────────
children.push(
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 40 },
shading: { type: ShadingType.CLEAR, fill: NAVY },
children: [
new TextRun({ text: "GUILLAIN-BARRÉ SYNDROME", bold: true, size: 40, color: WHITE, font: "Calibri" }),
],
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 20 },
shading: { type: ShadingType.CLEAR, fill: NAVY },
children: [
new TextRun({ text: "Clinical Quick Reference", size: 24, color: "A8D8EA", font: "Calibri", italics: true }),
],
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 200 },
shading: { type: ShadingType.CLEAR, fill: NAVY },
children: [
new TextRun({ text: "Last reviewed: July 2026 • Sources: Bradley & Daroff Neurology | Robbins Pathology | Tintinalli EM", size: 16, color: "BFC9CA", font: "Calibri" }),
],
})
);
// ─────────────────────────────────────────────────────────────
// 1. DEFINITION & EPIDEMIOLOGY
// ─────────────────────────────────────────────────────────────
children.push(sectionHeading("1. DEFINITION & EPIDEMIOLOGY"));
children.push(
body("Guillain-Barré syndrome (GBS) is an acute immune-mediated polyradiculoneuropathy — an inflammatory attack on peripheral nerves and spinal nerve roots causing rapidly progressive weakness, areflexia, and variable sensory loss."),
body("Most common cause of acute flaccid paralysis in the developed world. Also known as AIDP (Acute Inflammatory Demyelinating Polyradiculoneuropathy) in its classic form.", { bold: false }),
);
// Epi table
children.push(
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [
new TableRow({ children: [headerCell("Parameter"), headerCell("Value")] }),
new TableRow({ children: [dataCell("Annual incidence"), dataCell("1–2 per 100,000")] }),
new TableRow({ children: [dataCell("Sex ratio", LIGHT_GRAY_BG), dataCell("Male > Female (1.5:1)", LIGHT_GRAY_BG)] }),
new TableRow({ children: [dataCell("Age <18 yrs"), dataCell("~0.8 per 100,000")] }),
new TableRow({ children: [dataCell("Age >60 yrs", LIGHT_GRAY_BG), dataCell("~3.2 per 100,000", LIGHT_GRAY_BG)] }),
new TableRow({ children: [dataCell("Mortality (modern care)"), dataCell("1%–5%")] }),
new TableRow({ children: [dataCell("Long-term disability", LIGHT_GRAY_BG), dataCell("Up to 20% of hospitalized survivors", LIGHT_GRAY_BG)] }),
new TableRow({ children: [dataCell("Ventilation required"), dataCell("9%–30% of hospitalized patients")] }),
],
})
);
// ─────────────────────────────────────────────────────────────
// 2. PATHOPHYSIOLOGY
// ─────────────────────────────────────────────────────────────
children.push(sectionHeading("2. PATHOPHYSIOLOGY"));
children.push(
body("Trigger — Molecular Mimicry:", { bold: true }),
body("~2/3 of cases are preceded by infection 1–4 weeks prior. Microbial antigens (especially C. jejuni capsular antigens) share structural similarity with peripheral nerve gangliosides (GM1, GD1b). Antibodies formed against the pathogen cross-react with nerve components."),
body("Immune mechanisms (dual):", { bold: true }),
bullet("T cell-mediated: Sensitized T cells direct macrophages to invade endoneurium and strip myelin from axons (reproducible in animal models)"),
bullet("Antibody-mediated (humoral): IgG/IgM antibodies bind nerve antigens → classical complement pathway activation → macrophage processes penetrate Schwann cell basement membrane at nodes of Ranvier → myelin lamellae are physically stripped and engulfed"),
);
children.push(subHeading("Common Triggers"));
children.push(
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [
new TableRow({ children: [headerCell("Organism / Agent"), headerCell("Notes")] }),
new TableRow({ children: [dataCell("Campylobacter jejuni", LIGHT_BLUE_BG, true), dataCell("Strongest association; linked to axonal AMAN subtype", LIGHT_BLUE_BG)] }),
new TableRow({ children: [dataCell("Epstein-Barr Virus"), dataCell("Common trigger")] }),
new TableRow({ children: [dataCell("Cytomegalovirus (CMV)", LIGHT_GRAY_BG), dataCell("Common trigger", LIGHT_GRAY_BG)] }),
new TableRow({ children: [dataCell("Mycoplasma pneumoniae"), dataCell("Upper respiratory illness")] }),
new TableRow({ children: [dataCell("Zika Virus", LIGHT_GRAY_BG), dataCell("Epidemiologically significant", LIGHT_GRAY_BG)] }),
new TableRow({ children: [dataCell("SARS-CoV-2 / HIV"), dataCell("Reported associations")] }),
new TableRow({ children: [dataCell("Vaccines (rare)", LIGHT_YELLOW_BG), dataCell("Influenza, VZV, non-mRNA COVID vaccines — rare association", LIGHT_YELLOW_BG)] }),
],
})
);
// ─────────────────────────────────────────────────────────────
// 3. SUBTYPES & VARIANTS
// ─────────────────────────────────────────────────────────────
children.push(sectionHeading("3. SUBTYPES & VARIANTS"));
children.push(subHeading("Common Subtypes"));
children.push(
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [
new TableRow({ children: [headerCell("Subtype"), headerCell("Pathology"), headerCell("Key Features")] }),
new TableRow({ children: [
dataCell("AIDP", LIGHT_BLUE_BG, true),
dataCell("Demyelinating", LIGHT_BLUE_BG),
dataCell("Classic form; most common in Europe/North America", LIGHT_BLUE_BG),
]}),
new TableRow({ children: [
dataCell("AMAN", WHITE, true),
dataCell("Axonal (motor only)"),
dataCell("Pure motor paralysis, sensory intact; summer epidemics in China; C. jejuni association"),
]}),
new TableRow({ children: [
dataCell("AMSAN", LIGHT_RED_BG, true),
dataCell("Axonal (motor + sensory)", LIGHT_RED_BG),
dataCell("Severe; poorest prognosis", LIGHT_RED_BG),
]}),
],
})
);
children.push(subHeading("Rare Variants"));
children.push(
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [
new TableRow({ children: [headerCell("Variant"), headerCell("Cardinal Features")] }),
new TableRow({ children: [dataCell("Miller-Fisher Syndrome", LIGHT_YELLOW_BG, true), dataCell("Ophthalmoplegia + Ataxia + Areflexia (triad); anti-GQ1b antibodies; 6% of GBS in West", LIGHT_YELLOW_BG)] }),
new TableRow({ children: [dataCell("Pharyngeal-Cervical-Brachial"), dataCell("Weakness of pharyngeal, cervical, brachial muscles")] }),
new TableRow({ children: [dataCell("Facial Diplegia with Paresthesias", LIGHT_GRAY_BG), dataCell("Bilateral facial palsy", LIGHT_GRAY_BG)] }),
new TableRow({ children: [dataCell("Acute Pandysautonomia"), dataCell("Severe autonomic dysfunction")] }),
new TableRow({ children: [dataCell("Paraparetic Variant", LIGHT_GRAY_BG), dataCell("Predominantly lower limb weakness", LIGHT_GRAY_BG)] }),
],
})
);
// ─────────────────────────────────────────────────────────────
// 4. CLINICAL FEATURES
// ─────────────────────────────────────────────────────────────
children.push(sectionHeading("4. CLINICAL FEATURES"));
children.push(subHeading("Symptom Timeline"));
children.push(
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [
new TableRow({ children: [headerCell("Phase"), headerCell("Timing"), headerCell("Description")] }),
new TableRow({ children: [dataCell("Antecedent Event", LIGHT_BLUE_BG), dataCell("1–4 weeks before", LIGHT_BLUE_BG), dataCell("Infection / vaccination", LIGHT_BLUE_BG)] }),
new TableRow({ children: [dataCell("Onset"), dataCell("Day 0"), dataCell("Weakness ± paresthesias (often distal hands/fingers)")] }),
new TableRow({ children: [dataCell("Progression", LIGHT_GRAY_BG), dataCell("Days to 4 weeks", LIGHT_GRAY_BG), dataCell("Ascending paralysis; most reach nadir in <2 weeks", LIGHT_GRAY_BG)] }),
new TableRow({ children: [dataCell("Plateau"), dataCell("~Week 2–4"), dataCell("Maximum weakness; respiratory risk highest here")] }),
new TableRow({ children: [dataCell("Recovery", LIGHT_GREEN_BG), dataCell("Weeks to 1 year", LIGHT_GREEN_BG), dataCell("Begins 2–4 weeks after progression stops", LIGHT_GREEN_BG)] }),
],
})
);
children.push(subHeading("Motor"));
children.push(
bullet("Ascending, fairly symmetric weakness — lower limbs → upper limbs → cranial/oropharyngeal → respiratory muscles"),
bullet("Areflexia / hyporeflexia — invariable hallmark; may be absent very early"),
bullet("Cranial nerve involvement in 45%–75%: bilateral facial palsy (>50%), extraocular weakness, dysphagia, dysarthria"),
bullet("Respiratory failure in 9%–30%; risk ↑ with age"),
);
children.push(subHeading("Sensory"));
children.push(
bullet("NOT a prominent feature — mostly distal vibration loss"),
bullet("Pain (moderate–severe) in ~70% during acute phase — extremities, interscapular, back; may persist 1 year"),
bullet("Dysesthetic pain (burning/tingling) less common"),
);
children.push(subHeading("Autonomic (~65% of hospitalized patients)"));
children.push(
bullet("Orthostatic hypotension, urinary retention, GI atony"),
bullet("Sinus tachycardia, tachyarrhythmias, episodic hypertension"),
bullet("Anhidrosis or episodic diaphoresis, acral vasoconstriction"),
alertBox("⚠ WARNING:", "Sudden cardiac arrest may occur from excessive vagal activity. Continuous cardiac monitoring is mandatory.", LIGHT_RED_BG, RED),
);
// ─────────────────────────────────────────────────────────────
// 5. DIAGNOSTIC CRITERIA
// ─────────────────────────────────────────────────────────────
children.push(sectionHeading("5. DIAGNOSTIC CRITERIA"));
children.push(
alertBox("REQUIRED:", "1) Progressive weakness of both legs AND arms (>1 limb) 2) Areflexia or hyporeflexia", LIGHT_BLUE_BG, NAVY),
);
children.push(subHeading("Supportive Clinical Features"));
children.push(
bullet("Progression over days to 4 weeks"),
bullet("Relative symmetry of symptoms"),
bullet("Mild sensory symptoms or signs"),
bullet("Bifacial palsies"),
bullet("Autonomic dysfunction"),
bullet("Absence of fever at onset"),
bullet("Recovery beginning 2–4 weeks after progression ceases"),
);
children.push(subHeading("Features Against Diagnosis"));
children.push(
bullet("Persistent marked asymmetry"),
bullet("Bladder/bowel dysfunction at onset (not later)"),
bullet("CSF pleocytosis >50 cells/mm³"),
bullet("Sharp sensory level (suggests cord lesion)"),
);
// ─────────────────────────────────────────────────────────────
// 6. INVESTIGATIONS
// ─────────────────────────────────────────────────────────────
children.push(sectionHeading("6. INVESTIGATIONS"));
children.push(subHeading("CSF Analysis — Albuminocytological Dissociation (Classic Finding)"));
children.push(
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [
new TableRow({ children: [headerCell("Parameter"), headerCell("Typical GBS Finding"), headerCell("Significance")] }),
new TableRow({ children: [
dataCell("Protein", LIGHT_YELLOW_BG, true),
dataCell(">45 mg/dL (often 100–1000 mg/dL)", LIGHT_YELLOW_BG),
dataCell("Inflamed root microvasculature → protein leaks", LIGHT_YELLOW_BG),
]}),
new TableRow({ children: [
dataCell("WBC", WHITE, true),
dataCell("<10 cells/mm³ (mononuclear)"),
dataCell("Cells confined to roots, do not enter CSF"),
]}),
],
})
);
children.push(
alertBox("NOTE:", "If WBC >100/mm³, consider: HIV, Lyme, syphilis, sarcoidosis, TB/bacterial meningitis, leukemic infiltration.", LIGHT_YELLOW_BG, TEAL),
);
children.push(subHeading("Electrodiagnostic Studies (EMG/NCS)"));
children.push(
bullet("AIDP: Reduced conduction velocities, prolonged distal latencies, conduction blocks (demyelination pattern)"),
bullet("AMAN/AMSAN: Reduced CMAP amplitudes, relatively preserved conduction velocities (axonal pattern)"),
);
children.push(subHeading("Other Tests"));
children.push(
bullet("MRI: Nerve root enhancement (rules out spinal cord pathology)"),
bullet("Serology: Anti-GQ1b (Miller-Fisher), Anti-GM1/GD1a (AMAN)"),
bullet("Nerve biopsy: Mononuclear infiltrate, segmental demyelination and remyelination"),
);
// ─────────────────────────────────────────────────────────────
// 7. TREATMENT
// ─────────────────────────────────────────────────────────────
children.push(sectionHeading("7. TREATMENT"));
children.push(alertBox("⚠ STEROIDS:", "Corticosteroids are NOT beneficial and may be HARMFUL. Do NOT use.", LIGHT_RED_BG, RED));
children.push(subHeading("Step 1 — Respiratory Monitoring (Priority #1)"));
children.push(
body("Monitor vital capacity (VC). Respiratory failure can occur without dyspnea symptoms — proactive monitoring is essential."),
);
children.push(
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [
new TableRow({ children: [headerCell("Intubation Indications", RED), headerCell("ICU Admission Criteria (≥4 of:", NAVY)] }),
new TableRow({ children: [
dataCell("VC < 15 mL/kg\nPaO₂ < 70 mmHg on room air\nBulbar dysfunction (breathing, swallowing, speech)\nAspiration\nDeclining one-breath count (cannot count 1–25)"),
dataCell("Cannot stand / lift head / lift elbows\nInsufficient cough\nOnset to admission <7 days\nElevated liver enzymes\nVC < 20 mL/kg\nNIF < −30 cmH₂O\n>30% decline in VC or NIF"),
]}),
],
})
);
children.push(
alertBox("⚠ INTUBATION:", "Avoid SUCCINYLCHOLINE (depolarizing NMB) — risk of severe HYPERKALEMIA due to upregulated acetylcholine receptors in denervated muscle. Use non-depolarizing agents instead.", LIGHT_RED_BG, RED),
);
children.push(subHeading("Step 2 — Immunotherapy"));
children.push(
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [
new TableRow({ children: [headerCell("Treatment"), headerCell("Mechanism"), headerCell("Adverse Effects"), headerCell("Notes")] }),
new TableRow({ children: [
dataCell("IVIg (IV Immunoglobulin)", LIGHT_BLUE_BG, true),
dataCell("Suppresses immune response; neutralizes pathogenic antibodies", LIGHT_BLUE_BG),
dataCell("Thromboembolism, aseptic meningitis", LIGHT_BLUE_BG),
dataCell("More widely available; easier to administer", LIGHT_BLUE_BG),
]}),
new TableRow({ children: [
dataCell("Plasma Exchange (Plasmapheresis)", WHITE, true),
dataCell("Directly removes circulating pathogenic antibodies"),
dataCell("Hemodynamic instability, small ↑ relapse rate"),
dataCell("Equally effective; full recovery still more likely"),
]}),
],
})
);
children.push(
bullet("Neither IVIg nor plasma exchange is superior to the other"),
bullet("Combining both offers NO additional benefit"),
);
children.push(subHeading("Step 3 — Supportive Care"));
children.push(
bullet("Continuous cardiac monitoring (autonomic instability)"),
bullet("DVT prophylaxis (immobilized patients)"),
bullet("Nutritional support (NG/PEG if bulbar dysfunction)"),
bullet("Pain management (neuropathic pain agents: gabapentin, carbamazepine)"),
bullet("Physical and occupational therapy — start early"),
bullet("Psychological support (prolonged paralysis is psychologically devastating)"),
);
// ─────────────────────────────────────────────────────────────
// 8. PROGNOSIS
// ─────────────────────────────────────────────────────────────
children.push(sectionHeading("8. PROGNOSIS"));
children.push(
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [
new TableRow({ children: [headerCell("Outcome"), headerCell("Rate")] }),
new TableRow({ children: [dataCell("Full/near-full recovery", LIGHT_GREEN_BG, true), dataCell("~80%", LIGHT_GREEN_BG)] }),
new TableRow({ children: [dataCell("Mortality (respiratory failure, autonomic instability, cardiac arrest)"), dataCell("2%–5%")] }),
new TableRow({ children: [dataCell("Long-term disability (hospitalized survivors)", LIGHT_YELLOW_BG), dataCell("Up to 20%", LIGHT_YELLOW_BG)] }),
new TableRow({ children: [dataCell("Relapse rate"), dataCell("~3%")] }),
],
})
);
children.push(subHeading("Poor Prognostic Factors"));
children.push(
bullet("Older age"),
bullet("Rapid progression to nadir"),
bullet("Need for mechanical ventilation"),
bullet("AMSAN subtype"),
bullet("Very low CMAP amplitudes on NCS"),
bullet("Preceding C. jejuni infection"),
);
// ─────────────────────────────────────────────────────────────
// 9. DIFFERENTIAL DIAGNOSIS
// ─────────────────────────────────────────────────────────────
children.push(sectionHeading("9. DIFFERENTIAL DIAGNOSIS"));
children.push(
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [
new TableRow({ children: [headerCell("Condition"), headerCell("Distinguishing Feature")] }),
new TableRow({ children: [dataCell("Myasthenia Gravis"), dataCell("Fatigability, normal reflexes early, ptosis/diplopia, anti-AChR antibodies")] }),
new TableRow({ children: [dataCell("Transverse Myelitis", LIGHT_GRAY_BG), dataCell("Spinal level, early bladder/bowel, MRI cord lesion", LIGHT_GRAY_BG)] }),
new TableRow({ children: [dataCell("Botulism"), dataCell("Descending paralysis, dilated fixed pupils, food/wound exposure, no sensory loss")] }),
new TableRow({ children: [dataCell("Tick Paralysis", LIGHT_GRAY_BG), dataCell("Ascending paralysis — but tick found on scalp", LIGHT_GRAY_BG)] }),
new TableRow({ children: [dataCell("Poliomyelitis"), dataCell("Fever, CSF pleocytosis, asymmetric weakness, no sensory symptoms")] }),
new TableRow({ children: [dataCell("Hypokalemic Periodic Paralysis", LIGHT_GRAY_BG), dataCell("Low K⁺, episodic, no sensory signs", LIGHT_GRAY_BG)] }),
new TableRow({ children: [dataCell("Lyme Neuroborreliosis"), dataCell("Tick exposure, erythema migrans history, facial palsy, positive serology")] }),
new TableRow({ children: [dataCell("Critical Illness Polyneuropathy", LIGHT_GRAY_BG), dataCell("ICU setting, preceded by sepsis/MODS", LIGHT_GRAY_BG)] }),
new TableRow({ children: [dataCell("Diphtheria"), dataCell("Palatal palsy first, pharyngeal membrane, history of incomplete vaccination")] }),
],
})
);
// ─────────────────────────────────────────────────────────────
// 10. GBS vs CIDP
// ─────────────────────────────────────────────────────────────
children.push(sectionHeading("10. GBS vs CIDP — Key Differences"));
children.push(
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [
new TableRow({ children: [headerCell("Feature"), headerCell("GBS (Acute)"), headerCell("CIDP (Chronic)")] }),
new TableRow({ children: [dataCell("Time course"), dataCell("Nadir ≤4 weeks"), dataCell("Progresses >2 months")] }),
new TableRow({ children: [dataCell("Course", LIGHT_GRAY_BG), dataCell("Monophasic", LIGHT_GRAY_BG), dataCell("Relapsing-remitting or progressive", LIGHT_GRAY_BG)] }),
new TableRow({ children: [dataCell("Sensory involvement"), dataCell("Minor"), dataCell("Prominent mixed sensorimotor")] }),
new TableRow({ children: [dataCell("Associations", LIGHT_GRAY_BG), dataCell("Preceding infection", LIGHT_GRAY_BG), dataCell("Paraproteinemia, lymphoma, HIV", LIGHT_GRAY_BG)] }),
new TableRow({ children: [dataCell("Steroids"), dataCell("NOT effective — may harm"), dataCell("Effective (ongoing)")] }),
],
})
);
// ─────────────────────────────────────────────────────────────
// 11. QUICK REFERENCE MNEMONICS
// ─────────────────────────────────────────────────────────────
children.push(sectionHeading("11. QUICK REFERENCE MNEMONICS"));
children.push(
new Paragraph({
spacing: { before: 80, after: 60 },
shading: { type: ShadingType.CLEAR, fill: LIGHT_BLUE_BG },
border: { left: { style: BorderStyle.SINGLE, size: 16, color: NAVY, space: 8 } },
indent: { left: 240 },
children: [
new TextRun({ text: "GBS CORE FEATURES: ", bold: true, size: 20, color: NAVY, font: "Calibri" }),
new TextRun({ text: "Ascending weakness + Areflexia = GBS until proven otherwise", size: 20, color: DARK, font: "Calibri" }),
],
}),
new Paragraph({
spacing: { before: 60, after: 60 },
shading: { type: ShadingType.CLEAR, fill: LIGHT_GREEN_BG },
border: { left: { style: BorderStyle.SINGLE, size: 16, color: TEAL, space: 8 } },
indent: { left: 240 },
children: [
new TextRun({ text: "TREATMENT: ", bold: true, size: 20, color: TEAL, font: "Calibri" }),
new TextRun({ text: "IVIg OR Plasma Exchange + Supportive care. NEVER steroids.", size: 20, color: DARK, font: "Calibri" }),
],
}),
new Paragraph({
spacing: { before: 60, after: 60 },
shading: { type: ShadingType.CLEAR, fill: LIGHT_RED_BG },
border: { left: { style: BorderStyle.SINGLE, size: 16, color: RED, space: 8 } },
indent: { left: 240 },
children: [
new TextRun({ text: "DANGER: ", bold: true, size: 20, color: RED, font: "Calibri" }),
new TextRun({ text: "Avoid succinylcholine for intubation (hyperkalemia risk). Monitor VC. Watch for autonomic storms.", size: 20, color: DARK, font: "Calibri" }),
],
}),
new Paragraph({
spacing: { before: 60, after: 60 },
shading: { type: ShadingType.CLEAR, fill: LIGHT_YELLOW_BG },
border: { left: { style: BorderStyle.SINGLE, size: 16, color: "#B7950B", space: 8 } },
indent: { left: 240 },
children: [
new TextRun({ text: "CSF: ", bold: true, size: 20, color: "#B7950B", font: "Calibri" }),
new TextRun({ text: "High protein + Low cells = Albuminocytological dissociation (classic GBS pattern)", size: 20, color: DARK, font: "Calibri" }),
],
}),
new Paragraph({
spacing: { before: 60, after: 80 },
shading: { type: ShadingType.CLEAR, fill: LIGHT_GRAY_BG },
border: { left: { style: BorderStyle.SINGLE, size: 16, color: MID, space: 8 } },
indent: { left: 240 },
children: [
new TextRun({ text: "MILLER-FISHER: ", bold: true, size: 20, color: MID, font: "Calibri" }),
new TextRun({ text: "OAA = Ophthalmoplegia + Ataxia + Areflexia. Anti-GQ1b antibodies.", size: 20, color: DARK, font: "Calibri" }),
],
}),
);
// ─────────────────────────────────────────────────────────────
// FOOTER NOTE
// ─────────────────────────────────────────────────────────────
children.push(
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 200, after: 40 },
border: { top: { style: BorderStyle.SINGLE, size: 4, color: "AAAAAA", space: 8 } },
children: [
new TextRun({ text: "Sources: Bradley & Daroff's Neurology in Clinical Practice | Robbins & Cotran Pathologic Basis of Disease | Robbins & Kumar Basic Pathology | Tintinalli's Emergency Medicine", size: 15, color: "888888", font: "Calibri", italics: true }),
],
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 0 },
children: [
new TextRun({ text: "EAN/PNS GBS Guideline 2023 (PMID: 37814552) | Bellanti & Rinaldi Comprehensive Review 2024 (PMID: 38813755)", size: 15, color: "888888", font: "Calibri", italics: true }),
],
}),
);
// ══════════════════════════════════════════════════════════════
// BUILD DOCUMENT
// ══════════════════════════════════════════════════════════════
const doc = new Document({
styles: {
default: {
document: {
run: { font: "Calibri", size: 20 },
},
},
},
sections: [
{
properties: {
page: {
margin: { top: 720, bottom: 720, left: 900, right: 900 },
},
},
footers: {
default: new Footer({
children: [
new Paragraph({
alignment: AlignmentType.CENTER,
children: [
new TextRun({ text: "GBS Clinical Quick Reference — Page ", size: 16, color: "888888", font: "Calibri" }),
new TextRun({ children: [PageNumber.CURRENT], size: 16, color: "888888", font: "Calibri" }),
new TextRun({ text: " of ", size: 16, color: "888888", font: "Calibri" }),
new TextRun({ children: [PageNumber.TOTAL_PAGES], size: 16, color: "888888", font: "Calibri" }),
],
}),
],
}),
},
children,
},
],
});
Packer.toBuffer(doc).then(buffer => {
fs.writeFileSync("/home/daytona/workspace/gbs-clinical-summary/GBS_Clinical_Quick_Reference.docx", buffer);
console.log("Document created successfully.");
});
cd /home/daytona/workspace/gbs-clinical-summary && node create_gbs_doc.js 2>&1
python3 /home/daytona/skills/docx/scripts/office/validate.py /home/daytona/works…
cd /home/daytona/workspace/gbs-clinical-summary && python3 -c " import zipfile, …
GBS Clinical Quick Reference
Word Document · DOCX
| # | Section | Highlights |
|---|---|---|
| 1 | Definition & Epidemiology | Incidence table, sex/age distribution, mortality rates |
| 2 | Pathophysiology | Molecular mimicry, dual immune mechanisms, trigger table (C. jejuni, EBV, CMV, Zika, SARS-CoV-2, vaccines) |
| 3 | Subtypes & Variants | AIDP / AMAN / AMSAN comparison table; Miller-Fisher and rare variants |
| 4 | Clinical Features | Symptom timeline table; motor, sensory, autonomic features |
| 5 | Diagnostic Criteria | Required vs supportive vs against-diagnosis features |
| 6 | Investigations | CSF albuminocytological dissociation, NCS/EMG patterns, serology |
| 7 | Treatment | Intubation criteria table, ICU criteria, IVIg vs plasma exchange comparison, succinylcholine warning, steroid warning |
| 8 | Prognosis | Outcomes table, poor prognostic factors |
| 9 | Differential Diagnosis | 10-condition comparison table |
| 10 | GBS vs CIDP | Side-by-side comparison |
| 11 | Quick Reference Mnemonics | Color-coded boxes for core features, treatment, dangers, CSF pattern, Miller-Fisher |
Create a visual flowchart for GBS diagnosis and management
A clean, professional clinical flowchart for Guillain-Barré Syndrome (GBS) diagnosis and management. White background, medical style. The flowchart flows top to bottom with color-coded boxes and arrows. TITLE at top: "GUILLAIN-BARRÉ SYNDROME: Diagnosis & Management Flowchart" in bold dark navy. STEP 1 - TRIGGER (light blue box): "Antecedent Event (1-4 weeks prior)" with sub-text: "Campylobacter jejuni | CMV | EBV | Mycoplasma | Zika | SARS-CoV-2 | Vaccination (rare)" Arrow pointing down. STEP 2 - PRESENTATION (light blue box): "Clinical Presentation" with bullet points: "• Ascending symmetric weakness (legs → arms → cranial)" "• Areflexia / Hyporeflexia (hallmark)" "• ± Sensory paresthesias" "• ± Autonomic dysfunction" "• ± Facial palsy (bilateral)" Arrow pointing down. STEP 3 - DIAGNOSTIC CRITERIA (navy box, white text): "Diagnostic Criteria REQUIRED:" "✓ Progressive weakness >1 limb" "✓ Areflexia / Hyporeflexia" Supportive: "Symmetry | Mild sensory signs | Cranial palsy | No fever at onset" Arrow splits into TWO paths labeled "INVESTIGATE": LEFT PATH - CSF Analysis (yellow box): "Lumbar Puncture" "↑ Protein (>45 mg/dL)" "↓ Cells (<10/mm³)" "= Albuminocytological Dissociation" RIGHT PATH - NCS/EMG (yellow box): "Nerve Conduction Studies" "AIDP: ↓ Conduction velocity" "AMAN: ↓ CMAP amplitude" "AMSAN: Severe axonal damage" Both paths merge with arrow down. STEP 4 - SUBTYPES (three colored boxes side by side): - GREEN box: "AIDP - Demyelinating - Most common West" - ORANGE box: "AMAN - Axonal/Motor - Common Asia" - RED box: "AMSAN - Axonal Motor+Sensory - Worst prognosis" Small box below: "Miller-Fisher Variant: Ophthalmoplegia + Ataxia + Areflexia (Anti-GQ1b +)" Arrow down labeled "MANAGEMENT" STEP 5 - IMMEDIATE (red bordered box): "⚠ RESPIRATORY MONITORING (Priority #1)" "Vital Capacity < 15 mL/kg → INTUBATE" "⚠ AVOID SUCCINYLCHOLINE → Hyperkalemia risk" "Admit to ICU if ≥4 risk criteria met" Arrow down. STEP 6 - TREATMENT (two green boxes side by side): LEFT: "IVIg 0.4 g/kg/day × 5 days" RIGHT: "Plasma Exchange 5 sessions" Center text below boxes: "EQUALLY EFFECTIVE — Do NOT combine — No additional benefit" Red warning box: "✗ NO STEROIDS — Not effective, may harm" Arrow down. STEP 7 - SUPPORTIVE CARE (light green box): "• Cardiac monitoring (autonomic storms)" "• DVT prophylaxis" "• Pain management (gabapentinoids)" "• Nutritional support" "• Physiotherapy" Arrow down. STEP 8 - PROGNOSIS (split into three colored outcome boxes): - Green: "~80% Full Recovery" - Yellow: "~20% Long-term Disability" - Red: "2-5% Mortality (respiratory/autonomic)" Clean arrows throughout, professional medical typography, well-spaced layout.
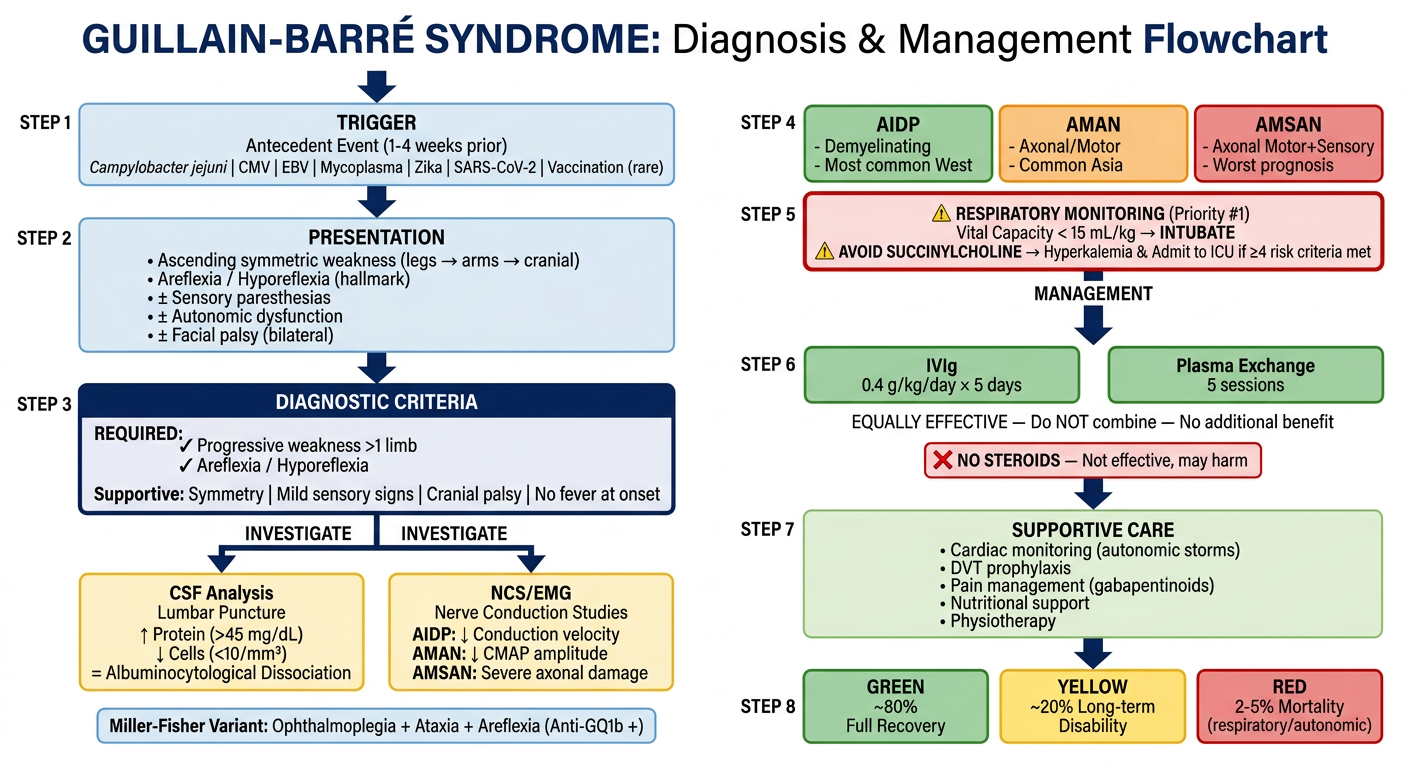
| Step | Content |
|---|---|
| 1. Trigger | Antecedent infections (C. jejuni, CMV, EBV, Zika, SARS-CoV-2, rare vaccines) |
| 2. Presentation | Ascending weakness, areflexia, ± sensory, ± autonomic, ± facial palsy |
| 3. Diagnosis | Required criteria + supportive features |
| 4. Investigations | CSF (albuminocytological dissociation) and NCS/EMG findings - branching paths |
| 5. Subtypes | AIDP / AMAN / AMSAN side by side, plus Miller-Fisher variant |
| 6. Immediate Action | Respiratory monitoring - VC threshold, succinylcholine warning, ICU criteria |
| 7. Treatment | IVIg vs Plasma Exchange (equally effective, not combined) + NO STEROIDS warning |
| 8. Prognosis | Three outcome branches: ~80% full recovery / ~20% disability / 2-5% mortality |