Stridor ENT topic
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative ENT and emergency medicine textbooks. Let me compile the full structured response.
Stridor - Comprehensive ENT Review
Definition
Stridor (from Latin stridulus - creaking, whistling, grating) is a harsh, high-pitched vibratory sound caused by partial obstruction or collapse of the airway, producing turbulent airflow through any portion of the upper airway from the nose to the trachea. It is distinct from:
- Stertor - low-pitched snoring sound from naso/oropharyngeal obstruction (pharyngeal level)
- Wheeze - high-pitched musical sound from small intrathoracic airways (asthma)
"Stridor is a high-pitched noise that can be mistaken for wheeze. Stridor arises from compromise of the airway at the level of the larynx and trachea." - Scott-Brown's Otorhinolaryngology
Anatomical Classification by Phase of Respiration
This is the most clinically useful classification:
| Phase | Anatomical Level | Mechanism | Examples |
|---|---|---|---|
| Inspiratory | At or above the glottis (supraglottis, glottis); extrathoracic | Extrathoracic airway collapses on inspiration | Epiglottitis, laryngomalacia, foreign body above glottis, croup |
| Expiratory | Intrathoracic airway, lower trachea | Expiratory compression of intrathoracic airway | Asthma, infective tracheobronchitis, lower foreign body |
| Biphasic | Subglottis, fixed lesions anywhere | Fixed obstruction with little change in airway dynamics through respiratory cycle | Subglottic stenosis, laryngeal web, bilateral vocal cord palsy, bacterial tracheitis |
Key principle: The extrathoracic airway collapses on inspiration (negative transmural pressure) and expands on expiration. The intrathoracic airway does the opposite. The subglottis/upper trachea, supported by cartilage, is largely immune to these pressure fluctuations - hence biphasic stridor.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2
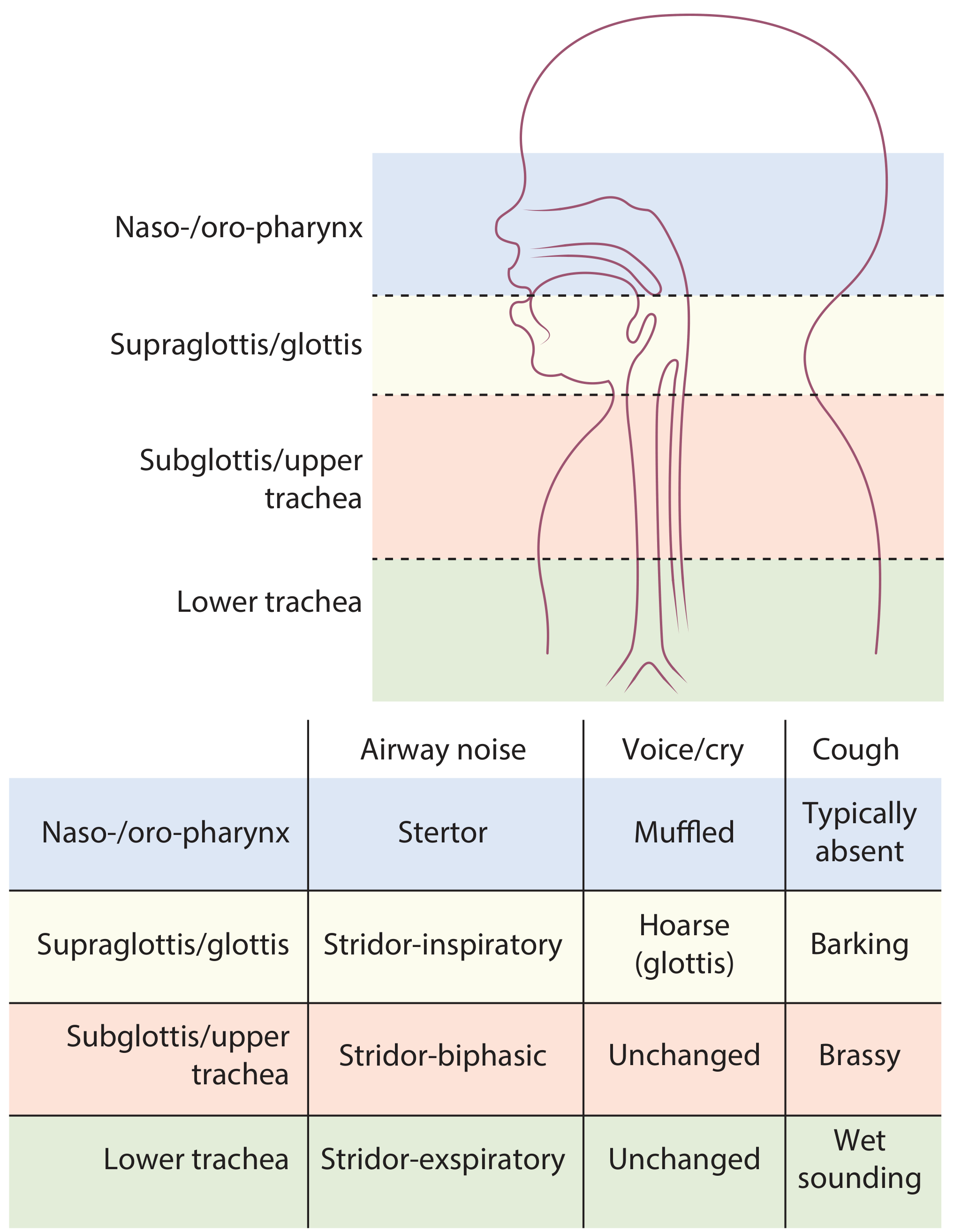
Voice/Cough Quality by Level
| Level | Airway Noise | Voice/Cry | Cough Quality |
|---|---|---|---|
| Naso-/oro-pharynx | Stertor | Muffled / "hot potato" | Typically absent |
| Supraglottis/glottis | Stridor - inspiratory | Hoarse (glottic) | Barking |
| Subglottis/upper trachea | Stridor - biphasic | Unchanged | Brassy |
| Lower trachea | Stridor - expiratory | Unchanged | Wet-sounding |
Causes of Stridor
Congenital (Paediatric)
| Cause | Notes |
|---|---|
| Laryngomalacia | Most common cause of infant stridor (60-75%). Inspiratory stridor, onset in first 2 weeks of life, omega-shaped epiglottis, resolves by 18 months in most |
| Vocal cord palsy | 2nd most common newborn stridor. Weak cry + inspiratory stridor. Causes: idiopathic, birth trauma, Arnold-Chiari malformation, cardiomegaly, PDA ligation |
| Subglottic stenosis | Biphasic stridor worsening with URTIs. History of intubation is key |
| Laryngeal web | Fixed biphasic stridor from birth |
| Subglottic haemangioma | Progressive inspiratory stridor, skin haemangioma in 50%, do NOT biopsy |
| Tracheomalacia | Expiratory stridor/wheeze, "dying spells" |
| Vascular ring | Stridor worse with feeding, from birth |
| Choanal atresia (bilateral) | Improves with crying (mouth open) |
Inflammatory/Infective (Acquired)
| Cause | Age | Stridor | Key Features |
|---|---|---|---|
| Croup (viral LTB) | 1-3 years | Loud, barking, inspiratory | Parainfluenza virus; 1-2 day coryza prodrome; low fever; responds to steroids + nebulized adrenaline |
| Epiglottitis | 2-7 years | Muffled, soft | H. influenzae type b; high fever; drooling; toxic, tripod position; ALL require intubation |
| Bacterial tracheitis | Any child | High-pitched, biphasic | S. aureus; high fever; >80% require intubation; purulent tracheal secretions |
| Peritonsillar abscess | Older children/adults | Sonorous, gurgling | "Hot potato" voice; uvula deviation |
| Retropharyngeal abscess | Young children | Inspiratory | Fever, neck stiffness, drooling |
| Angioneurotic oedema | Any | Inspiratory | Allergic (antihistamines + steroids + adrenaline) vs. hereditary (C1 esterase inhibitor deficiency) |
Adult Causes
- Laryngeal cancer - progressive hoarseness, then stridor
- Laryngeal papillomatosis - recurrent respiratory papillomatosis (HPV 6/11)
- Subglottic stenosis - post-intubation, post-radiation, Wegener's granulomatosis
- Foreign body aspiration - sudden onset; inspiratory if above glottis, expiratory/biphasic if lower
- Thyroid/mediastinal mass - extrinsic compression
- Bilateral vocal cord palsy - post-thyroid surgery
- Traumatic - laryngeal fracture, expanding neck haematoma
Croup vs. Epiglottitis - Key Comparison
| Feature | Croup | Epiglottitis |
|---|---|---|
| Age | 1-3 years | 2-7 years |
| Cause | Parainfluenza viruses | H. influenzae b (Hib) |
| Prodrome | 1-2 days of coryza | Hours; sore throat, dysphagia, drooling |
| Fever | <38°C | >38°C |
| Appearance | Lethargic | Pale, toxic; drooling; sitting with neck extended (tripod) |
| Stridor quality | Barking cough, loud stridor | Muffled stridor |
| Hypoxia | Unusual | Frequent |
| Intubation | <5% of hospitalized cases | ALL require intubation |
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1
Critical warning: If a child is stridulous and drooling, do NOT lay them down and do NOT attempt to examine the mouth - this can precipitate complete airway obstruction. - Bailey and Love's Surgery
Laryngomalacia - Detailed
- Most common cause of stridor in infancy
- Pathophysiology: Collapse of the supraglottic larynx on inspiration, related to neuromuscular hypotonia and dysfunction of the laryngeal adductor reflex (LAR), a vagally-mediated reflex
- Stridor character: Relatively low-pitched, worsens with feeding; in mild cases improves with crying (pharyngeal tone increases), but in severe cases worsens with crying due to increased airflow through the collapsed larynx
- Natural history: Median spontaneous resolution 7-9 months; vast majority resolve by 18 months
- Treatment: Observation for mild cases. Supraglottoplasty for severe cases (failure to thrive, apnoea, severe respiratory distress)
- Association: Gastro-oesophageal reflux (GER) is found in ~50% of cases of infantile stridor
- Cummings Otolaryngology
History Taking
Neonates/Infants:
- Onset - at birth (fixed congenital lesion) vs first weeks (laryngomalacia)?
- Aggravating factors: worse with feeding (vascular ring, TOF), worse with crying (laryngomalacia), better with crying (choanal atresia)
- Abnormal cry: suggests vocal cord palsy
- Prematurity / intubation history: risk for subglottic stenosis
- Gradual worsening: suggests growing lesion (subglottic haemangioma, mediastinal mass)
Older children/Adults:
- Choking episode: foreign body until proven otherwise
- Prior airway procedures / intubation: post-intubation stenosis
- Duration and rate of progression
- Associated voice change, dysphagia, odynophagia, referred otalgia
- Baseline noise quality (helps localize level of obstruction)
Examination
- Observe first - at rest, do not disturb if critical
- Vital signs - SpO2, RR, HR
- Signs of increased work of breathing: suprasternal, intercostal, subcostal recession; nasal flaring; head bobbing; accessory muscle use
- Do NOT lay down or examine throat in drooling stridulous child
- Differentiate inspiratory/expiratory/biphasic
- Position preference (worse supine - pedunculated laryngeal mass or micrognathia)
- Transcutaneous oximetry invaluable in neonates/infants
- Resuscitation trolley and emergency airway equipment ready
Investigations
| Investigation | Use |
|---|---|
| Lateral soft tissue neck X-ray | Epiglottitis (thumb sign), retropharyngeal abscess (widened prevertebral space), subglottic narrowing |
| AP neck X-ray (PA chest) | "Steeple sign" in croup |
| CT neck/chest | Extrinsic compression, vascular rings, masses |
| Flexible nasendoscopy | Bedside assessment of supraglottis, vocal cords; can assist intubation |
| Microlaryngoscopy and bronchoscopy (MLB) | Definitive diagnosis of paediatric airway pathology |
| Barium swallow | Vascular ring, aspiration, TOF |
| MRI/echo | Cardiac and neurological causes of vocal cord palsy |
| Polysomnography | Severity of airway obstruction during sleep |
| ABG + SpO2 | Degree of respiratory compromise |
Management
Immediate/Acute
- Secure airway - in any cyanosed, severely distressed child, this takes priority
- Position - sitting upright, allow child to adopt position of comfort
- Oxygen supplementation
- Heliox (79% helium / 21% oxygen OR 1:2 helium-air mixture) - lower density allows less effort breathing; useful temporising measure in acute stridor
- Nebulised adrenaline (1 ml/kg of 1:1000, max 5 ml) - for croup with severe obstruction
- Corticosteroids - dexamethasone or nebulised budesonide for croup (effective within 30-60 minutes, reduce hospital stay)
- Intubation - all epiglottitis, >80% bacterial tracheitis, severe cases
- Tracheostomy - if intubation fails, or for chronic severe obstruction
Cause-Specific
| Cause | Treatment |
|---|---|
| Croup | Steroids + nebulised adrenaline; <5% need intubation |
| Epiglottitis | IV antibiotics + intubation under GA in theatre |
| Bacterial tracheitis | IV antibiotics + intubation + tracheal toilet |
| Laryngomalacia | Observation; supraglottoplasty if severe |
| Subglottic stenosis | Balloon dilation, anterior cricoid split, laryngotracheal reconstruction |
| Subglottic haemangioma | Propranolol (first-line), CO2 laser |
| Vocal cord palsy | Observation; tracheostomy for bilateral; laryngeal reinnervation |
| Allergic angioedema | Adrenaline 1:1000 SC + antihistamines + corticosteroids |
| Hereditary angioedema | IV C1 esterase inhibitor; icatibant; conestat alfa |
| Foreign body | Rigid bronchoscopy retrieval |
Severity Assessment (Westley Croup Score - applied to stridor broadly)
Stridor requiring admission includes: stridor at rest, SpO2 <92%, severe recession, altered mental status, poor air entry, or failure to respond to outpatient treatments.
Signs indicating respiratory failure and impending arrest:
- Extreme distress or paradoxically quiet (stridor may diminish in respiratory failure due to lack of airflow)
- Altered mental status
- Cyanosis / pallor / mottled skin
- Hypotonia
Key ENT Exam Points (Summary)
- Stridor = turbulent airflow = partial obstruction
- Inspiratory = at/above glottis (extrathoracic)
- Expiratory = intrathoracic
- Biphasic = subglottis/trachea (fixed lesion)
- Most common infant stridor = laryngomalacia
- 2nd most common newborn stridor = vocal cord palsy
- Epiglottitis = ALL need intubation; Croup = <5% need intubation
- "Stridor + drooling" = do NOT examine throat
- Heliox + nebulised adrenaline + steroids = acute medical management
- Definitive airway investigation = microlaryngoscopy and bronchoscopy (MLB)
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol 1 & 2); Cummings Otolaryngology Head and Neck Surgery; Bailey and Love's Short Practice of Surgery; K.J. Lee's Essential Otolaryngology; Rosen's Emergency Medicine; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.