Cushing syndrome with diagram
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Generating Image
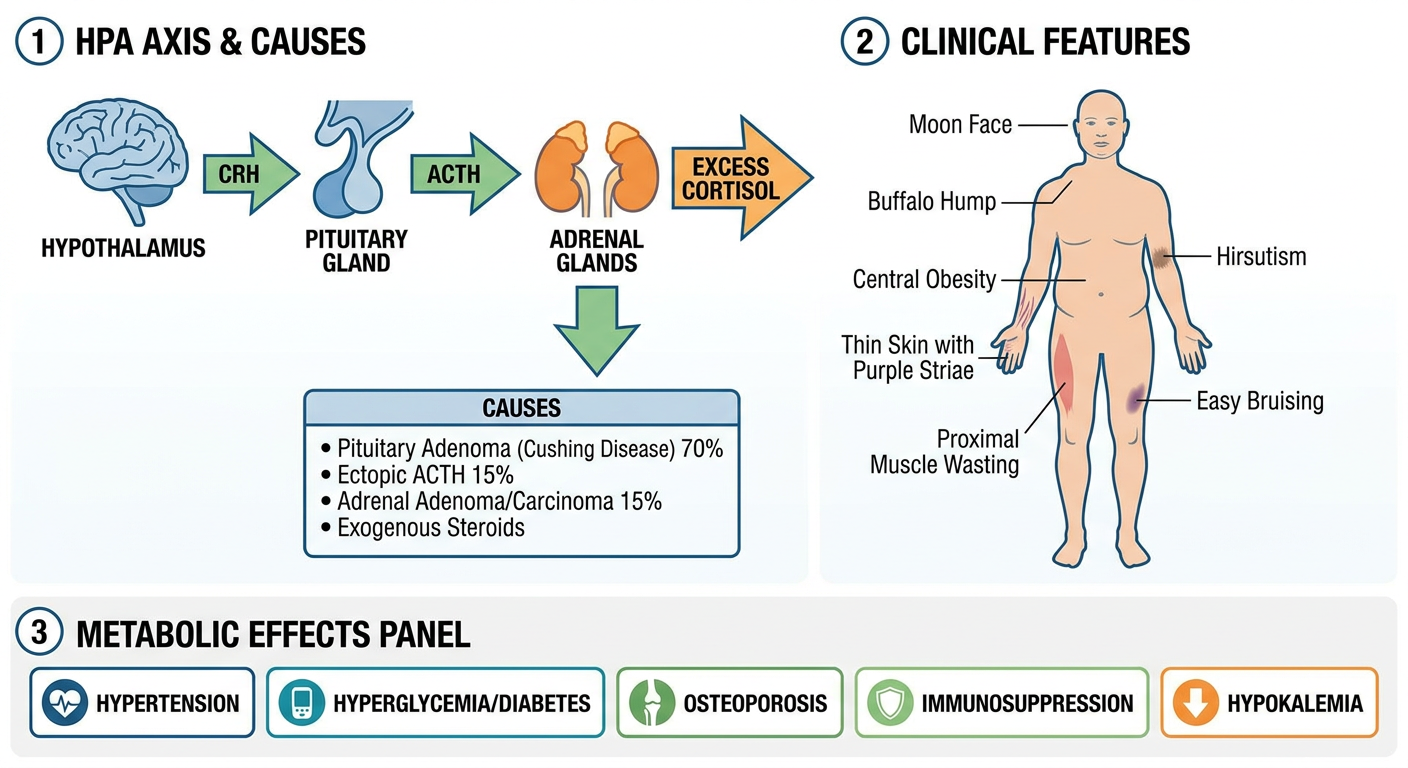
Medical diagram of Cushing syndrome showing: (1) HPA axis with hypothalamus releasing CRH, pituitary releasing ACTH, and adrenal glands producing excess cortisol - with causes labeled (pituitary adenoma/Cushing disease 70%, ectopic ACTH 15%, adrenal adenoma/carcinoma 15%, exogenous steroids); (2) body figure showing all classic clinical features: moon face, buffalo hump, central obesity, thin skin with purple striae, proximal muscle wasting, easy bruising, hirsutism; (3) metabolic effects panel: hypertension, hyperglycemia/diabetes, osteoporosis, immunosuppression, hypokalemia. Clean educational medical illustration style with labels and color-coding.
I now have all the content needed. Let me compile a comprehensive, well-illustrated response.
Cushing Syndrome
Cushing syndrome is the clinical state resulting from chronic exposure to excess glucocorticoids - either from exogenous steroid use or from endogenous overproduction of cortisol.
Overview Diagram
Causes and Classification
Cushing syndrome is divided into exogenous and endogenous causes. Endogenous disease is further classified by whether it is ACTH-dependent or ACTH-independent.
| Cause | Frequency | ACTH Level |
|---|---|---|
| Exogenous glucocorticoids (iatrogenic) | Most common overall | Suppressed |
| Cushing's disease (pituitary corticotrope adenoma) | ~70% of endogenous | Normal/High |
| Ectopic ACTH (small cell lung CA, carcinoid, PanNET) | 10-15% | Very high |
| Adrenal adenoma or carcinoma | 15-20% | Suppressed |
| Ectopic CRH (rare neuroendocrine tumors) | <1% | Elevated |
Cushing's disease specifically refers to a pituitary ACTH-secreting adenoma - usually a microadenoma (<1 cm) that harbors activating somatic variants of the USP8 gene in 11-62% of cases. It is 3-8x more common in women aged 20-40 years. - Harrison's Principles of Internal Medicine 22E
Pathophysiology
The hypothalamic-pituitary-adrenal (HPA) axis is the key regulatory circuit:
- The hypothalamus releases CRH - stimulating the anterior pituitary
- The anterior pituitary releases ACTH (cleaved from POMC precursor) - stimulating the adrenal cortex zona fasciculata
- The adrenal cortex secretes cortisol (up to 20 mg/day normally)
- Cortisol completes the negative feedback loop by inhibiting CRH and ACTH production
- Cortisol secretion follows a circadian rhythm - peak in the morning, nadir around 11 PM
In Cushing syndrome, this feedback is disrupted - cortisol remains chronically elevated regardless of circadian pattern. - Campbell-Walsh-Wein Urology
Morphology (Adrenal Glands)
The adrenal appearance depends on the cause:
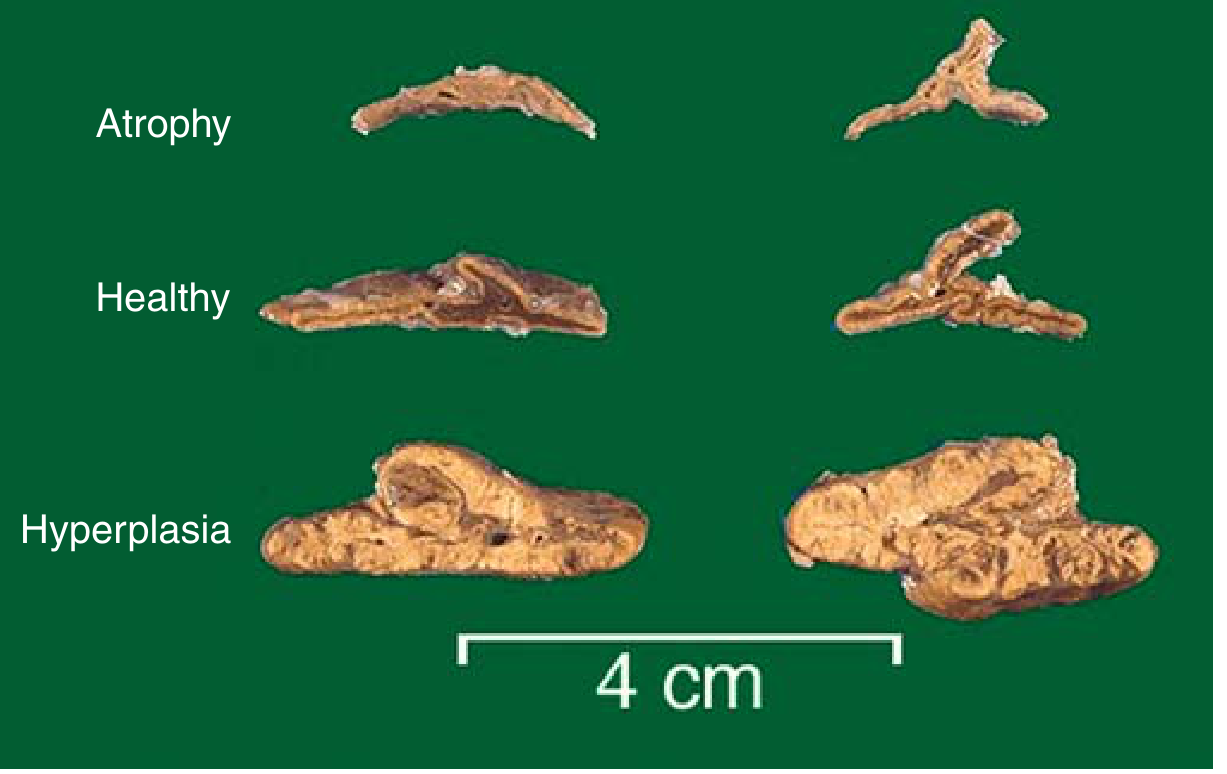
FIG. 18.31 - Adrenal glands in Cushing syndrome. Top: Atrophy (from exogenous steroid use, ACTH suppressed). Middle: Normal. Bottom: Diffuse bilateral hyperplasia (from ACTH-dependent disease).
-
Exogenous steroids → ACTH suppressed → bilateral cortical atrophy (zona fasciculata and zona reticularis; zona glomerulosa spared as it is not ACTH-dependent)
-
ACTH-dependent disease → bilateral cortical hyperplasia (each gland up to 30 g, yellow, thickened)
-
Pituitary adenoma → anterior pituitary shows Crooke hyaline change (basophilic cytoplasm of ACTH cells replaced by homogeneous pale material from accumulated keratin filaments)
-
ACTH-independent (adrenal adenoma/carcinoma) → autonomous secretion, contralateral gland atrophies
-
Robbins & Kumar Basic Pathology
Clinical Features
Cushing syndrome usually develops gradually. The signs and symptoms are exaggerations of cortisol's normal physiologic actions.
Classic Physical Signs

FIG. 18.33 - Central obesity, moon facies, and prominent abdominal striae in Cushing syndrome
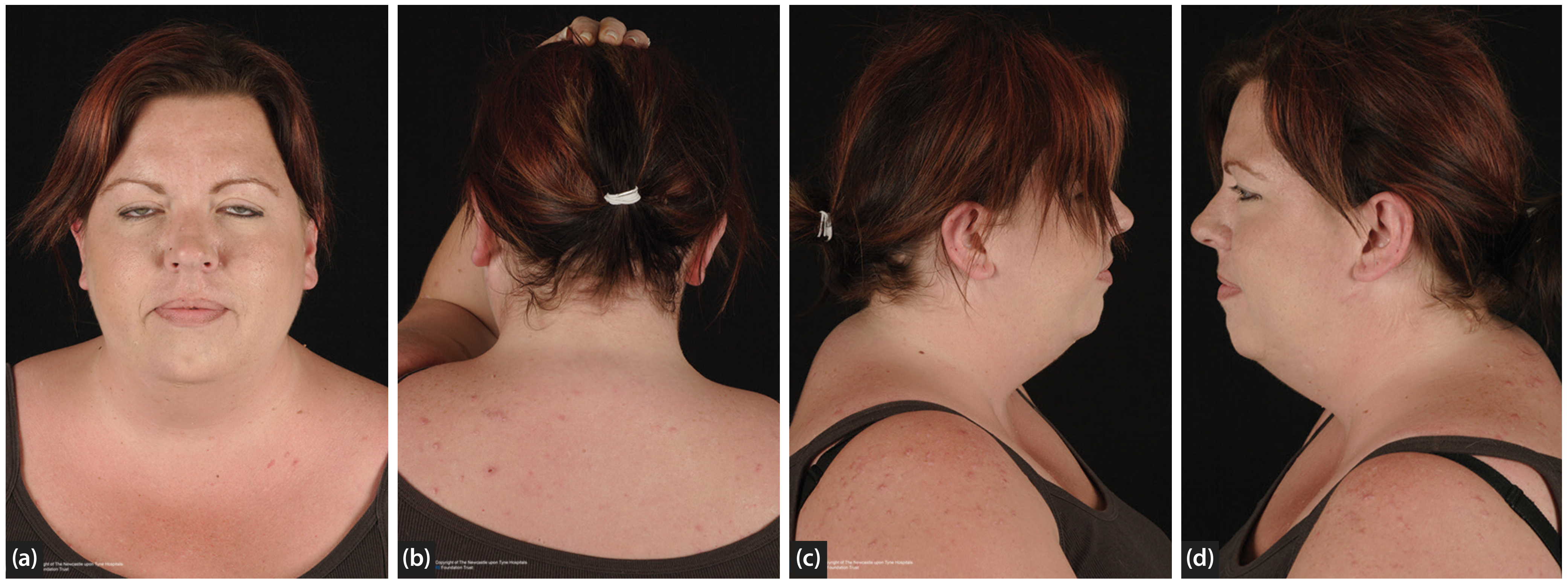
Figure 82.4 - Clinical appearance in Cushing's disease: (a) Moon face with plethora, (b) Buffalo hump - fat pad at posterior neck, (c-d) Facial fullness in profile
Clinical Features Organized by Mechanism
| Mechanism | Signs/Symptoms |
|---|---|
| Fat redistribution | Centripetal (truncal) obesity, moon face, buffalo hump (dorsocervical fat pad) |
| Muscle catabolism (type II fiber atrophy) | Proximal limb weakness, muscle wasting |
| Skin collagen loss | Thin fragile skin, easy bruising, purple/violaceous striae (abdomen, thighs), poor wound healing |
| Gluconeogenesis + insulin resistance | Hyperglycemia, secondary diabetes mellitus, glycosuria, polydipsia |
| Mineralocorticoid effect | Hypertension, hypokalemia, edema |
| Bone effects | Osteoporosis, vertebral fractures (reduced renal Ca absorption + increased urinary loss) |
| Immune suppression | Increased susceptibility to infections (bacterial, fungal, opportunistic) |
| Androgenic effects | Hirsutism, acne, menstrual irregularities (amenorrhea), reduced libido |
| Psychiatric | Mood swings, depression, anxiety, frank psychosis |
| ACTH excess (ectopic only) | Hyperpigmentation (ACTH stimulates melanocytes via MC1R) |
| Coagulation | Hypercoagulable state → DVT, pulmonary embolism |
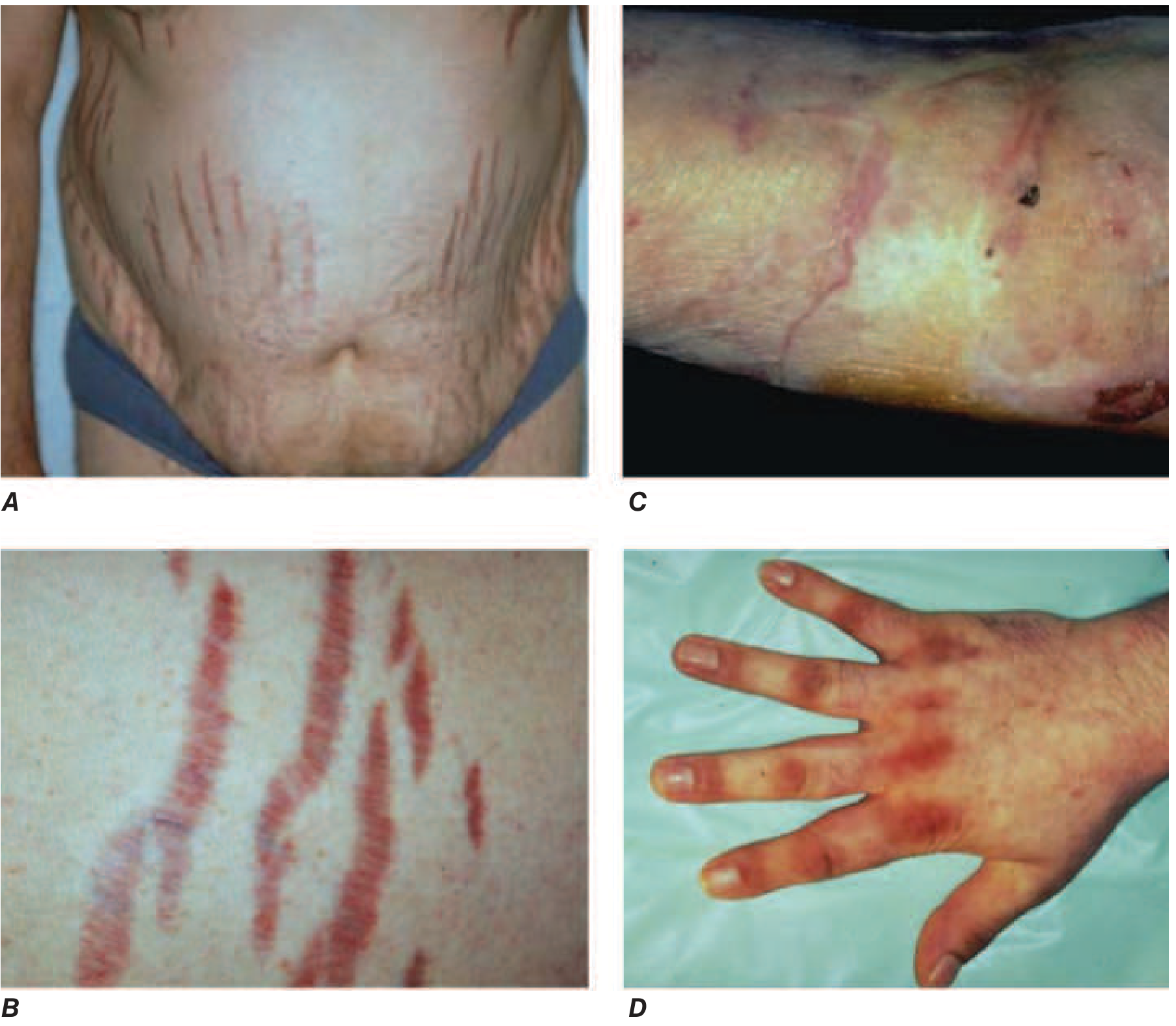
FIGURE 398-9 (Harrison's 22E) - A: Central obesity with broad purple striae. B: Close-up of striae. C: Thin/brittle skin. D: Knuckle hyperpigmentation in ectopic ACTH syndrome.
Diagnostic Value of Features (from Scott-Brown's)
| Diagnostic Value | Feature |
|---|---|
| High | Skin atrophy, proximal myopathy, easy bruising, childhood growth arrest, osteoporosis |
| Medium | Edema, striae, moon face, facial hirsutism, labile mood |
| Non-specific | Buffalo hump, hypertension, diabetes, plethora, acne |
Diagnosis
Step 1: Confirm Cortisol Excess
- 24-hour urinary free cortisol (3 separate collections) - elevated
- Overnight low-dose dexamethasone suppression test (DST): 1 mg dexamethasone at midnight; normal response = morning cortisol <1.8 mcg/dL; failure to suppress = Cushing's
- Late-night salivary cortisol: loss of diurnal rhythm is hallmark; cortisol should be at nadir (~11 PM) - elevated midnight level is pathological
Step 2: Determine ACTH Dependence
- Measure plasma ACTH
- Suppressed (<10 pg/mL) → ACTH-independent → adrenal imaging (CT/MRI)
- Normal or elevated → ACTH-dependent → go to step 3
Step 3: Localize the Source (if ACTH-dependent)
- Pituitary MRI: look for adenoma
- High-dose DST (8 mg): pituitary adenoma will partially suppress cortisol; ectopic ACTH will not
- CRH stimulation test: pituitary adenoma will respond; ectopic source will not
- Inferior petrosal sinus sampling (IPSS): gold standard for differentiating pituitary vs. ectopic ACTH
Harrison's Principles of Internal Medicine 22E emphasizes: most management errors occur when imaging is ordered before confirming whether cortisol excess is ACTH-dependent or independent.
Treatment
| Cause | Treatment |
|---|---|
| Exogenous | Gradual taper of steroids |
| Cushing's disease (pituitary adenoma) | Transsphenoidal adenomectomy (first line) |
| Ectopic ACTH | Treat underlying tumor; bilateral adrenalectomy if unresectable |
| Adrenal adenoma | Unilateral adrenalectomy |
| Adrenal carcinoma | Adrenalectomy + mitotane |
| Medical therapy (bridge/adjunct) | Ketoconazole, metyrapone, osilodrostat, pasireotide, cabergoline |
Untreated Cushing's disease carries a 50% mortality at 5 years, mainly from cardiovascular complications. - Scott-Brown's Otorhinolaryngology
Key Summary
- Most common cause overall: exogenous (iatrogenic) glucocorticoids
- Most common endogenous cause: Cushing's disease (pituitary ACTH adenoma)
- Hallmark biochemistry: elevated cortisol + loss of diurnal rhythm
- Hallmark skin finding: broad purple/violaceous striae + thin fragile skin
- Hallmark fat distribution: centripetal - truncal, moon face, buffalo hump with limb sparing
- Danger: DVT/PE from hypercoagulability; opportunistic infections; osteoporotic fractures
Sources: Robbins & Kumar Basic Pathology | Harrison's Principles of Internal Medicine 22E | Campbell-Walsh-Wein Urology | Scott-Brown's Otorhinolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.