PXF in opthalmology
Reading File
Finding Sources
Finding Sources
Searching PubMed
pseudoexfoliation syndrome glaucoma
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive textbook content and clinical images to compose a thorough, well-illustrated answer.
Pseudoexfoliation Syndrome (PXF / PXS) in Ophthalmology
Definition
Pseudoexfoliation syndrome (PXF or PXS) is an age-related systemic disorder characterised by the production and progressive accumulation of a grey-white fibrillary extracellular material in ocular and non-ocular tissues. It is the most common identifiable cause of secondary open-angle glaucoma worldwide and a leading cause of glaucoma blindness. The glaucoma that results is called pseudoexfoliation glaucoma (PXG) or "capsular glaucoma."
- Wills Eye Manual, p. 595 | Kanski's Clinical Ophthalmology 10th ed., p. 397
Epidemiology
| Feature | Detail |
|---|---|
| Age | Rare before 50; prevalence increases rapidly after the 6th decade; ~5% prevalence at age 75-85 |
| Sex | More common in women |
| Geography | Highest prevalence in Scandinavia; found worldwide in all ethnic groups |
| Glaucoma risk | 15-30% have glaucoma at time of PXF diagnosis; cumulative risk requiring glaucoma treatment can reach 60% at 5 years |
| Laterality | Usually bilateral but often asymmetric; glaucoma confined to one eye in ~two-thirds of patients |
Pathogenesis
Pseudoexfoliative material is a grey-white fibrillary substance arising from abnormal extracellular matrix (ECM) metabolism. Key points:
- Deposited on: lens capsule, zonular fibres, iris, trabecular meshwork (TM), conjunctiva, and distant visceral organs (skin, heart, liver)
- Genetic basis: Single nucleotide polymorphisms (SNPs) in the LOXL1 gene (chromosome 15), which encodes lysyl oxidase-like 1, an enzyme vital for tropoelastin and collagen cross-linking and ECM maintenance. These SNPs are nearly universal in PXF patients in some populations, but are also common in individuals without PXF.
- Elevated homocysteine in plasma and aqueous humour is associated; inadequate dietary folate (which reduces homocysteine) may be a risk factor.
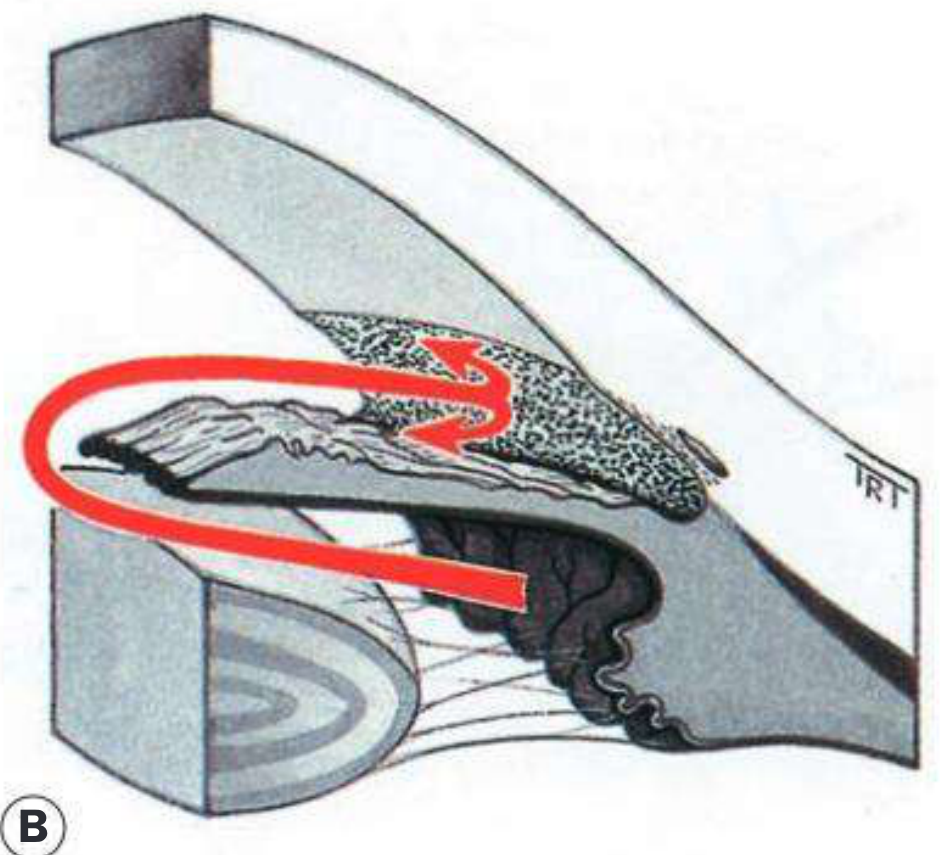
- IOP elevation results from trabecular obstruction by PXF material and liberated iris pigment, causing secondary degenerative outflow dysfunction.
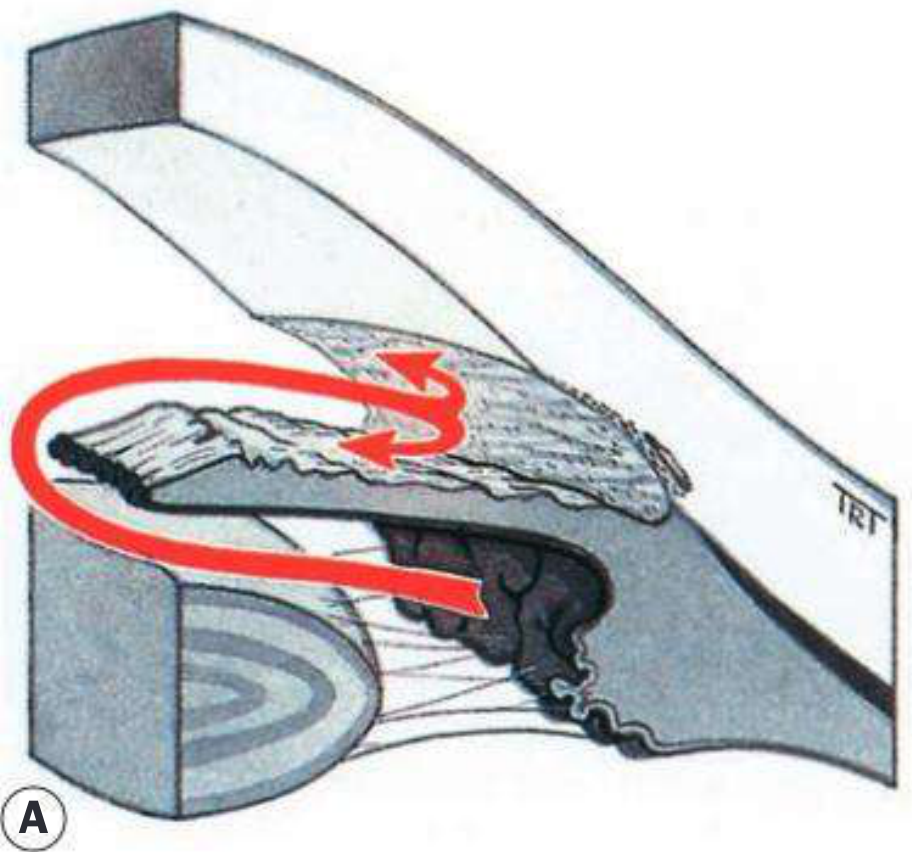
Diagrams (A & B from Kanski's) illustrating how PXF fibrillary material accumulates in the anterior segment angle and clogs the trabecular meshwork.
Clinical Signs
Slit Lamp (Critical Signs)
1. Anterior lens capsule - the classic "target pattern":
- Central zone: disc of PXF material (often with rolled-up edges)
- Mid-zone (clear zone): the iris rides over and wipes away PXF material during pupillary movement
- Peripheral cloudy zone: PXF deposits here undisturbed
Pupil dilation is often needed to visualise the full anterior lens capsular pattern.
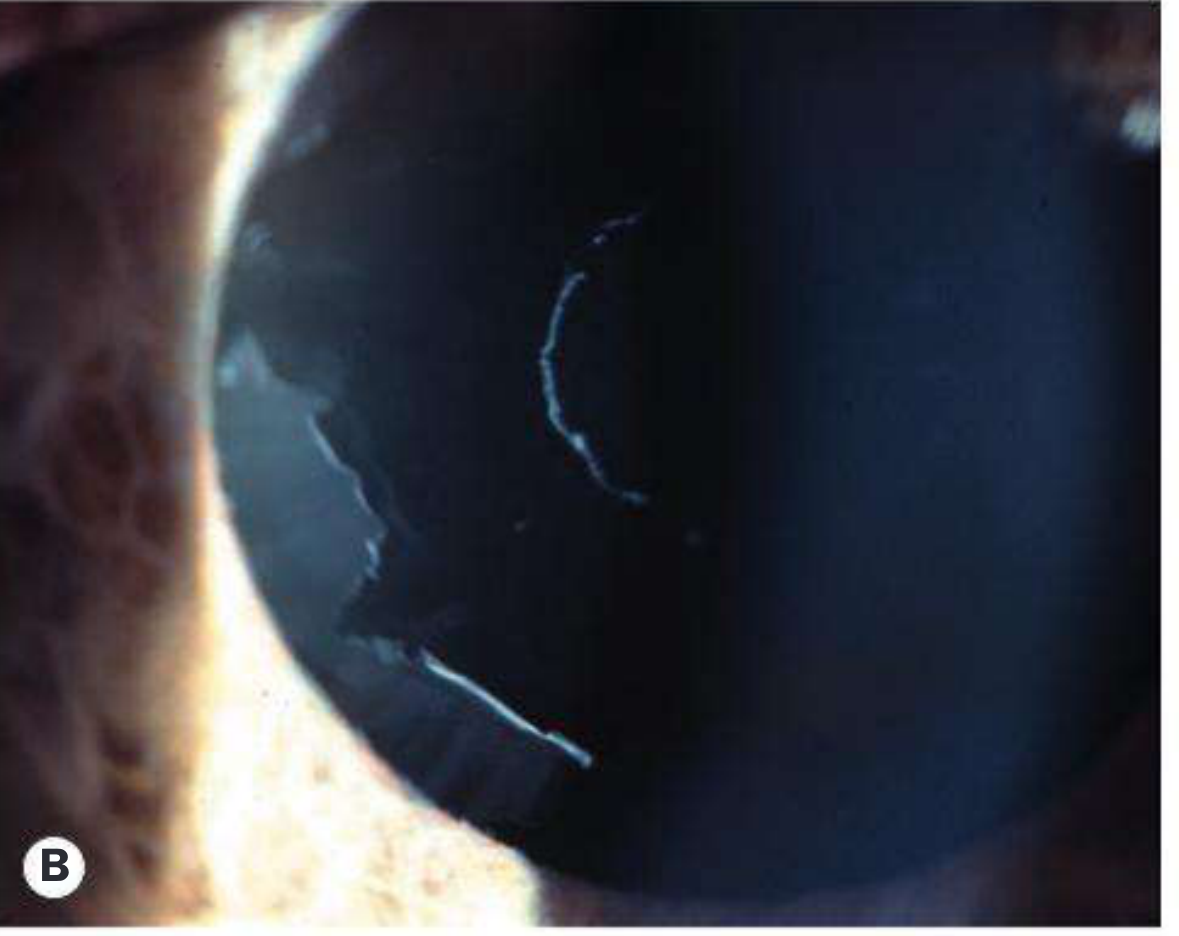
Fig: PXF material on anterior lens capsule (Kanski's) - note the white scrolled deposits at the peripheral zone boundary.
2. Pupillary margin:
- White, flaky PXF material visible at the pupillary border
- Peripupillary transillumination defects (TIDs) - from iris pigment loss at the sphincter region
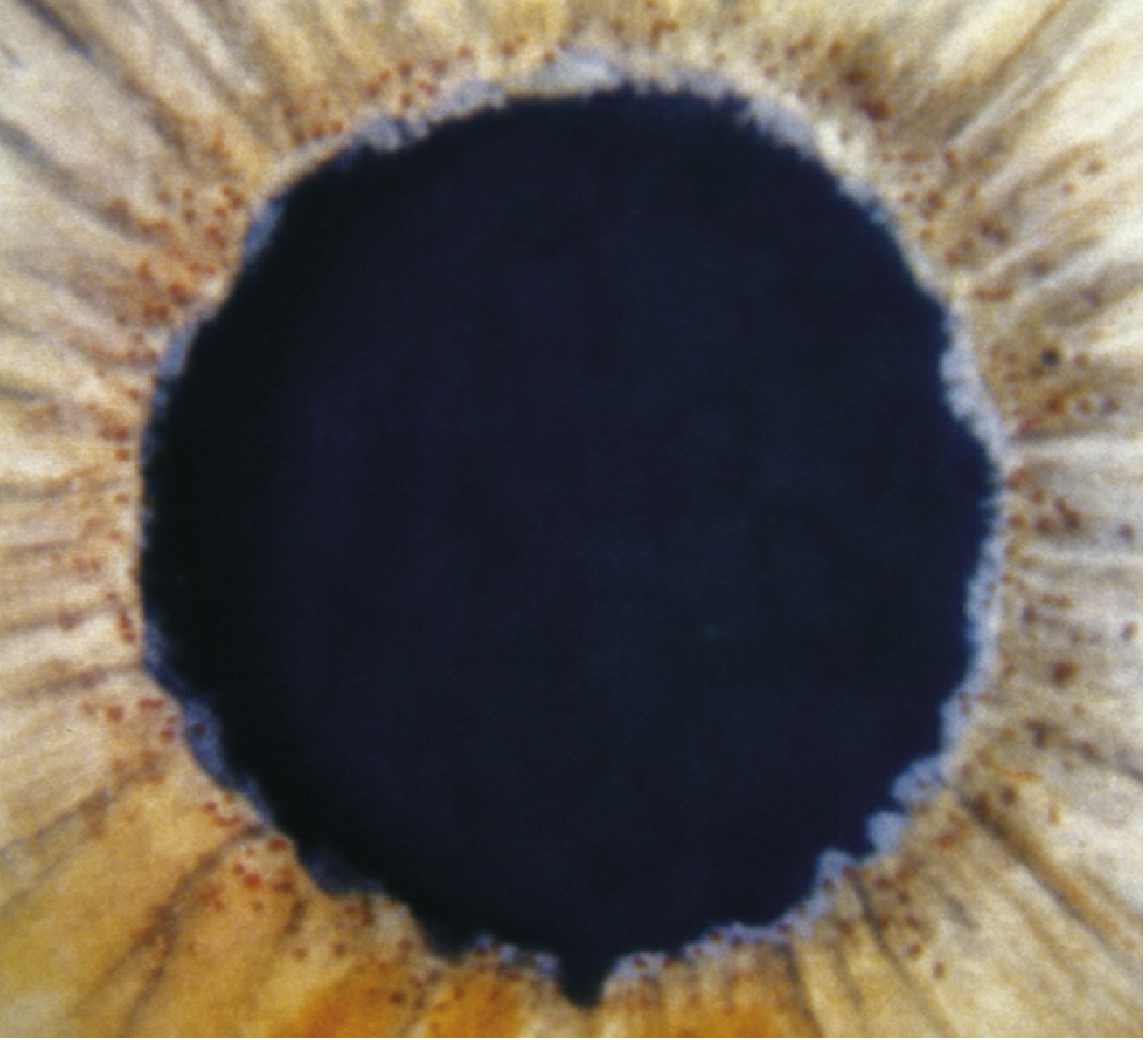
Fig 9.11.1 (Wills Eye): White PXF material at the pupillary margin with peripupillary iris transillumination defects.
3. Iris:
- Poor pupillary dilation (believed to be due to iris dilator muscle atrophy)
- Peripupillary iris atrophy
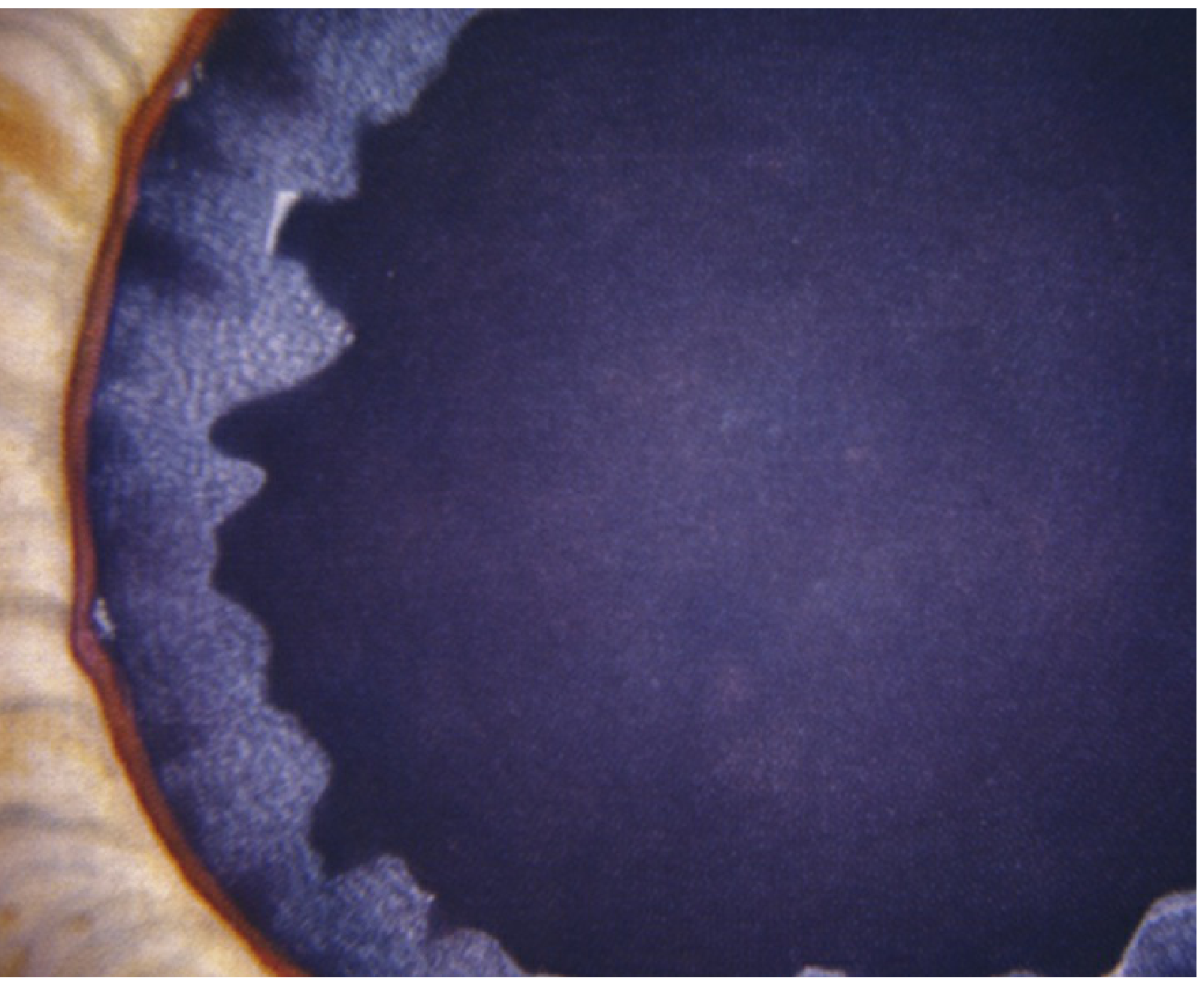
Fig 9.11.2 (Wills Eye): White material on the anterior lens capsule of a dilated PXF eye.
Gonioscopy (Angle Signs)
- Heavy, irregular trabecular pigmentation - especially inferiorly (more than in pigment dispersion)
- Sampaolesi line: an irregular pigment band on or anterior to the Schwalbe line, especially inferiorly - present but not pathognomonic (also seen in pigment dispersion syndrome)
- Dandruff-like PXF material deposits on trabecular meshwork
- Increased risk of secondary angle closure due to zonular laxity
Other Slit-Lamp Signs
- PXF material on the corneal endothelium (angular, irregular KP-like deposits); endothelial cell density is lower than normal
- Phacodonesis (lens tremulousness) from zonular weakness
- Cataract formation (more common - possibly from reduced aqueous ascorbate)
- Zonular fragility - spontaneous lens subluxation is rare, but surgical risk is high
IOP Characteristics
- PXF is associated with highly volatile IOP with large diurnal fluctuations
- IOP may rise acutely despite an open angle (mimicking acute angle closure)
- IOP levels tend to be higher than in POAG
Prognosis
Key teaching point: Pseudoexfoliation glaucoma progresses more rapidly than primary open-angle glaucoma (POAG) and is more likely to result in significant visual loss. Severe damage may be present at diagnosis and can develop very rapidly.
- Kanski's Clinical Ophthalmology, p. 398
Systemic Associations
- High-tone sensorineural hearing loss
- Ischaemic cardiovascular and cerebrovascular disease
- Increased risk of pelvic organ prolapse in older women
- Elevated plasma homocysteine
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Pigment dispersion syndrome | Mid-peripheral iris TIDs (not peripupillary); pigment on posterior lens equator; deep anterior chamber; typically young myopes; Krukenberg spindle on cornea |
| True capsular exfoliation | Trauma or chronic heat exposure (glassblowers); thin membrane peels from anterior capsule; glaucoma uncommon |
| Inflammatory glaucoma | Photophobia, flare; ragged "volcano-like" PAS; no PXF material |
| Primary amyloidosis | Amyloid deposits at pupillary margin/anterior capsule; systemic features |
| UGH syndrome | Prior intraocular surgery history |
Workup
- History: Family history; age; ethnicity
- Slit-lamp examination: Look for PXF material at pupillary margin; dilate pupil to assess anterior lens capsule
- Gonioscopy: Assess pigmentation pattern, Sampaolesi line, angle width
- Baseline glaucoma evaluation: IOP (including diurnal curve), optic disc assessment, visual fields, OCT RNFL
Treatment
Medical
- Similar to POAG - prostaglandin analogues are first-line
- Medical therapy fails more commonly than in POAG; IOP control is often more difficult
Laser
- Selective Laser Trabeculoplasty (SLT) is more effective in PXF than in POAG, with mean IOP reduction ~30%
- Caution: trabecular hyperpigmentation causes higher laser energy absorption - risk of transient IOP spikes
- SLT benefit may wane after ~2 years
Surgical
- Phacoemulsification alone can significantly lower IOP but carries high complication risks:
- Poor mydriasis (difficult to dilate)
- Zonular fragility and weakness - risk of zonular dehiscence
- Increased risk of intraoperative vitreous loss
- Postoperative IOP spikes, corneal oedema, inflammation, capsular opacification, and IOL dislocation
- Combined phaco + trabeculectomy for better IOP control
- Cataract extraction does NOT eliminate the glaucoma
Follow-Up
| Patient group | Interval |
|---|---|
| PXF with glaucoma | Every 1-3 months (as with POAG, but with awareness of rapid progression) |
| PXF without glaucoma | Every 6-12 months; treat at first sign of IOP elevation or glaucomatous damage |
Recent Evidence (2025)
A 2025 systematic review and meta-analysis (PMID 40131012) examined OCT alterations of the choroid and lamina cribrosa in PXF and PXG, providing new structural insights into how PXF affects deep optic nerve head architecture - relevant for understanding the aggressive progression of PXG beyond just IOP effects.
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach (10th ed.), pp. 397-399 | The Wills Eye Manual (7th ed.), pp. 595-598
This is a shared conversation. Sign in to Orris to start your own chat.