
IMG_0700.jpg
Read this
analyse_media
Here is a read of this chest X-ray:
Patient Info
- Patient ID: 935978 | Sex: Female
- Date/Time: 07/17/26 at 7:33 PM
- View: R-SIT AP (sitting anteroposterior, portable)
- Radiographer: MEJIA J | RTOD: PASCUANA
Technical Quality
- Suboptimal inspiration (common on portable/sitting films) - artificially magnifies the heart and mediastinum
- Mild rotation noted
Key Findings
Right Lung - ABNORMAL
- Large, dense homogeneous opacity in the right lower zone
- Upper border shows a meniscus-like curve laterally - strongly suspicious for a moderate-to-large right pleural effusion
- Right hemidiaphragm and right costophrenic angle are completely obscured
- Underlying right lower lobe consolidation or compressive atelectasis cannot be excluded (may be hidden by the fluid)
- Mild patchy bronchovascular markings in the right mid-to-upper zones
Left Lung - CLEAR
- No focal consolidation, mass, or nodule
- Left costophrenic angle is sharp - no left effusion
- Left hemidiaphragm visible and normal
Cardiac/Mediastinum
- Trachea is midline
- No significant mediastinal shift to the left (which would be expected with a massive effusion alone - the absence of shift suggests co-existing atelectasis/volume loss is pulling structures back rightward)
- Cardiac silhouette appears mildly enlarged, but this is likely exaggerated by the AP technique and low lung volumes
Subdiaphragmatic
- Prominent bowel gas visible in the upper abdomen - no obvious free air under the diaphragm
Bones/Soft Tissues
- No acute rib fractures, clavicle fractures, or lytic lesions identified
Impression
- Right pleural effusion (moderate-to-large) - the dominant finding
- Possible right lower lobe consolidation or atelectasis obscured by the effusion
- Apparent cardiomegaly - likely technique-related; recommend PA upright film for accurate assessment
Disclaimer: This is an AI-assisted image read for informational purposes only. All radiographic findings must be confirmed and formally interpreted by a licensed radiologist. Do not make clinical decisions based solely on this analysis.
Initial
Asking for Preferences
What are the criteria for plural effusion
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a comprehensive breakdown of the criteria for pleural effusion - covering diagnosis, classification, and characterization of the fluid:
Criteria for Pleural Effusion
1. Radiographic Criteria (Detection)
On a chest X-ray (like the one above):
- PA upright view: Blunting of the costophrenic angle - requires ~200-300 mL of fluid
- Lateral view: As little as 50-75 mL can blunt the posterior costophrenic angle
- AP supine/sitting view: Diffuse haziness over a hemithorax (as seen in this patient's right side)
- Findings: meniscus sign, blunting of costophrenic angles, opacification of a hemithorax, mediastinal shift (with large effusions)
2. Light's Criteria - Transudate vs. Exudate
The most important and widely used classification. Any ONE of the following makes it an exudate (sensitivity 98%, specificity 83%):
| Criterion | Threshold |
|---|---|
| Pleural fluid protein / Serum protein | > 0.5 |
| Pleural fluid LDH / Serum LDH | > 0.6 |
| Pleural fluid LDH | > 2/3 upper limit of normal serum LDH |
If none of the criteria are met → Transudate
- Washington Manual of Medical Therapeutics, p. 405
- Rosen's Emergency Medicine, p. 63.3
Heffner's Criteria (alternative - does not require serum values):
- Pleural fluid protein > 2.9 g/dL
- Pleural fluid cholesterol > 45 mg/dL
- Pleural fluid LDH > 45% of upper limit of normal serum value
3. Causes by Type
| Transudate | Exudate |
|---|---|
| Heart failure (most common) | Pneumonia / parapneumonic |
| Cirrhosis (hepatic hydrothorax) | Malignancy |
| Nephrotic syndrome | Tuberculosis |
| Hypoalbuminemia | Pulmonary embolism |
| Hypothyroidism | Autoimmune (RA, SLE) |
| Esophageal rupture |
4. Additional Fluid Criteria (After Transudate/Exudate Classification)
pH
- < 7.3 - parapneumonic effusion, malignancy, TB, rheumatoid, systemic acidosis
- < 7.0 - strongly suggests empyema or esophageal rupture → indication for chest tube
Glucose
- Low glucose - empyema, malignancy, TB, rheumatoid effusion
Cell Count & Differential
- Neutrophil predominant (>50%) - acute process: parapneumonic effusion, PE
- Lymphocyte predominant exudate - almost always TB or malignancy (PPV 97%)
- Eosinophilia - nonspecific (inflammation, viral, TB, pneumococcal, repeated thoracentesis)
- Low mesothelial cells (<5%) - highly suggestive of TB
Gram stain / Culture
- Positive → diagnosis of empyema
Cytology
- Positive for malignant cells → malignant pleural effusion (specific but not sensitive; sensitivity ~70%)
Hematocrit
- Pleural hematocrit / serum hematocrit > 0.5 → hemothorax
Triglycerides
-
110 mg/dL → chylothorax
- 50-110 mg/dL with clinical suspicion → lipoprotein electrophoresis for chylomicrons
Albumin Gradient (Serum - Pleural)
- < 1.2 g/dL = most specific single test for exudate (LR+ 10.88)
5. Size Classification (Radiographic)
| Size | Volume | Chest X-ray Finding |
|---|---|---|
| Small | <300 mL | Blunting of costophrenic angle |
| Moderate | 300-1500 mL | Opacity up to mid-lung field |
| Large/Massive | >1500 mL | Opacification of hemithorax ± mediastinal shift |
The X-ray you shared shows a moderate-to-large right pleural effusion based on the extent of opacification.
Sources: Washington Manual of Medical Therapeutics; Rosen's Emergency Medicine; Symptom to Diagnosis: An Evidence Based Guide, 4th Ed.
In xray and how to differentiate atilectasis and plural effusion in xray
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is the full breakdown of how to differentiate atelectasis from pleural effusion on chest X-ray:
Differentiating Atelectasis vs. Pleural Effusion on X-Ray
The Single Most Important Sign: Mediastinal/Tracheal Shift
| Feature | Pleural Effusion | Atelectasis (Collapse) |
|---|---|---|
| Mediastinal shift | AWAY from the opacity (contralateral) | TOWARD the opacity (ipsilateral) |
| Tracheal deviation | Pushed to opposite side | Pulled toward affected side |
| Diaphragm | Depressed / inverted (large effusions) | Elevated on the affected side |
| Lung volume | Normal or increased on affected side | Decreased - volume loss is the cardinal sign |
| Intercostal spaces | Widened (fluid expands chest) | Narrowed (lung shrinks) |
| Costophrenic angle | Blunted / obliterated | May be obliterated but from volume loss |
| Opacity border | Concave upward meniscus - higher laterally | Straight or wedge-shaped edge, may show fissure displacement |
| Air bronchograms | Absent (fluid surrounds lung) | Present (in some types - e.g. compressive) |
| Fissure displacement | No fissure shift | Fissures displaced toward the opacity |
Textbook Teaching Image
This figure from Murray & Nadel's shows the mediastinal shift difference clearly:
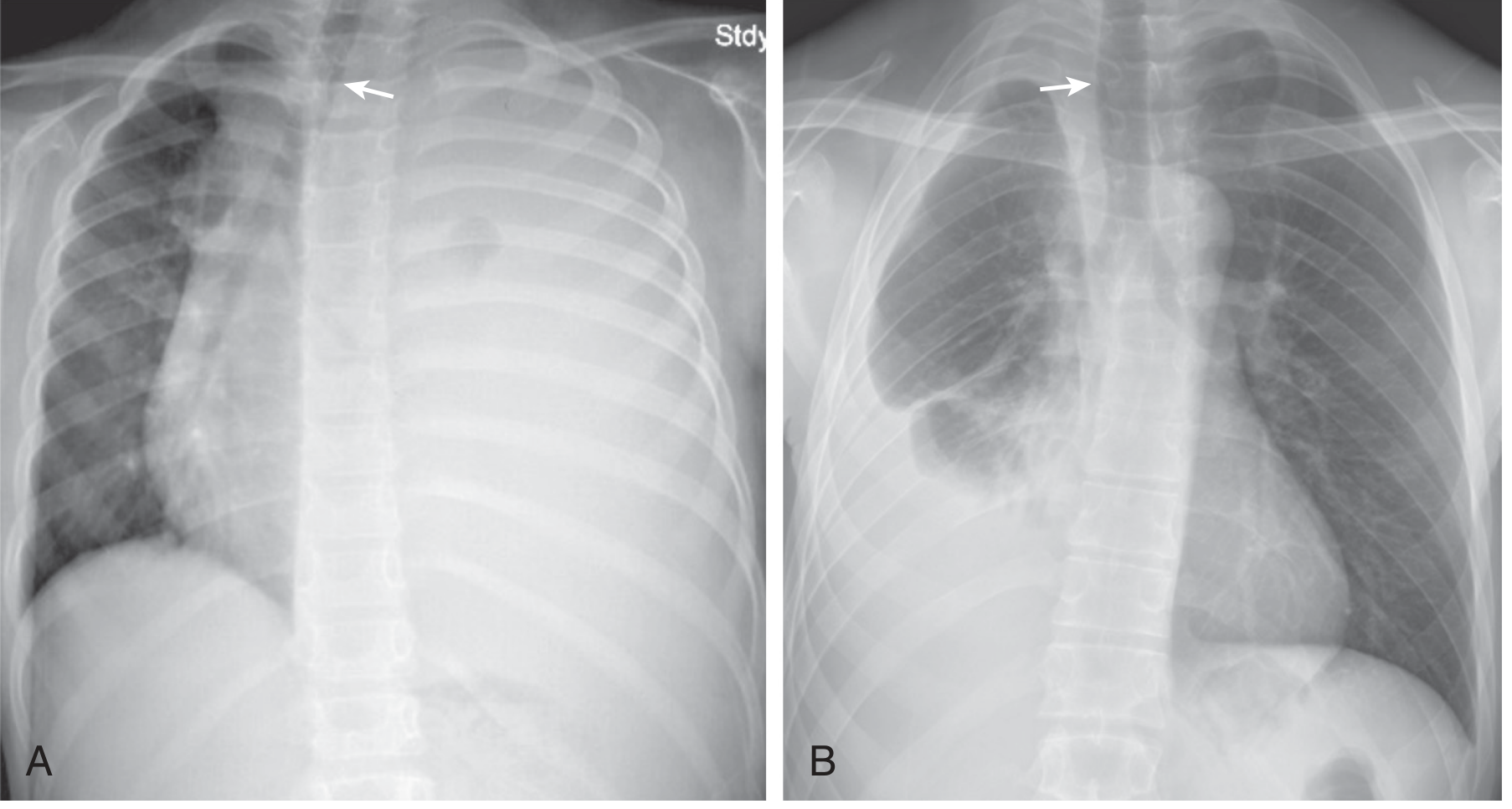
- (A) Large LEFT effusion - trachea pushed to the right (contralateral)
- (B) Right effusion with co-existing lung infiltration/atelectasis - trachea stays on the same side (no contralateral shift, or even slight ipsilateral shift)
Murray & Nadel's Textbook of Respiratory Medicine, eFig. 114.2
Key Differentiating Signs in Detail
1. Meniscus Sign
- Pleural effusion only - the upper border of the opacity forms a concave curve that is higher laterally than medially (fluid tracks up the lateral chest wall)
- Atelectasis has a straight, angular, or fissure-based border - no meniscus
2. Volume Loss (Cardinal Sign of Atelectasis)
- Atelectasis = collapsed/airless lung = lung takes up less space
- Signs of volume loss: elevated hemidiaphragm, narrowed intercostal spaces, ipsilateral mediastinal shift, compensatory hyperinflation of contralateral lung
- Effusion ADDS volume - pushes structures away
3. Opacification Pattern
- Effusion: Homogeneous, gravity-dependent opacity; the lung may still be visible floating above the fluid
- Atelectasis: Can be lobar (wedge-shaped, follows a lobe), linear/discoid (plate-like), or complete (white-out)
4. Air Bronchograms
- Present in atelectasis (especially compressive/passive atelectasis) - you can see air in the bronchi because the surrounding alveoli have collapsed
- Absent in pleural effusion (fluid separates the bronchi and is not airspace disease)
When Both are Present Simultaneously
This is exactly what is seen on the patient's X-ray above. When effusion + atelectasis coexist:
- Mediastinal shift may be absent or minimal - the two forces cancel each other out
- The effusion pushes the mediastinum away, while the atelectasis pulls it back
- The result is a white-out without mediastinal shift - which should always prompt suspicion of combined pathology or extensive pleural malignancy
"Absence of mediastinal shift with a large effusion raises the strong possibility of obstructive collapse of the ipsilateral lung or extensive pleural malignancy."
- Grainger & Allison's Diagnostic Radiology
Quick Summary Table
| Sign | Effusion | Atelectasis |
|---|---|---|
| Tracheal shift | Away (contralateral) | Toward (ipsilateral) |
| Diaphragm | Pushed down | Pulled up |
| Intercostal spaces | Widened | Narrowed |
| Meniscus sign | YES | No |
| Air bronchograms | No | YES (often) |
| Fissure displacement | No | YES (toward opacity) |
| Volume | Increased | Decreased |
When in Doubt: CT or Ultrasound
- Ultrasound - can detect as little as 5-10 mL of fluid; pleural fluid appears anechoic (black); atelectatic lung appears echogenic and may show the "lung pulse" sign
- CT chest - gold standard; clearly distinguishes fluid (low HU, gravity-dependent) from collapsed lung tissue (higher HU, may contain air bronchograms)
Sources: Grainger & Allison's Diagnostic Radiology; Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.