









+16 more
Interpretation
Reading File
analyse_media
analyse_media
analyse_media
analyse_media
Here is a structured interpretation of all 10 images of the CT scan belonging to Miss Abhiruchi Sonkar, Female, 35 years, from Raaghav Diagnostic Centre (3 film sheets, 3/3 pages).
CT Abdomen & Pelvis - Visual Interpretation
Important disclaimer: This is a visual assessment of photographs of printed CT films - not a reading of the original DICOM data. Subtle findings, small lesions, and precise densitometry cannot be reliably assessed from photographs. This does NOT replace an official radiologist's report.
Study Details
| Field | Information |
|---|---|
| Patient | Miss Abhiruchi Sonkar |
| Sex / Age | Female, 35 years |
| Centre | Raaghav Diagnostic Centre |
| Film sheets | 3 of 3 |
| Views | Axial (cross-sectional), Coronal (front-to-back), Sagittal (side-profile) |
Findings by Region
1. Liver
- Normal size and contour visible on upper axial and coronal slices.
- No grossly obvious large hypoattenuating (dark) or hyperattenuating (bright) focal masses visible at photograph resolution.
2. Spleen
- Normal size, homogeneous density.
- No gross splenomegaly or focal lesions identified.
3. Kidneys
- Both kidneys appear symmetric in size and position.
- No gross hydronephrosis (collecting system dilatation) or large exophytic masses visible.
4. Pancreas & Gallbladder
- Grossly unremarkable on available views; no large pancreatic masses or obvious biliary dilatation seen.
5. Gastrointestinal Tract
- Bowel gas and fluid distribution appears normal.
- No evidence of high-grade mechanical bowel obstruction.
- Rectosigmoid colon appears normal caliber, no obvious wall thickening.
6. Peritoneal Cavity
- No large-volume free fluid (ascites) visible in the paracolic gutters, perihepatic, or perisplenic spaces.
- No free air (pneumoperitoneum) identified.
7. Pelvis - Uterus & Adnexa
- The uterus is centrally located, normal size for a 35-year-old female.
- No grossly distorting large uterine or adnexal masses identified.
- No large ovarian cysts or solid masses clearly visible.
- Small physiological free fluid in the Pouch of Douglas cannot be excluded at this resolution (normal for premenopausal women).
8. Urinary Bladder
- Partially filled, smooth symmetric walls.
- No obvious intraluminal filling defects or gross wall thickening.
9. Lymph Nodes
- No bulky retroperitoneal or pelvic lymphadenopathy (enlarged nodes) visible.
- Normal-sized lymph nodes are not resolvable on photograph-resolution images.
10. Lumbar Spine & Bony Pelvis
- Normal lumbar lordosis preserved on sagittal views.
- Vertebral body heights appear maintained; no obvious compression fractures.
- Pelvic bones (iliac, sacrum, pubic rami) appear intact with normal joint spaces at the sacroiliac joints and hip joints.
- Color overlays (green/yellow, pink) visible on the sagittal reconstructions represent software-generated segmentation/annotation of the lumbar vertebrae (L2-L5) and sacrum - likely used for volumetric measurement, AI-assisted analysis, or highlighting a region of clinical interest (e.g., lower back pain evaluation).
Summary
At photograph resolution, no gross, large-scale abnormality is immediately apparent - no large tumors, major fluid collections, bowel obstruction, or significant bone destruction.
The colored annotations on the sagittal spine views suggest the study was specifically reviewed for a spinal or lower-back complaint (possibly lower back pain, radiculopathy, or sacral pathology).
Recommended Next Steps
- Obtain the official written radiology report - the radiologist reviewing digital DICOM images will have documented precise measurements, Hounsfield unit densities, and any subtle findings not visible on photograph.
- Window/level review - soft tissue, bone, and lung windows each reveal different pathology; only one window is visible per photograph frame.
- If pelvic pathology is suspected: Pelvic Ultrasound (transvaginal) or Pelvic MRI provides far superior soft-tissue contrast for uterine/ovarian assessment.
- If spinal pathology is the concern: MRI Lumbar Spine is the gold standard for disc disease, nerve root compression, and marrow pathology.
*This interpretation is for educational guidance only and must be correlated with clinical history, laboratory results, and the official radiologist's report by the treating physician.*Here is a clear, structured interpretation of both reports for Miss Abhiruchi Sonkar, 35Y/F, dated 13.07.2026.
Report 1 — Ultrasound Whole Abdomen
Centre: Rudradiagnostic Centre | Reported by: Dr. Rohan Kumar Singh (MD Radiodiagnosis, FIVIR)
Findings Summary
| Organ | Finding |
|---|---|
| Liver | Normal size (13.1 cm), echogenicity, no focal lesion, no biliary dilatation, portal vein normal |
| Gallbladder | Normal distension, wall thickness, no calculus/mass |
| CBD | Normal course and caliber, no calculus |
| Pancreas | Normal size, shape, echogenicity, no focal lesion |
| Spleen | Normal size (8.7 cm), no focal lesion |
| Retroperitoneum | No lymphadenopathy, no free fluid in peritoneal or pleural cavities |
| Right Kidney | Normal size, shape, parenchyma - BUT: mild dilatation of the proximal right ureter; distal ureter could not be traced due to bowel gas obscuring it |
| Left Kidney | Normal in all parameters; no calculus, hydronephrosis, or mass |
| Urinary Bladder | Normal - wall thickness normal, both VUJ (vesico-ureteric junctions) normal, no calculus/mass |
| Uterus | Normal size (7.0 × 4.2 × 3.1 cm), normal echotexture, normal endometrium |
| Ovaries | Both normal size and shape; adnexa appear normal |
| POD (Pouch of Douglas) | No free fluid |
Impression (USG)
Right proximal ureter dilatation - likely obstructive etiology. Possibility of right ureteric calculus.
- NCCT KUB recommended for further evaluation.
Report 2 — NCCT KUB (Non-Contrast CT of Kidneys, Ureters, Bladder)
Centre: Raaghav Diagnostic Centre | Reported by: Dr. Sushma Rani (MD Radiodiagnosis)
Findings Summary
| Structure | Finding |
|---|---|
| Right Kidney | Normal size (81 × 46 mm), normal parenchyma, smooth outline |
| Right Ureter | Normal in course and caliber; no evidence of calculus or calcification |
| Right perirenal fat | Normal |
| Left Kidney | Normal size (77 × 41 mm), normal parenchyma and outline |
| Left Ureter | Normal course and caliber; no calculus/calcification |
| Urinary Bladder | Normal shape, outline, distension, wall thickness; no mass lesion |
| Uterus | Normal size and density; no adnexal mass |
Impression (NCCT KUB)
Normal study of KUB region.
Clinical Correlation & What This Means
The Key Finding
The USG showed mild dilatation of the right proximal ureter, raising suspicion for a right ureteric calculus causing partial obstruction. This prompted the NCCT KUB.
The NCCT KUB Result
The NCCT KUB - which is the gold standard for detecting ureteric stones (sensitivity ~95-98%, specificity ~96%) - came back completely normal. Specifically:
- No calculus or calcification anywhere in the KUB tract bilaterally
- No hydronephrosis
- Normal ureteric caliber bilaterally
Interpretation
| Possible Explanation | Comment |
|---|---|
| Spontaneous passage of stone | If a small stone was present, it may have passed between the two studies |
| Transient ureteric peristalsis | Mild proximal ureteral dilatation on USG can be a transient/positional finding, not always pathological |
| Bowel gas artifact on USG | The ultrasound itself noted the distal ureter was untraceable due to bowel gas, reducing the reliability of that study |
| Extrinsic compression | Less likely given the normal CT |
Bottom Line
The NCCT KUB is reassuring - no stone is currently present in the urinary tract. All other abdominal and pelvic organs are normal on both studies.
Recommended Next Steps
- Clinical correlation - is the patient symptomatic (right flank pain, hematuria)? If symptoms persist, further evaluation is warranted.
- Urine routine/microscopy - check for hematuria or infection, which would support a recent stone passage.
- Follow-up USG - if mild right hydronephrosis recurs on repeat imaging, urological evaluation should be sought.
- No immediate intervention needed based on current imaging.
This interpretation is for educational/informational purposes only. Please discuss these reports with the treating physician (Dr. K.M. Chaudhary / Dr. Nilima Verma) for clinical decision-making.
Explain by the each view of NCCT
The NCCT KUB uses three standard views/planes to examine the urinary tract. Let me explain each one using the actual CT films already shared.
The Three Views in an NCCT KUB
1. AXIAL VIEW (Cross-Sectional / "Slice" View)
This is the most numerous set of images - the horizontal slices from top to bottom
What it looks like
- Oval/circular frames showing a horizontal "slice" of the body at each level
- Like cutting a loaf of bread - you see the inside at that exact level
- Visible in Film Sheet 1 (page 1/3) - the large grid of oval images
What is evaluated in each slice
At the level of the kidneys (upper abdomen slices):
- Size, shape, and outline of each kidney
- Parenchymal (kidney tissue) density - should be uniform gray
- Collecting system (renal pelvis) - should not be dilated/bright white
- Stones appear as bright white (hyperdense) spots - easy to spot on non-contrast CT
- Perirenal fat - should be clean, not "dirty/stranded" (which would suggest infection or inflammation around a stone)
- Aorta and IVC visible centrally
At the level of the ureters (mid-abdomen slices):
- Ureters are thin tubes running along the psoas muscle, just beside the spine
- Normally very thin (~3 mm) - you follow them slice by slice going downward
- A stone appears as a bright white dot within the ureteric lumen
- "Soft tissue rim sign" - soft tissue halo around a bright dot = confirms it is in the ureter (not a vascular calcification)
At the level of the bladder (pelvic slices):
- Bladder appears as a large oval structure in the pelvis
- Uterus visible posterior to bladder in females
- VUJ (vesico-ureteric junction) - where the ureter enters the bladder - most common site for stones to get stuck
- Stones at VUJ appear as bright dots at the bladder wall
In Miss Abhiruchi's CT:
- All axial slices showed normal kidney size (R: 81×46 mm, L: 77×41 mm)
- No bright hyperdense foci anywhere along the ureteric course
- No perinephric fat stranding (no inflammation)
2. CORONAL VIEW (Front-to-Back Reconstruction)
The tall, narrow portrait-orientation images - like looking at the body from the front
What it looks like
- Long vertical images showing the full body from front to back
- You can see both kidneys, both ureters, and the bladder all at once in a single image
- Visible in Film Sheet 3 (page 3/3) - top rows of tall vertical images, and also seen on the multiplanar film sheets
What is evaluated
Overall urinary tract at a glance:
- Both kidneys seen simultaneously - easy to compare size and position
- The entire course of both ureters from kidney to bladder can be traced in sequence
- Collecting system anatomy (renal calyces, pelvis, ureteropelvic junction / UPJ)
- Hydronephrosis (dilated collecting system) is very obvious on coronal view - appears as a black (fluid-filled) branching pattern within the kidney
- Any stone causing obstruction causes dilation above it - seen as the "column of fluid" above the bright stone dot
Spine and surrounding structures:
- Lumbar vertebrae seen in midline
- Psoas muscles on either side - ureters run along these
- Iliac vessels, bowel loops visible
In Miss Abhiruchi's CT:
- Coronal views confirmed both collecting systems are normal (no black branching hydronephrosis pattern)
- No ureteric dilation seen along the full length of either ureter
- The colored segmentation overlays (green/yellow on sagittal spine) are software annotations - not pathology
3. SAGITTAL VIEW (Side-Profile Reconstruction)
The tall narrow images showing the body from the side - like an X-ray side view
What it looks like
- Side-profile view, like slicing the body from left to right
- Shows spine, aorta, bladder, uterus in profile
- Visible in Film Sheet 3 (page 3/3) - the lower rows with the spine visible
What is evaluated
Spine anatomy:
- Lumbar vertebral alignment, disc spaces
- Sacrum and pelvis in profile
Bladder and uterus:
- Relationship between bladder (front) and uterus/rectum (behind) clearly seen
- Bladder wall thickness measured
- Post-void residual can be estimated
Aorta and vessels:
- Abdominal aorta runs anterior to the spine
- Aortic calcification would be visible as bright deposits on the vessel wall
Ureter (limited visibility):
- Sagittal is less useful for the ureter specifically (ureters run front-to-back and are better seen on axial and coronal)
- However, it helps confirm no retroperitoneal mass displacing the ureters
In Miss Abhiruchi's CT:
- Normal lumbar lordosis
- No obvious disc collapse or vertebral pathology
- Bladder appears normal in profile
Summary Table: Three Views Compared
| Feature | Axial | Coronal | Sagittal |
|---|---|---|---|
| Appearance | Horizontal oval slices | Tall vertical front-view | Tall vertical side-view |
| Best for stones | ✅ Best - shows exact stone location | ✅ Good - shows dilation above stone | Limited |
| Best for hydronephrosis | ✅ Yes | ✅ Best overview | Partial |
| Best for kidney size | ✅ Yes | ✅ Yes (both together) | No |
| Ureter tracing | ✅ Slice by slice | ✅ Full course visible | Limited |
| Bladder | ✅ Yes | ✅ Yes | ✅ Profile view |
| Spine | ✅ Cross-section | Front view | ✅ Best for alignment |
Why NCCT (Non-Contrast) Specifically?
- Stones are calcium-based and naturally bright (hyperdense) on CT without any contrast
- Adding contrast dye would actually obscure small stones (the bright dye fills the ureter and hides the stone)
- NCCT is faster, cheaper, no allergic risk from contrast
- Sensitivity for stones: ~97%, which is why it is the gold standard over USG
Miss Abhiruchi's Result Across All Three Views
All three views (axial slices, coronal reconstructions, sagittal reconstructions) showed:
- ✅ Normal kidneys bilaterally
- ✅ No calculus or calcification anywhere in KUB tract
- ✅ No hydronephrosis or ureteric dilation
- ✅ Normal bladder
- ✅ No perinephric fat stranding
Conclusion: Normal NCCT KUB - the proximal right ureteric dilatation seen on ultrasound was not confirmed on CT, most likely representing either a transient finding or a small stone that had already passed.
Further treatment
Finding Sources
Searching PubMed
ureteral calculus management conservative treatment
Finding Sources
Searching PubMed
urolithiasis medical expulsive therapy alpha blocker
Finding Sources
Reading File
Reading File
Here is a complete, evidence-based further treatment plan for Miss Abhiruchi Sonkar, structured for the treating physician.
Further Management Plan
Patient: Miss Abhiruchi Sonkar | 35Y / Female
Clinical Scenario: Right proximal ureteric dilatation on USG → NCCT KUB normal (no stone confirmed)
Step 1 — Immediate Clinical Assessment
Before any treatment, the treating physician must answer three questions:
| Question | Significance |
|---|---|
| Is she symptomatic? (right flank/loin pain, hematuria) | Determines urgency |
| Any fever / chills / dysuria? | Rules out infection / pyelonephritis |
| Any nausea/vomiting, pain radiating to groin? | Classic ureteric colic features |
Step 2 — Urine Investigations (Order Now)
These are the most important immediate tests:
| Test | Purpose |
|---|---|
| Urine routine & microscopy | Look for RBCs (hematuria confirms stone passage), pus cells (infection), crystals (stone type clue) |
| Urine culture & sensitivity | Rule out UTI / pyelonephritis if any fever/symptoms |
| Urine pH | Acidic = uric acid stones; Alkaline = struvite/infection stones |
| Serum creatinine & urea | Assess kidney function - especially important given right ureteric dilatation |
| Serum calcium, uric acid | Metabolic workup to identify stone-forming tendency |
| CBC | Rule out infection (raised TLC) |
Scenario A — Patient is Asymptomatic (Most Likely Given Normal NCCT)
Interpretation
- The right proximal ureteric dilatation was likely a transient finding - stone probably passed spontaneously before NCCT was done
- NCCT is 97-99% sensitive for stones; a normal NCCT effectively rules out active obstruction
Management
No active urological intervention needed at this time.
-
Increase fluid intake - Target urine output >2 liters/day
- Dilutes urine, reduces stone re-formation risk
- Drink at least 2.5-3 liters of water daily
-
Dietary advice:
- Reduce sodium intake (high sodium increases urinary calcium excretion)
- Moderate animal protein intake
- Adequate calcium in diet (do NOT restrict calcium - paradoxically increases oxalate absorption)
- Reduce oxalate-rich foods if calcium oxalate stones suspected (spinach, nuts, chocolate, tea)
-
Follow-up USG KUB after 4-6 weeks to confirm resolution of right ureteric dilatation
-
Metabolic stone workup if there is any family history of stones or recurrent episodes:
- 24-hour urine for calcium, oxalate, uric acid, citrate, phosphate, sodium, creatinine
Scenario B — Patient Has Active Symptoms (Flank Pain / Hematuria)
This means a stone may still be present but was missed on NCCT (rare, <3%) OR a new episode has started.
Pain Management (Acute Renal Colic)
| Drug | Dose | Notes |
|---|---|---|
| Tab. Diclofenac (NSAID - first line) | 75 mg IM/oral | Best for ureteric colic; reduces ureteral spasm |
| Tab. Ketorolac | 30 mg IM | If rapid relief needed |
| Injection Tramadol | 100 mg slow IV | If NSAIDs contraindicated |
| Tab. Ondansetron | 4 mg | For nausea/vomiting |
| Hyoscine butylbromide (Buscopan) | 20 mg IV/oral | Antispasmodic for ureteral spasm |
NSAIDs are the first-line analgesic for ureteric colic - they are superior to opioids per evidence - Brenner & Rector's The Kidney
Medical Expulsive Therapy (MET)
Indicated if a stone ≤10 mm is suspected/present in the ureter:
| Drug | Dose | Mechanism |
|---|---|---|
| Tab. Tamsulosin 0.4 mg (Alpha-1 blocker) | Once daily at bedtime | Relaxes ureteral smooth muscle, reduces peristaltic spasm → facilitates stone passage |
| Tab. Nifedipine 30 mg (Calcium channel blocker) | Once daily | Alternative if tamsulosin not tolerated |
Evidence: A Cochrane review of 67 studies (10,509 participants) confirmed alpha blockers increase stone clearance and shorten expulsion time. Tamsulosin is superior to nifedipine. Especially effective for stones >5 mm - Brenner & Rector's The Kidney
Duration: Continue for 4 weeks or until stone passes (whichever is earlier)
Side effects of tamsulosin to counsel: Postural hypotension (dizziness on standing), retrograde ejaculation (not relevant here), nasal congestion
Scenario C — Red Flags Requiring Urgent Urology Referral
Refer immediately if any of the following are present:
| Red Flag | Reason |
|---|---|
| Fever + loin pain + rigors | Infected hydronephrosis / urosepsis - emergency |
| Persistent pain >72 hours despite adequate analgesia | Surgical intervention needed |
| Worsening hydronephrosis on repeat imaging | Obstruction with risk of renal damage |
| Single functioning kidney | No tolerance for obstruction |
| Bilateral ureteric obstruction | Acute kidney injury risk |
| Rising serum creatinine | Obstructive nephropathy |
Surgical Options (if needed)
| Procedure | When Used |
|---|---|
| ESWL (Extracorporeal Shock Wave Lithotripsy) | Stones 5-20 mm, proximal ureter or kidney |
| URS + Laser lithotripsy (Ureteroscopy) | Any ureteric stone, especially distal |
| PCNL (Percutaneous Nephrolithotomy) | Large renal stones >20 mm |
| DJ Stenting | To relieve obstruction while planning definitive treatment |
| Nephrostomy | Emergency decompression in infected/obstructed kidney |
Open surgery is now a final resort when all minimally invasive options have been exhausted - Comprehensive Clinical Nephrology, 7th Ed.
Long-Term Prevention (Stone Recurrence)
Since the patient is only 35 years old with likely right ureteric stone disease, prevention of recurrence is important:
| Measure | Detail |
|---|---|
| High fluid intake | >2.5 L urine output/day - single most effective prevention strategy |
| Low salt diet | <6 g NaCl/day |
| Citrate supplementation | Tab. Potassium citrate if urinary citrate is low (citrate inhibits stone formation) |
| Treat underlying cause | Hypercalciuria → Thiazide diuretics; Hyperuricosuria → Allopurinol; Hyperoxaluria → Dietary oxalate restriction |
| Alkalinization of urine | If uric acid stones: Tab. Sodium bicarbonate to keep urine pH >6.5 |
Summary Action Plan
TODAY:
✅ Urine routine + microscopy + culture
✅ Serum creatinine, calcium, uric acid
✅ If symptomatic: Tab. Diclofenac + Tab. Tamsulosin 0.4 mg OD
✅ Advise high fluid intake
IN 4-6 WEEKS:
✅ Repeat USG KUB - confirm resolution of right proximal ureteric dilatation
✅ 24-hour urine metabolic workup if recurrent or strong family history
REFER UROLOGY if:
⚠️ Symptoms persist >72 hours
⚠️ Fever/infection signs
⚠️ Rising creatinine
⚠️ Repeat imaging shows new/worsening hydronephrosis
Based on Brenner & Rector's The Kidney and Comprehensive Clinical Nephrology, 7th Ed. All treatment decisions must be made by the treating physician after clinical examination.
Patient has back pain and nausea
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Active Symptom Management for Miss Abhiruchi Sonkar
Why She Has Back Pain + Nausea — The Mechanism
The textbook explains this precisely:
"Renal colic pain occurs as the kidney stone is propelled through the ureter — a consequence of increased intraluminal pressure, causing stimulation of nerve endings in the ureteral mucosa. Pain originates in the back or flank, radiating around the torso to the groin. Renal colic can be associated with nausea and vomiting because the GI tract shares common innervation with the genitourinary system."
- Brenner & Rector's The Kidney
This is classic right ureteric colic - the back pain and nausea are both from the same cause: the right ureter being irritated/obstructed.
Immediate Treatment Protocol
🔴 Step 1 — Pain Relief (Most Important Right Now)
| Drug | Dose & Route | Notes |
|---|---|---|
| Inj. Diclofenac 75 mg | IM stat | First line - NSAIDs reduce intrarenal pressure and ureteral spasm; superior to opioids for colic |
| OR Tab. Diclofenac SR 75 mg | Oral if vomiting absent | Can be given orally if she can tolerate |
| OR Tab. Ketorolac 10 mg | Oral / IM | Faster onset NSAID alternative |
| Inj. Tramadol 100 mg | Slow IV in 100 mL NS | Add if NSAIDs alone insufficient (rescue analgesia) |
| Tab. Paracetamol 500 mg | Oral, 6-hourly | Mild background analgesic between doses |
⚠️ Avoid NSAIDs if: Gastric ulcer history, kidney function impaired, or patient is dehydrated
🟡 Step 2 — Nausea Control (Give First if Vomiting is Active)
| Drug | Dose & Route | Notes |
|---|---|---|
| Inj. Ondansetron 4 mg | IV / IM slow | First line antiemetic - 5-HT3 blocker, works fast |
| OR Tab. Ondansetron 4 mg | Oral/sublingual | If mild nausea without vomiting |
| Inj. Metoclopramide 10 mg | IV/IM | Alternative; also promotes gastric emptying |
| Inj. Promethazine 25 mg | Deep IM | If severe nausea with pain; added sedation helps |
Give antiemetic before or with analgesic - nausea must be controlled so oral medications can be taken
🔵 Step 3 — IV Fluids & Hydration
| Fluid | Amount | Purpose |
|---|---|---|
| IV NS or RL | 500-1000 mL over 1-2 hours | Rehydrate if vomiting, flush the urinary tract |
| Oral water | 2.5-3 L/day ongoing | Dilutes urine, promotes stone passage |
High fluid intake increases urine flow which helps push a small stone distally toward the bladder
🟢 Step 4 — Medical Expulsive Therapy (Start Today)
| Drug | Dose | Timing |
|---|---|---|
| Tab. Tamsulosin 0.4 mg | Once daily at bedtime | Relaxes right ureteral smooth muscle → helps stone pass |
- Cochrane review (67 studies, 10,509 patients) confirms alpha blockers shorten stone expulsion time
- Both AUA and EAU guidelines recommend tamsulosin for ureteral stones
- Continue for 4-6 weeks or until symptoms resolve
- Advise: may cause dizziness on standing - take at bedtime to minimize this
🔵 Step 5 — Antispasmodic
| Drug | Dose | Purpose |
|---|---|---|
| Tab. Hyoscine butylbromide (Buscopan) 10 mg | 3 times daily | Reduces ureteral smooth muscle spasm, decreases cramping pain |
| OR Tab. Drotaverine 80 mg | 3 times daily | Common in India for ureteric/intestinal spasm |
Prescription Summary (What to Write)
1. Inj. Ondansetron 4 mg IV stat (for nausea)
2. Inj. Diclofenac 75 mg IM stat (for pain)
3. IV NS 500 mL over 1 hour
4. Tab. Tamsulosin 0.4 mg HS (at bedtime) × 4 weeks
5. Tab. Drotaverine 80 mg TDS × 5 days
6. Tab. Ondansetron 4 mg TDS × 3 days (oral, after vomiting settles)
7. Tab. Diclofenac SR 75 mg BD after meals × 3-5 days
8. Tab. Pantoprazole 40 mg OD before breakfast
(always give PPI with NSAIDs to protect stomach)
9. Oral fluids: minimum 3 liters water daily
⚠️ Warning Signs — Admit/Refer Immediately If:
| Sign | Concern |
|---|---|
| Fever >38°C + back pain | Infected hydronephrosis / urosepsis - EMERGENCY |
| Pain not relieved after 2 doses of IV analgesic | Surgical intervention likely needed |
| Persistent vomiting (cannot take orals) | Hospital admission for IV management |
| Oliguria / no urine output | Bilateral obstruction or single kidney affected |
| Rising serum creatinine | Obstructive nephropathy |
Follow-Up Plan
| Timeline | Action |
|---|---|
| 24-48 hours | Review - is pain settling? Can she take orals? |
| 48-72 hours | If pain persists → urology referral for URS (ureteroscopy) |
| 2 weeks | Repeat urine routine to check for residual hematuria/infection |
| 4-6 weeks | Repeat USG KUB to confirm right proximal ureteric dilatation has resolved |
| After resolution | Urine metabolic workup (24-hour urine) to prevent recurrence |
Based on Brenner & Rector's The Kidney. All prescriptions to be administered by the treating physician (Dr. K.M. Chaudhary / Dr. Nilima Verma) after clinical examination.
Ureteroscopy
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Here is a complete guide to Ureteroscopy (URS) as it would apply to Miss Abhiruchi Sonkar's case, based on Hinman's Atlas of Urologic Surgery and Campbell-Walsh-Wein Urology.
Ureteroscopy (URS) — Complete Explanation
What is Ureteroscopy?
Ureteroscopy is a minimally invasive endoscopic procedure where a thin telescope (ureteroscope) is passed through the urethra → bladder → ureter to directly visualize, fragment, and remove a ureteral or renal stone. There is no incision - the scope travels through the body's natural passages.
Types of Ureteroscopes
| Type | Appearance | Used For |
|---|---|---|
| Semirigid ureteroscope | Thin, slightly bendable metal tube | Lower ureter (below iliac vessels) - best visualization + irrigation |
| Flexible ureteroscope | Fully bendable, steerable tip | Upper ureter, renal pelvis, all calyces - reaches anywhere |
For Miss Abhiruchi's right proximal ureteric location (above iliac vessels): flexible ureteroscopy is preferred, especially in females where semirigid can sometimes access proximal ureter too. - Hinman's Atlas of Urologic Surgery
Step-by-Step Procedure
Pre-operative Preparation
- Urine culture done and infection cleared (never proceed if pus/infection found - stent first, URS later)
- Antibiotics given before the procedure
- Patient under general or spinal anesthesia (regional preferred for better stone visualization)
- Patient positioned in lithotomy position (legs raised in stirrups)
- Foley catheter inserted, bladder drained
Step 1 — Cystoscopy & Ureteral Access
- Rigid cystoscope inserted through urethra into bladder
- The right ureteral orifice is identified at the trigone of the bladder
- A guidewire (hydrophilic tip) is passed through the ureteral orifice up into the right renal pelvis under fluoroscopic guidance
- A retrograde pyelogram is performed - contrast injected to map the stone location and collecting system anatomy
- A second safety guidewire is placed alongside the first
- The safety wire is critical - it maintains access if the scope needs to be withdrawn and a stent placed
"Ureteroscopy should not proceed without a safety wire, which provides access to the collecting system when a case is terminated early." - Hinman's Atlas
Step 2 — Ureteroscope Insertion
- The ureteroscope is passed alongside the safety wire, through the ureteral orifice and up the ureter
- If the ureteral orifice is too narrow: balloon dilation or serial dilators are used
- The scope is advanced carefully under direct vision + fluoroscopy until the stone is reached
Step 3 — Stone Visualization
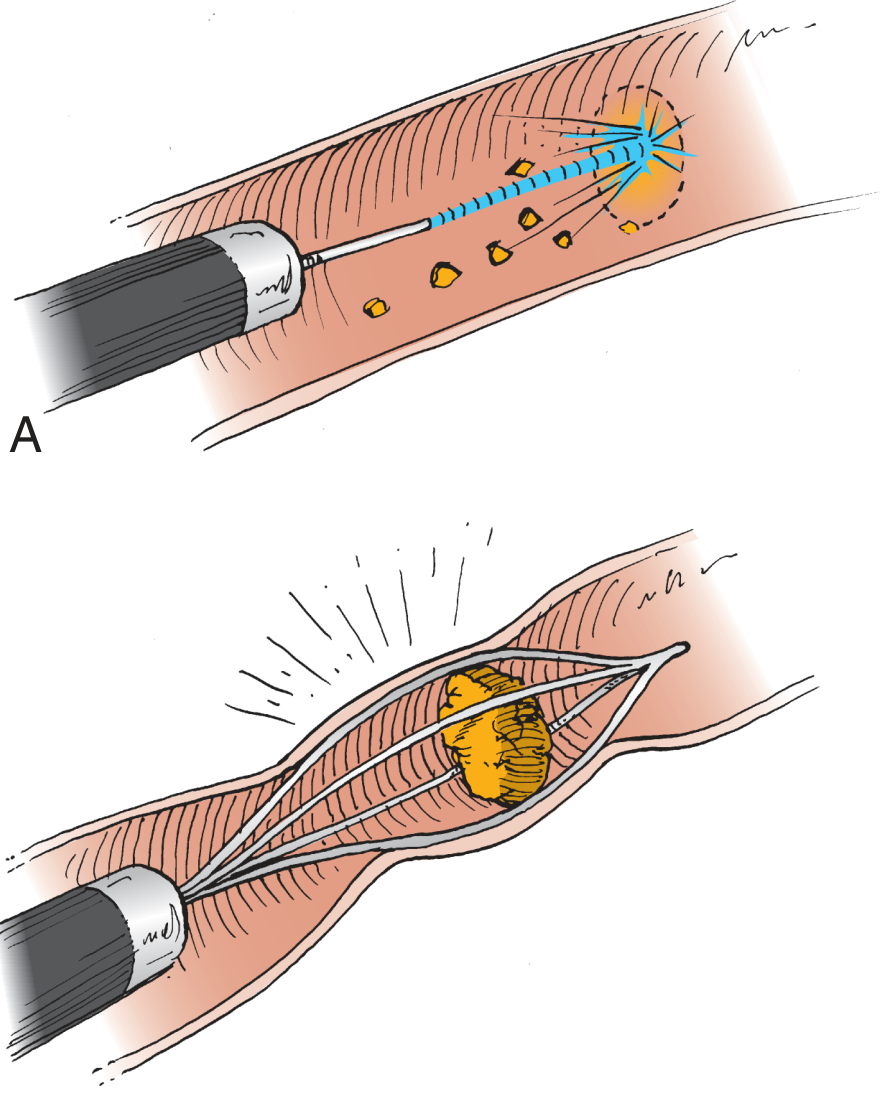
Figure shows (A) laser fiber fragmenting the stone into small pieces inside the ureter, and (B) basket device capturing and extracting a whole or fragmented stone.
- Stone is directly visualized through the ureteroscope's camera
- Stone characteristics (size, shape, color, hardness) are assessed
- An antiretropulsion device (stone cone/basket) may be placed just above the stone to prevent it from being pushed back up into the kidney during fragmentation
Step 4 — Stone Fragmentation (Lithotripsy)
This is the core step - breaking the stone:
| Method | How it Works | Notes |
|---|---|---|
| Ho:YAG Laser (Holmium laser) ⭐ | Laser fiber vaporizes stone on contact | Gold standard - works on ALL stone types, flexible fiber, minimal tissue damage, least retropulsion |
| Pneumatic/Ballistic lithotripsy | Probe fires mechanical impulses like a jackhammer | Effective but causes stone retropulsion in 40% of proximal stones |
| Electrohydraulic (EHL) | Electrical spark creates shockwaves | Older technique, higher perforation risk |
| Ultrasonic | High-frequency vibration | Good for soft stones, requires larger scope channel |
"Ho:YAG laser is clearly the current most efficacious and safe laser available... we recommend Ho:YAG as the first-line option." - Hinman's Atlas
Success rates with laser: Stones ≤10 mm: 91-97% stone-free. Stones >10 mm: 71-89% stone-free - Campbell-Walsh-Wein Urology
Step 5 — Fragment Extraction
- Small fragments (<2 mm) are washed out with irrigation fluid ("dusting" technique)
- Larger fragments are grasped with a stone basket or grasping forceps and removed
- Caution: never basket a stone too large for the ureter - risk of ureteral avulsion
Step 6 — DJ Stent Placement (Post-procedure)
After stone clearance, a Double-J (DJ) ureteral stent is placed in most cases:
Kidney (upper J curl) ←— stent ——→ Bladder (lower J curl)
| Why a DJ stent is placed | Details |
|---|---|
| Prevents post-op ureteral swelling/obstruction | Ureter gets swollen after manipulation |
| Allows drainage if residual fragments present | Fragments can obstruct |
| Aids healing if ureteral injury occurred | Splints the ureter |
| Promotes stone fragment passage | Keeps ureter patent |
- Stent duration: Usually 1-4 weeks, then removed via cystoscopy
- Stentless URS is possible in uncomplicated low-risk cases
"A double pigtail ureteral stent can then be placed. Stentless ureteroscopy is an option in uncomplicated, low-risk patients." - Hinman's Atlas
Step 7 — Post-procedure
- Recovery: few hours in hospital, often day-care procedure
- Discharge: same day or next day
- Expects: blood-tinged urine for 2-3 days (normal), mild burning, frequent urination
- Return to work: 2-5 days
Indications for URS (When to Do It)
| Indication | Detail |
|---|---|
| Ureteral stone, any size | Most common indication - first line for all ureteral stones |
| Stone not passing after 4-6 weeks of conservative treatment | Failed medical management |
| Pain not controlled by analgesics >72 hours | |
| Obstruction with fever/infection | Emergency URS or stenting |
| Stone >10 mm (unlikely to pass spontaneously) | |
| Patient preference (wants quick definitive treatment) | |
| Pregnancy with symptomatic ureteral stone | URS is safest option |
Contraindications
| Contraindication | Reason |
|---|---|
| Untreated urinary tract infection | Risk of sepsis - stent first, treat infection, URS later |
| Uncorrected coagulopathy | Bleeding risk |
| Severe urethral/ureteral stricture preventing access | May need dilation first |
| Active pyelonephritis | Emergency decompression first |
Complications
| Complication | Incidence | Management |
|---|---|---|
| Hematuria | Very common (expected) | Self-limiting, resolves in 2-3 days |
| UTI / Fever | 2-5% | Antibiotics |
| Ureteral perforation | 1.4% | DJ stent placement, usually heals |
| Stone retropulsion | 10-40% | Stone pushed to kidney - may need ESWL or PCNL |
| Ureteral stricture (late) | <1% | Balloon dilation or reconstructive surgery |
| Ureteral avulsion (rare) | <0.1% | Emergency surgery - most feared complication |
| Stent symptoms | Common | Frequency, urgency, mild pain - resolves after stent removal |
"Complications include ureteral avulsion, perforation, extravasation, mucosal damage, hematuria, infection, and stricture. Advances in laser technology reduce the need for graspers and baskets and hence reduce complications." - Comprehensive Clinical Nephrology, 7th Ed.
URS vs Other Treatments — When to Choose What
| Stone Characteristic | Best Treatment |
|---|---|
| Ureteral stone, any size | URS (first line) |
| Non-lower pole renal stone <20 mm | ESWL or URS |
| Non-lower pole renal stone >20 mm | PCNL |
| Lower pole stone <10 mm | ESWL or URS |
| Lower pole stone >10 mm | PCNL or URS |
| Staghorn calculus | PCNL |
Based on AUA/Endourological Society Guidelines 2016 - Comprehensive Clinical Nephrology, 7th Ed.
Relevance to Miss Abhiruchi Sonkar
| Factor | Status |
|---|---|
| Stone confirmed on NCCT? | ❌ Not confirmed - NCCT normal |
| Current symptoms | ✅ Back pain + nausea (active colic) |
| Should URS be done now? | Not yet - attempt conservative treatment (tamsulosin + analgesics) for 4-6 weeks first per AUA guidelines |
| Trigger for URS | If symptoms persist >72 hours despite analgesics OR repeat USG shows worsening hydronephrosis |
| If URS needed | Right-sided, likely proximal → flexible URS + Ho:YAG laser preferred |
Source: Hinman's Atlas of Urologic Surgery; Campbell-Walsh-Wein Urology; Comprehensive Clinical Nephrology 7th Ed. (AUA/EAU Guidelines)
Hematuria
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Here is a complete, structured explanation of hematuria, directly relevant to Miss Abhiruchi Sonkar's case.
Hematuria — Complete Guide
Definition
Hematuria = presence of blood (red blood cells) in the urine.
| Type | Definition | Patient Awareness |
|---|---|---|
| Gross (Macroscopic) Hematuria | Urine visibly red, pink, or brown | Patient sees it - alarming |
| Microscopic Hematuria (MH) | Invisible to naked eye; detected on urine test | ≥3 RBCs per high-power field (HPF) on microscopy |
"Hematuria is a concerning urologic sign in adults and must be evaluated because it may signal the presence of a urologic cancer in up to 25% of patients."
- Campbell-Walsh-Wein Urology
In Miss Abhiruchi's Context
She has right ureteric dilatation + back pain + nausea. Hematuria here is:
- Expected as a confirmatory sign of ureteric stone/colic
- If present on urine microscopy = strongly supports stone disease diagnosis
- If absent = does NOT rule out stone (hematuria is absent in ~15-20% of confirmed stone cases)
Causes of Hematuria — Full Classification
A. Urological (Non-Glomerular) Causes
RBCs are normal shape (eumorphic)
| Category | Specific Causes |
|---|---|
| Stones (Most likely in this patient) | Ureteric calculus, renal calculus, bladder stone - stone trauma to urothelium causes bleeding |
| Infection | UTI, cystitis, pyelonephritis, urethritis, TB of urinary tract |
| Tumors | Bladder cancer (most common cause of gross hematuria in >50 years), renal cell carcinoma, ureteric TCC, prostate cancer |
| Trauma | Kidney injury, urethral trauma, post-catheterization, post-URS (expected) |
| Benign conditions | BPH (benign prostatic hyperplasia), renal cysts, vascular malformations, nutcracker syndrome |
| Drugs | Cyclophosphamide (hemorrhagic cystitis), anticoagulants (warfarin), NSAIDs |
| Exercise-induced | Vigorous physical activity - resolves within 24-48 hours |
B. Nephrological (Glomerular) Causes
RBCs are dysmorphic (distorted) on microscopy; often + proteinuria
| Condition | Features |
|---|---|
| IgA nephropathy (Berger's disease) | Most common glomerular cause; hematuria after URTI |
| Thin Basement Membrane Disease | Persistent microscopic hematuria; benign prognosis |
| Alport syndrome | Hereditary nephritis + sensorineural deafness |
| Post-streptococcal GN | 2-3 weeks after throat/skin infection; tea-colored urine |
| Lupus nephritis | + systemic lupus features |
C. Systemic / Other Causes
| Cause | Detail |
|---|---|
| Bleeding disorders | Hemophilia, thrombocytopenia, DIC |
| Sickle cell disease | RBC sickling in renal medulla |
| Endometriosis | Cyclical hematuria (rare) |
| Pseudohematuria | Beets, rifampicin, myoglobinuria - red urine but NO RBCs on microscopy |
How to Distinguish the Cause — Urine Microscopy is Key
| Finding on Microscopy | Suggests |
|---|---|
| Normal (eumorphic) RBCs | Urological cause (stone, tumor, infection) |
| Dysmorphic RBCs (acanthocytes) | Glomerular cause (nephritis) |
| RBC casts | Definitive glomerulonephritis |
| WBC casts | Pyelonephritis / interstitial nephritis |
| Proteinuria + dysmorphic RBCs | Refer to nephrologist |
| Bacteria + WBCs | UTI - treat, then retest |
Stream of Hematuria Tells the Location
"Initial stream hematuria = prostatic/urethral source; Terminal hematuria = bladder neck; Total stream hematuria = bladder or upper tract"
- Campbell-Walsh-Wein Urology
| Hematuria Timing | Source |
|---|---|
| Initial stream | Urethra, prostate |
| Terminal (end of stream) | Bladder neck, trigone |
| Total stream (throughout) | Bladder, ureter, kidney - most clinically significant |
| With clots - vermiform (worm-shaped) | Upper tract (kidney/ureter) |
| With clots - cuboid/irregular | Bladder |
Clot Shape Clue
"Clots formed in the upper tract often have a vermiform (worm-shaped) shape; cuboid clots are likely produced in the bladder."
- Campbell-Walsh-Wein Urology
Evaluation Protocol — AUA Guidelines
The evaluation follows three pillars:
Pillar 1 — History & Physical
Key questions to ask:
- Duration and onset of hematuria
- Associated symptoms: pain, fever, burning, frequency, urgency
- Smoking history (bladder cancer risk)
- Chemical/industrial exposure (aromatic amines → bladder cancer)
- Family history of kidney disease, polycystic kidneys, VHL syndrome
- Drug history (anticoagulants, cyclophosphamide)
- Recent exercise, menstruation, trauma, catheterization
Pillar 2 — Laboratory Tests
| Test | Purpose |
|---|---|
| Urine routine + microscopy | Confirm true hematuria (RBCs vs pseudohematuria); dysmorphic cells vs eumorphic; casts; WBCs |
| Urine dipstick | Screening only - NOT sufficient alone (false positives from myoglobin/hemoglobin) |
| Urine culture | Rule out infection - treat UTI, retest urine |
| Serum creatinine | Assess kidney function; guides imaging choice |
| Urine cytology | If high-risk for urothelial malignancy (smoker, industrial exposure, >35 years) |
| Urine calcium, uric acid | If stone disease suspected |
| PT/INR | If anticoagulants |
"The urine dipstick alone is NOT sufficient for determining true hematuria - always confirm with microscopy." - Campbell-Walsh-Wein Urology
Pillar 3 — Imaging + Cystoscopy
| Investigation | When |
|---|---|
| NCCT KUB (done ✅) | Best for stones - already performed, normal |
| CT Urography (CTU) | Gold standard for hematuria workup - detects stones, tumors, vascular lesions; 97% sensitivity for upper tract urothelial cancers |
| Ultrasound (done ✅) | Good for renal masses, hydronephrosis - already done |
| Cystoscopy | Mandatory in gross hematuria or in patients >35 years with risk factors - directly visualizes bladder for tumors, carcinoma in situ, polyps |
| Retrograde pyelogram | If upper tract TCC suspected and CT insufficient |
| Kidney biopsy | If glomerular hematuria suspected (dysmorphic RBCs + proteinuria + nephrological symptoms) |
Hematuria in Stone Disease — Specifically
| Feature | Detail |
|---|---|
| Mechanism | Stone scrapes/traumatizes urothelial lining of ureter → capillary rupture → RBCs leak into urine |
| Type | Total stream hematuria (throughout void) |
| Amount | Usually microscopic; occasionally macroscopic (red/pink urine) |
| Associated symptoms | Flank pain, nausea, vomiting - exactly as in this patient |
| Significance | In the context of colic → confirms stone passage / ureteric injury |
| After stone passes | Hematuria resolves within 24-72 hours |
| After URS | Expect blood-tinged urine for 2-3 days (normal, expected complication) |
When is Hematuria an Emergency?
| Situation | Action Needed |
|---|---|
| Gross hematuria + clot retention (cannot pass urine) | Emergency - bladder irrigation + urology |
| Hematuria + fever + flank pain | Infected obstructed kidney - emergency decompression |
| Painless gross hematuria (no infection, no stone) | Urgent urology referral - bladder/kidney cancer until proven otherwise |
| Hematuria + rising creatinine | Glomerulonephritis or obstructive nephropathy - urgent nephrology |
| Hematuria in post-URS patient + heavy bleeding | Arteriovenous fistula or ureteral injury - urgent radiology/urology |
What to Do Now for Miss Abhiruchi
Given her symptoms (back pain + nausea + likely ureteric colic):
1. Urine routine + microscopy — STAT
→ If ≥3 RBCs/HPF with eumorphic cells = confirms ureteric stone/colic
→ If dysmorphic RBCs + proteinuria = refer nephrology
→ If WBCs + bacteria = UTI, treat first
2. Urine culture — send simultaneously
→ Essential before any procedure (URS)
3. Serum creatinine — assess right kidney function
4. If gross hematuria with clots → urgent urology referral
5. If microscopic hematuria resolves with stone treatment → no further hematuria workup needed
6. If hematuria persists after stone treatment resolves → full AUA hematuria evaluation including cystoscopy
Key Points Summary
- Hematuria in this patient is almost certainly from right ureteric stone injury (eumorphic RBCs, associated colic)
- Urine microscopy confirms and characterizes it - always do microscopy, not just dipstick
- Stone-related hematuria resolves with stone treatment
- Painless gross hematuria in any patient = bladder cancer until proven otherwise - this is the most important alarm signal
- AUA guidelines mandate complete evaluation even if one cause is found - other causes (tumor, glomerular) must be excluded if hematuria persists
Source: Campbell-Walsh-Wein Urology; Brenner & Rector's The Kidney; Textbook of Family Medicine 9th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.