Bernoulis in MD anaesthesia . Give an exam ready answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have all the material needed for a complete exam-ready answer. Here it is:
Bernoulli's Principle in Anaesthesia
Definition and Basic Physics
Bernoulli's principle states that for steady (non-turbulent), incompressible fluid flow, the total mechanical energy per unit volume is constant along a streamline. When a fluid passes through a constriction (narrowing), its velocity increases and its lateral (static) pressure decreases proportionally, so that the sum of kinetic energy and potential (pressure) energy is conserved.
The equation:
P₁ + ½ρv₁² = P₂ + ½ρv₂²
Where:
- P = pressure
- ρ = fluid density
- v = velocity
At the constriction: v increases → P falls. Downstream where the tube widens: v falls → P recovers. The pressure drop due to kinetic energy conversion is reversible, unlike that due to frictional resistance (which is irreversible and dissipated as heat) - Ganong's Review of Medical Physiology.
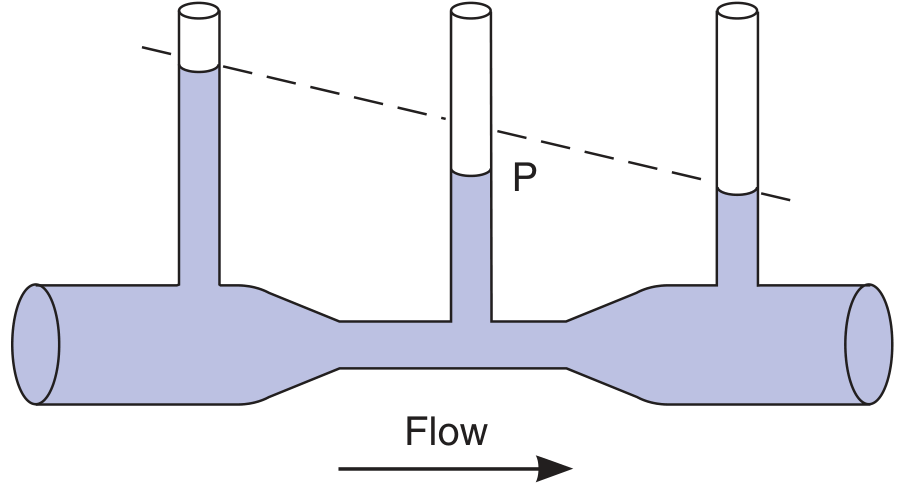
FIGURE: Bernoulli principle. When fluid flows through the narrow portion of the tube, kinetic energy increases as velocity increases, and potential energy (measured pressure P) is reduced. The dashed line shows what the pressure drop due to friction alone would have been in a uniform tube. - Ganong's Review of Medical Physiology, 26th ed.
Applications in Anaesthesia
1. Venturi Mask (Controlled FiO₂ Delivery)
The Venturi mask (Campbell, 1967) is the classic clinical application of Bernoulli's principle. 100% O₂ is driven through a narrow jet/channel. The high-velocity jet creates a zone of low lateral pressure at the constriction, which entrains ambient air through side apertures.
- By varying the diameter of the jet and the size of the entrainment apertures, a precise and fixed oxygen:air ratio is delivered.
- Available FiO₂ range: 24-50% (colour-coded entrainment connectors)
- Total flow delivered: 50-70 L/min - far exceeding patient's peak inspiratory flow, ensuring FiO₂ is independent of tidal volume and respiratory pattern
- Clinical use: First-line oxygen therapy in patients at risk of hypercapnia (COPD), where precise FiO₂ titration is essential - Murray & Nadel's Respiratory Medicine
Key point for exams: The Venturi mask delivers a fixed FiO₂ because the entrainment ratio is fixed by the device geometry, not by the patient's breathing pattern.
2. Rotameter (Constant-Pressure, Variable-Orifice Flowmeter)
The Thorpe tube rotameter on anaesthesia machines operates on Bernoulli's principle.
- A float (bobbin/ball) is suspended in a vertically tapered glass tube
- Gas flows upward; as flow increases, the float rises to a wider part of the tube (increasing the annular orifice)
- The pressure drop across the float remains constant regardless of flow rate (constant-pressure, variable-orifice)
- The float rises until its weight is just balanced by the pressure difference (constant pressure drop = float weight / cross-sectional area)
- At the annular gap around the float, velocity is high and lateral pressure is low (Bernoulli) - this pressure differential supports the float
Calibration note: At low flows, flow is laminar and the flowmeter is calibrated for gas viscosity (Poiseuille's law). At high flows, flow becomes turbulent and the meter is calibrated for gas density (Bernoulli/Torricelli). Each flowmeter is therefore gas-specific. - Morgan & Mikhail's Clinical Anesthesiology, 7e
Safety feature: Oxygen flowmeter is positioned furthest downstream (rightmost, nearest to the vaporizer) so that a leak in an upstream flowmeter does not produce a hypoxic mixture.
3. Venturi Injector / Jet Ventilation
Used in high-frequency jet ventilation (HFJV) and Sanders injector for laryngoscopy/airway surgery:
- A high-pressure jet of oxygen is passed through a narrow nozzle into the airway
- The resulting high velocity creates low lateral pressure (Bernoulli), entraining ambient air/anaesthetic gases into the airway alongside the jet
- This produces ventilation without an endotracheal tube, making it useful for laryngeal and subglottic surgery, rigid bronchoscopy, and laser procedures
- Scott-Brown's (ENT) describes supraglottic or transtracheal jet ventilation using this principle for endolaryngeal surgery
4. Nebulizers
Pneumatic nebulizers use Bernoulli's principle:
- A high-velocity gas jet passes across the tip of a liquid feed tube
- Low lateral pressure created at the jet tip draws liquid upward (Venturi/Bernoulli effect)
- The entrained liquid is then shattered into fine aerosol particles by the gas stream
- Used in delivery of bronchodilators, antibiotics, and humidification circuits
5. Echocardiographic Bernoulli Equation (Relevant to Anaesthesia - TOE/TEE)
Bernoulli's principle forms the basis of Doppler echocardiographic pressure gradient estimation, highly relevant in perioperative TOE/TEE:
The modified (simplified) Bernoulli equation:
ΔP = 4V²
Where:
- ΔP = transvalvular pressure gradient (mmHg)
- V = peak jet velocity (m/s) by continuous-wave Doppler
Full form (when proximal velocity V₁ > 1.5 m/s):
ΔP = 4(V₂² - V₁²)
Applications in perioperative TOE:
- Quantify severity of aortic stenosis (peak and mean gradient across aortic valve)
- Assess mitral stenosis gradient
- Estimate pulmonary artery systolic pressure from tricuspid regurgitation jet: PASP = 4(V_TR)² + RA pressure
- Assess severity of valvular regurgitation
- Identify intracardiac shunts and estimate chamber pressures
Note: If V₁ < 1.5 m/s it is usually ignored. If V₁ exceeds 1.5 m/s it must be included. - Miller's Anesthesia, 10e
6. Pathophysiological Relevance
- Arterial stenosis (atherosclerotic plaque): At a stenosis, velocity increases → lateral pressure falls → vessel wall is at risk of collapse, and the narrowing tends to be self-perpetuating (Bernoulli collapse phenomenon) - Ganong's
- Paediatric airway (subglottic oedema/croup): The narrow subglottis already generates high-velocity, low-pressure flow. Oedema further narrows the lumen → velocity rises further → wall-distending pressure falls even more → the airway tends toward dynamic collapse during inspiration (important consideration in paediatric anaesthesia) - Scott-Brown's
- Airway collapse in obstructive sleep apnoea: Supraglottic collapse during apnoeas is partly mediated by the Bernoulli effect at the narrow pharynx
Summary Table
| Application | Gas/Fluid | Bernoulli Effect | Clinical Outcome |
|---|---|---|---|
| Venturi mask | O₂ jet | Low pressure entrains air | Fixed FiO₂ delivery |
| Rotameter (Thorpe tube) | Anaesthetic gas | Pressure drop across float constant | Accurate flow measurement |
| Jet ventilator/Sanders injector | O₂ jet | Entrains air into airway | Tubeless ventilation |
| Pneumatic nebulizer | Driving gas | Liquid entrained by low pressure | Aerosol drug delivery |
| TOE/Doppler (ΔP = 4V²) | Blood | Velocity → pressure conversion | Non-invasive gradient estimation |
| Arterial stenosis/croup | Blood/air | Velocity ↑ → pressure ↓ | Vessel/airway collapse |
Exam Mnemonics
"VeRNe JNeP" - Venturi mask, Rotameter, Nebulizer, Jet ventilator, Narrow airway pathology, echocardiography (TEE/ΔP=4V²)
Key distinction to remember: Bernoulli applies to laminar, incompressible, steady flow of ideal fluids. In the real anaesthetic context, Poiseuille's law (resistance to laminar flow, viscosity-dependent) and turbulent flow considerations modify pure Bernoulli behaviour - which is why flowmeters must be calibrated separately for each gas at different flow ranges.
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e | Miller's Anesthesia 10e | Murray & Nadel's Respiratory Medicine | Ganong's Review of Medical Physiology 26e | Scott-Brown's Otolaryngology
Triage in management of trauma patients in MD Anaesthesia
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
I now have comprehensive, textbook-sourced material. Here is the complete exam-ready answer:
Triage in Management of Trauma Patients
Definition
Triage (from French trier - to sort) is the systematic process of sorting and prioritizing multiple casualties according to the urgency of their injuries and the likelihood of survival, so that available resources - personnel, equipment, operating rooms - are allocated to produce the greatest benefit for the greatest number of patients.
The three guiding ATLS principles underlying all triage decisions are:
- Treat the greatest threat to life first
- The lack of a definitive diagnosis must never impede indicated treatment
- A detailed history is not essential to begin trauma evaluation
- Tintinalli's Emergency Medicine
Types of Triage
A. Routine (Everyday) Triage - Single/Few Patients
Used when resources are adequate. Priority is given to the most critically injured regardless of resource use. The anaesthesiologist focuses on:
- Airway assessment and intervention
- Haemodynamic status and resuscitation needs
- Operating room (OR) prioritization
B. Mass Casualty Incident (MCI) Triage
When casualties overwhelm available resources, the goal shifts from "do everything for the most critically injured" to "do the most good for the most patients." Resources are directed to those most likely to survive.
Triage Systems
1. START Triage (Simple Triage and Rapid Treatment)
Most widely used field triage system. Can be completed in <30 seconds per patient.
Assessment sequence: RPM - Respiration, Perfusion, Mental status
| Category | Colour | Criteria | Action |
|---|---|---|---|
| Immediate | Red | RR >30/min OR capillary refill >2 s OR unable to follow commands | Treat first |
| Delayed | Yellow | Ambulatory with minor injury; stable vitals | Can wait up to 1 hour |
| Minimal | Green | Walking wounded; minor injuries | Self-care/delayed |
| Expectant | Black | Apnoeic (no breath after airway repositioning); no pulse | Expectant/comfort only |
| Dead | Black | No signs of life | No intervention |
2. SALT Triage (Sort, Assess, Lifesaving interventions, Treatment/Transport)
CDC-endorsed system for MCI. More comprehensive than START.
Five categories:
- Immediate (Red): Non-ambulatory; deranged respiration, perfusion, or mental status. Requires: airway opening, tourniquet, chest decompression
- Delayed (Yellow): Significant injuries but care can wait up to 1 hour
- Minimal (Green): Ambulatory, minor injuries, may self-help
- Expectant (Gray): Highly likely to die imminently even with immediate care; still deserving of comfort and compassion
- Dead (Black): No signs of life
3. RAMP (Rapid Assessment of Mentation and Pulse)
Simplified alternative to START; assesses only mentation + pulse.
National Field Triage Guidelines (4-Step Algorithm)
The CDC/ATLS field triage decision scheme is a 4-step sequential assessment:
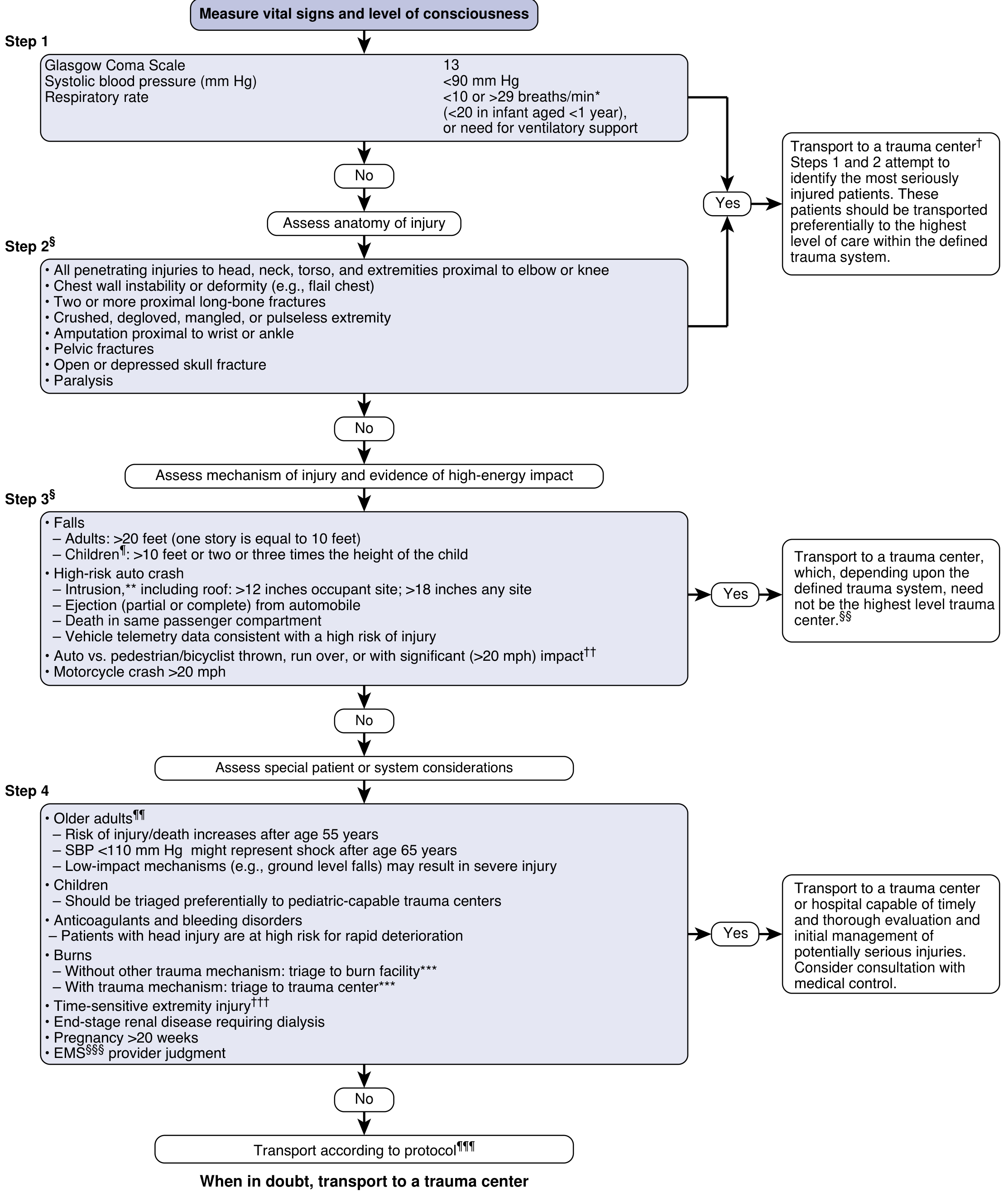
Step 1 - Vital Signs and Level of Consciousness (Highest priority):
- GCS <13
- SBP <90 mmHg
- RR <10 or >29/min → Transport to highest-level trauma centre
Step 2 - Anatomy of Injury:
- Penetrating injury to head/neck/torso/proximal extremities
- Flail chest, pelvic fracture, skull fracture/paralysis
- Two or more proximal long bone fractures
- Crushed/pulseless/mangled extremity, amputation → Highest-level trauma centre
Step 3 - Mechanism of Injury (High-energy impact):
- Falls >20 feet (adults), >10 feet (children)
- High-risk auto crash: ejection, intrusion >12 inches, death in same compartment
- Pedestrian/cyclist struck at >20 mph → Trauma centre (need not be highest level)
Step 4 - Special Considerations:
- Age >55 years: SBP <110 mmHg may indicate shock
- Children: triage to paediatric-capable trauma centre
- Anticoagulant use, pregnancy >20 weeks, burns with trauma → Appropriate trauma centre with EMS judgment
"When in doubt, transport to a trauma centre" - Current Surgical Therapy, 14e
Trauma Scoring Systems Used in Triage
Physiologic Scores
| Score | Components | Range | Purpose |
|---|---|---|---|
| Revised Trauma Score (RTS) | GCS + SBP + RR (coded 0-4 each) | 0-12 | Field triage; predicts survival probability |
| Glasgow Coma Scale (GCS) | Eye (4) + Verbal (5) + Motor (6) | 3-15 | Neurological triage; motor component most predictive |
| New Trauma Score (NTS) | Actual GCS + coded SBP + SpO₂ | - | Improved physiologic scoring |
Revised Trauma Score coding:
| Parameter | 4 | 3 | 2 | 1 | 0 |
|---|---|---|---|---|---|
| GCS | 13-15 | 9-12 | 6-8 | 4-5 | 3 |
| SBP (mmHg) | >89 | 76-89 | 50-75 | 1-49 | 0 |
| RR (/min) | 10-29 | >29 | 6-9 | 1-5 | 0 |
RTS <11 → transport to Level I trauma centre
Anatomic Scores
- Abbreviated Injury Scale (AIS): Grades individual injury 1 (minor) to 6 (unsurvivable)
- Injury Severity Score (ISS): Sum of squares of three highest AIS scores from different body regions. Range 1-75. ISS >15 = major trauma (Level I centre)
- Trauma Mortality Prediction Model (TMPM): ICD-based; predicts survival more accurately than ISS
Combined Score
- TRISS (Trauma and Injury Severity Score): Combines RTS + ISS + age + mechanism → probability of survival (Ps). Used for audit and benchmarking.
ATLS Primary Survey - The Anaesthesiologist's Priority Framework
The primary survey with simultaneous resuscitation forms the cornerstone of trauma triage at the hospital level:
ABCDE + F:
| Step | Assessment | Immediately Life-Threatening Conditions |
|---|---|---|
| A - Airway + C-spine | Patency, obstruction | Foreign body, angioedema, fracture, burns |
| B - Breathing | Rate, SpO₂, chest movement | Tension pneumothorax, open pneumothorax, flail chest, haemothorax |
| C - Circulation | Pulse, BP, CRT, haemorrhage | Massive haemorrhage (external/internal), cardiac tamponade |
| D - Disability | GCS, pupils, AVPU | TBI, spinal cord injury |
| E - Exposure | Head-to-toe exam | Any missed injuries |
| F - FAST/Foley | FAST USG, urinary output | Intra-abdominal/pericardial blood |
After primary survey: secondary survey (detailed head-to-toe), then tertiary survey (once stabilized, 24-48 h, to detect missed injuries) - Miller's Anesthesia, 10e; Schwartz's Principles of Surgery
Trauma Centre Level Designation
| Level | Capabilities | Requirement |
|---|---|---|
| I | Highest; 24-h in-house senior surgeon, anaesthesiologist, neurosurgeon; research & education | Major urban/academic centre |
| II | 24-h availability; all specialties; may transfer complex cases | Community trauma centre |
| III | Prompt assessment/resuscitation; transfers critical cases | Rural/community hospital |
| IV | Basic stabilization; transfer to higher centre | Remote settings |
- Tintinalli's Emergency Medicine
Role of the Anaesthesiologist in Trauma Triage
- Prehospital liaison: Receives information via D-MIST handoff (Demographics, Mechanism, Injuries, Signs, Treatment given) from EMS; activates appropriate OR and personnel
- Airway triage: First to identify impending airway catastrophe - intubation, surgical airway
- Haemodynamic assessment: Guides initial resuscitation; recognizes occult shock (shock index HR/SBP >1 = concern)
- OR prioritization in multiple casualties: Decides order of patients for surgery based on physiologic stability, injury pattern, and damage control principles
- Damage Control Resuscitation (DCR):
- Permissive hypotension (SBP 80-90 mmHg) until surgical haemostasis in penetrating trauma
- Haemostatic resuscitation: 1:1:1 PRBC:FFP:platelets
- Avoid crystalloid excess
- Damage Control Surgery (DCS) over Early Total Care: In severely compromised patients, supports abbreviated surgery (pack and control haemorrhage, temporize) followed by ICU resuscitation and planned re-look. Prolonged procedures in the "lethal triad" (hypothermia, acidosis, coagulopathy) worsen outcomes - Bailey & Love's Surgery
The Lethal Triad - Triage Urgency Signal
When any two of the three are present, the patient requires immediate damage control (not definitive repair):
Hypothermia
/\
/ \
/ \
Acidosis ------ Coagulopathy
Each element worsens the other two. The anaesthesiologist must recognize and break this cycle by prioritizing rapid haemostasis over definitive reconstruction.
Special Triage Considerations
| Population | Key Adjustment |
|---|---|
| Elderly (>55 yr) | SBP <110 may indicate shock; even "low-energy" falls can cause severe injury; age alone worsens outcome |
| Children | Triage to paediatric trauma centre; SBP threshold: <70 + (2 × age in years) |
| Pregnancy >20 wk | Maternal resuscitation = foetal resuscitation; left lateral tilt; neonatology team alert |
| Anticoagulated patients | Head injuries have high risk of rapid deterioration; lower threshold for CT/neurosurgery |
| Burns + trauma | If burn is greater threat → burn centre; if non-burn injury greater threat → trauma centre first |
Psychological/Ethical Dimension of MCI Triage
- Expectant category: The decision to withhold intervention from salvageable-looking but non-survivable patients is ethically the hardest aspect of MCI triage. It requires specific training.
- Critical Incident Stress Management (CISM): Must be planned in advance; tools like Psy-START help psychological triage post-event
- Austere environments: Tactical EMS (TEMS) teams operate in hostile environments; scene safety always before patient access - Rosen's Emergency Medicine
Summary Flow for Exam
SCENE → Field Triage (START/SALT) → Transport Decision (Trauma Level)
↓
HOSPITAL → Primary Survey (ABCDE) + Simultaneous Resuscitation
↓
Life-threatening injury identified? → IMMEDIATE intervention
↓
Secondary Survey + Adjuncts (FAST, X-ray, CT)
↓
Scoring (GCS, RTS, ISS, TRISS) → Audit/Outcome
↓
OR Prioritization → Damage Control Surgery vs Early Total Care
↓
ICU → Tertiary Survey (24-48 h)
Sources: Miller's Anesthesia 10e | Tintinalli's Emergency Medicine | Rosen's Emergency Medicine | Current Surgical Therapy 14e | Schwartz's Principles of Surgery 11e | Sabiston Textbook of Surgery | Bailey & Love's Short Practice of Surgery 28e
Oxygen vacuum insulated vaporater in md Anaesthesia
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
vacuum insulated evaporator VIE oxygen anaesthesia MD exam construction principle safety
Reading File
Searching the Web
VIE vacuum insulated evaporator hospital oxygen supply anaesthesia physics construction working principle
Reading Web Page
https://anaesthetics.ukzn.ac.za/wp-content/uploads/2024/03/2…
I now have comprehensive material from multiple authoritative sources. Here is the complete exam-ready answer:
Oxygen - Vacuum Insulated Evaporator (VIE)
Definition
A Vacuum Insulated Evaporator (VIE) is a large cryogenic bulk storage vessel used to store liquid oxygen at hospitals. It functions as the primary oxygen supply for hospital pipeline systems, including those feeding anaesthetic machines in operating theatres. It is essentially a giant thermos flask that maintains oxygen in its liquid state at very low temperatures and moderate pressure.
Properties of Oxygen Relevant to VIE
Before understanding the VIE, key physical properties of oxygen must be understood:
| Property | Value |
|---|---|
| Molecular weight | 32 g/mol |
| Boiling point at 1 atm | -183°C |
| Critical temperature | -118°C |
| Critical pressure | 50.1 bar |
| Colour | Colourless (pale blue as liquid) |
| Density | 1.4 times heavier than air |
| State at room temperature and pressure | Gas (above critical temperature) |
Critical temperature is the temperature above which a substance cannot be liquefied by pressure alone. Oxygen's critical temperature is -118°C - this is a key exam fact. At room temperature (25°C), oxygen is well above its critical temperature, meaning it cannot be stored as a liquid at room temperature regardless of the pressure applied. This is why cryogenic storage is required.
Key distinction:
- Nitrous oxide (critical temperature +36.5°C) can be stored as a liquid at room temperature under pressure in cylinders
- Oxygen cannot - it must be stored below -118°C to exist as a liquid
- This is why the VIE is necessary and why oxygen cylinders contain compressed gas, not liquid
Construction of the VIE
The VIE is designed like a very large, high-performance thermos flask:
┌─────────────────────────────┐
│ OUTER SHELL (Carbon Steel) │
│ ┌─────────────────────────┐ │
│ │ VACUUM SPACE │ │ ← ~0.3 kPa vacuum
│ │ ┌───────────────────┐ │ │ (excellent insulator)
│ │ │ INNER SHELL │ │ │
│ │ │ (Stainless Steel) │ │ │
│ │ │ │ │ │
│ │ │ VAPOUR PHASE ↑ │ │ │ ← Gaseous O₂ at top
│ │ │ ───────────── │ │ │
│ │ │ LIQUID PHASE │ │ │ ← Liquid O₂ at bottom
│ │ │ at -150 to -180°C│ │ │
│ │ └───────────────────┘ │ │
│ └─────────────────────────┘ │
└─────────────────────────────┘
Structural Components:
- Inner vessel - stainless steel; contains liquid oxygen
- Outer jacket - carbon steel; structural support
- Vacuum space between the two shells - the key insulating layer (~0.3 kPa vacuum). The vacuum virtually eliminates conductive and convective heat transfer (same principle as Dewar flask/thermos). Minimal heat enters by radiation only.
- Superheater/evaporator coil - a U-shaped or serpentine pipe on the way out of the tank that acts as a heat exchanger, warming the liquid oxygen to gas before it enters the hospital pipeline
- Safety blow-off (pressure relief) valve - set at 17 bar (1700 kPa); opens if internal pressure becomes dangerously high
- Pressure raising valve and vaporizer - used during high-demand periods (see working below)
- Weighing mechanism - the entire tank sits on a platform scale; weight is the only reliable way to determine remaining oxygen content (you cannot assess content by pressure alone since liquid-vapour equilibrium is maintained)
- Refill inlet - accepts liquid oxygen delivery from a tanker truck
Working Principle
Normal Operation (Low/Moderate Demand)
- Liquid oxygen is stored at approximately -150 to -180°C and 10 bar (1000 kPa)
- In normal conditions, gaseous oxygen from the vapour phase at the top of the tank is piped out
- This gas passes through a superheater coil (ambient-temperature heat exchanger) where it warms to safe temperature for pipeline delivery
- It then passes through a series of pressure reducing valves that step down the pressure:
- Tank pressure: ~10 bar
- Intermediate: reduced stepwise
- Pipeline pressure delivered to hospital: 4.1 bar (410 kPa / ~60 psi)
- Pressure reducing valves at the theatre wall reduce this further to 50 psi (3.4 bar) for the anaesthesia machine
During High Demand (e.g., Mass Casualty/High Surgical Throughput)
- High gas extraction causes rapid vaporization → latent heat of vaporization is absorbed from remaining liquid → liquid temperature and saturated vapour pressure (SVP) drop
- This reduces the pressure in the vapour phase
- The drop in vapour pressure activates the pressure raising valve, which:
- Pipes liquid oxygen from the bottom of the tank through a separate pressure raising vaporizer
- The warmed gas re-joins the main gas stream, boosting pressure back to normal supply pressure
- The pressure raising vaporizer pipe is typically encrusted with ice from the extreme cold of vaporizing liquid oxygen - this is a normal and expected finding
During Low Demand / Hot Weather
- Ambient heat gradually enters despite insulation → temperature and SVP rise
- If pressure rises above 17 bar → blow-off valve opens, releasing oxygen to atmosphere
- This evaporative loss cools the remaining liquid (gas law: pressure loss = temperature loss), restoring normal working pressure
- This continuous loss of oxygen when demand is low is an inherent inefficiency of VIE systems
Operating Parameters - Summary Table (Key Exam Numbers)
| Parameter | Value |
|---|---|
| Storage temperature | -150°C to -180°C |
| Storage pressure | ~10 bar (1000 kPa) |
| Safety blow-off valve pressure | 17 bar (1700 kPa) |
| Pipeline pressure to hospital | 4.1 bar (410 kPa) |
| Pressure at anaesthesia machine wall outlet | ~4 bar (400 kPa / ~50 psi) |
| Cylinder (E-cylinder) backup pressure at machine | 45 psi (3.1 bar) |
| Vacuum in insulating space | ~0.3 kPa |
| Oxygen critical temperature | -118°C |
| Oxygen boiling point | -183°C |
How to Measure Remaining Content
Pressure measurement cannot reliably indicate the remaining volume in a VIE because:
- As long as both liquid and vapour phases coexist, the vapour pressure remains constant (determined only by temperature, not amount of liquid)
- Pressure only falls once all liquid has evaporated (all oxygen is then in gas phase)
Therefore, the only reliable method is weighing the tank. The tank is mounted on a large platform scale or hinged mechanism, and content is inferred from weight.
Comparison: VIE vs Oxygen Cylinders
| Feature | VIE | Cylinder (E-type) |
|---|---|---|
| State of storage | Liquid | Gas (compressed) |
| Temperature | -150 to -180°C | Room temperature |
| Pressure | ~10 bar | ~137 bar (full E-cylinder: 1900 psi) |
| Capacity | Thousands of litres | 600 L (E-cylinder at 20°C) |
| Content estimation | Weight only | Pressure gauge (gas obeys Boyle's law) |
| Use | Primary hospital supply | Backup/portable/anaesthesia machine |
| Cost-effective when | >300 L/min consumption | Smaller facilities |
| Content assessment | Pressure unreliable; use weight | Pressure proportional to remaining gas |
Safety Features of the VIE System
- Pressure blow-off (relief) valve at 17 bar - prevents catastrophic rupture
- Vacuum insulation - prevents heat ingress; minimizes uncontrolled evaporation
- Superheater coil - ensures only warm gas enters pipeline (prevents ice formation in pipes)
- Pressure reducing valves (staged) - stepped pressure reduction to safe pipeline level
- Pressure raising valve + vaporizer - maintains supply during high demand
- Weight-based content measurement - accurate regardless of temperature
- Sited outdoors - spilled/vented liquid oxygen cannot accumulate in enclosed spaces (oxygen-enriched atmospheres are fire hazards)
- Backup cylinder manifold - automatic switchover if VIE fails
- Pipeline alarms - low-pressure alarms in theatre and anaesthesia machine
Hospital Pipeline Distribution - From VIE to Theatre
VIE (Outdoor, -150°C, 10 bar)
↓ Superheater/Evaporator coil
↓ Pressure reducing valves → 4.1 bar
↓ Hospital pipeline (copper tubing, colour-coded GREEN)
↓ Wall outlet (DISS/Quick-connect connector - gas specific)
↓ Anaesthesia machine DISS inlet → 50 psi (≈3.4 bar)
↓ Pipeline check valve (prevents retrograde flow)
↓ Pressure gauge (pipeline)
↓ Flow control → Rotameter → Vaporizer → Common Gas Outlet
-
Pipeline connectors are Diameter Index Safety System (DISS) - non-interchangeable between gases
-
Colour coding: Oxygen = Green (UK/Europe: White)
-
Pipeline gas always takes priority over cylinder supply (50 psi vs 45 psi cylinder output)
-
If pipeline crossover is suspected: (1) Turn on cylinder backup → (2) Disconnect pipeline supply (mandatory - machine preferentially uses higher-pressure pipeline even if wrong gas)
-
Miller's Anesthesia, 10e; Morgan & Mikhail's Clinical Anesthesiology, 7e; Barash Clinical Anesthesia, 9e
Production of Medical Oxygen
Oxygen for VIE supply is manufactured by fractional distillation of air:
- Atmospheric air is filtered and cooled far below the boiling points of its constituents until it liquefies
- The liquid air is slowly warmed
- Constituents evaporate sequentially as they reach their boiling points:
- Nitrogen boils off at -195.8°C
- Liquid oxygen remains behind at -183°C
- Further purification yields medical-grade oxygen (≥99.5% purity)
Alternative: Pressure Swing Adsorption (PSA) using zeolite molecular sieves (used in oxygen concentrators - smaller scale)
Anaesthesia Machine Interface (Exam-Relevant Details)
- Pipeline oxygen enters the machine at 50 psig (3.4 bar); this drives flow through flowmeters and powers pneumatic ventilators
- E-cylinders on the machine deliver at 45 psig - intentionally lower so pipeline gas is preferred
- Oxygen flush valve bypasses vaporizers and delivers high-flow 100% O₂ (35-75 L/min) directly to the breathing circuit from the intermediate-pressure circuit
- Second-stage regulator inside the machine reduces 50 psig pipeline supply to a stable intermediate pressure (~16-26 psig) for the flowmeter circuits
- Fail-safe device (oxygen pressure failure device/Bosun whistle): cuts off or reduces N₂O flow proportionally if oxygen pipeline pressure falls
VIE Failure - Anaesthetic Implications
Causes of VIE/pipeline failure:
- Tank rupture (as occurred in 2002 - 8,000 gallons of liquid oxygen released)
- Pipeline crossover (most catastrophic - misconnection of O₂ and N₂O pipelines; caused 23 deaths in Sudbury, Ontario)
- Valve malfunction, pressure regulator failure
Anaesthetic response to suspected pipeline failure:
- Switch to cylinder supply (turn on E-cylinders)
- Disconnect pipeline hose from the wall (otherwise machine preferentially uses wrong gas at higher pipeline pressure)
- Use oxygen analyser in breathing circuit - last line of defence
- Conserve oxygen: reduce fresh gas flow, use closed circuit
- Cancel or expedite surgery; notify hospital engineering
- Barash Clinical Anesthesia, 9e; Miller's Anesthesia, 10e
Key Exam Summary Points
| Point | Fact |
|---|---|
| VIE stores oxygen as | Liquid |
| Storage temperature | -150 to -180°C |
| Oxygen critical temperature | -118°C (must stay below this) |
| Storage pressure | ~10 bar |
| Safety blow-off valve | 17 bar |
| Pipeline pressure | 4.1 bar (410 kPa) |
| Anaesthesia machine inlet | ~50 psi (3.4 bar) |
| Content measured by | Weight only (not pressure) |
| Insulation mechanism | Vacuum between double walls |
| Primary gas supply route | Vapour from top of tank |
| High-demand supply route | Liquid from bottom via pressure raising vaporizer |
| Oxygen manufacture | Fractional distillation of air |
| Backup to VIE | Cylinder bank manifold |
Sources: Miller's Anesthesia 10e | Morgan & Mikhail's Clinical Anesthesiology 7e | Barash Clinical Anesthesia 9e | Anaesthetics.ukzn.ac.za Medical Gases Review | Deranged Physiology - Wall Oxygen Supply
Burn in md anesthesia
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive textbook material. Let me compile the complete exam-ready answer:
Burns in MD Anaesthesia
Classification of Burns
By Depth
| Degree | Old Terminology | Structures Involved | Appearance | Pain | Healing |
|---|---|---|---|---|---|
| Superficial | 1st degree | Epidermis only | Erythema, dry, no blisters | Painful | 3-5 days, no scar |
| Superficial partial thickness | 2nd degree (superficial) | Epidermis + superficial dermis | Blisters, moist, pink/red | Very painful | 14 days, minimal scar |
| Deep partial thickness | 2nd degree (deep) | Epidermis + deep dermis | Pale/mottled, less moist | Less painful (nerve damage) | >21 days, scarring |
| Full thickness | 3rd degree | All skin layers | Leathery, white/brown/black, no blisters | Painless (nerve destroyed) | No self-healing; needs grafting |
| 4th degree | - | Muscle, bone, tendon | Charred | Painless | Amputation often needed |
By Extent - Rule of Nines (Wallace's Rule of Nines)
| Body Region | Adult % TBSA | Child (9 yrs) | Infant |
|---|---|---|---|
| Head and neck | 9% | 14% | 18% |
| Each upper limb | 9% | 9% | 9% |
| Chest (anterior trunk) | 18% | 18% | 18% |
| Posterior trunk | 18% | 18% | 18% |
| Each lower limb | 18% | 14% | 14% |
| Perineum | 1% | 1% | 1% |
Lund and Browder chart - more accurate than Rule of Nines, especially in children (accounts for age-related variation in head:leg ratio).
Palm method: Patient's palm (including fingers) = approximately 1% TBSA - useful for irregular burns.
Major Burn (Criteria for Burn Unit Admission)
-
25% TBSA in adults (>20% in elderly or children)
- Full thickness burns >10% TBSA
- Burns involving face, hands, feet, genitalia, perineum, major joints
- Inhalation injury
- Electrical or chemical burns
- Burns with associated trauma or significant pre-existing disease
Pathophysiology of Burn Injury
Local Response - Jackson's Zones (3 Concentric Zones)
┌──────────────────────────────────┐
│ Zone of HYPERAEMIA (outermost) │ ← Vasodilation; recovers fully
│ ┌────────────────────────────┐ │
│ │ Zone of STASIS (middle) │ │ ← Ischaemia; can be saved with
│ │ ┌──────────────────────┐ │ │ optimal resuscitation
│ │ │ Zone of COAGULATION │ │ │ ← Central core; irreversible
│ │ │ (innermost) │ │ │ necrosis
│ │ └──────────────────────┘ │ │
│ └────────────────────────────┘ │
└──────────────────────────────────┘
The zone of stasis is critical - inadequate resuscitation converts it to a zone of coagulation, deepening the burn.
Systemic Response
Phase 1: Ebb phase (0-48 hours) - Burn shock
- Massive capillary leak → fluid, protein, electrolytes lost into interstitium
- Most severe in first 8 hours; continues up to 24-48 hours
- Hypovolaemia → reduced cardiac output → organ hypoperfusion
- Catecholamine surge → peripheral vasoconstriction
Phase 2: Flow phase (>48 hours) - Hypermetabolic state
- Cardiac output rises to supernormal levels (2-3 x normal)
- Hypermetabolism: elevated BMR up to 200% of normal in severe burns
- Persistent catabolism, weight loss, muscle wasting
- Elevated body temperature set-point (~38.5°C)
- This phase can persist for up to 2 years post-injury
Fluid Resuscitation
Parkland (Baxter) Formula - Most Widely Used
4 mL × body weight (kg) × % TBSA burned Using Lactated Ringer's (Hartmann's) solution
Administration:
- First half given in the first 8 hours (from time of burn, NOT from time of arrival)
- Second half given over the next 16 hours
- Only superficial partial thickness, deep partial thickness, and full thickness burns are included in TBSA calculation. Superficial (1st degree/erythema) are excluded.
Other Formulae
| Formula | Crystalloid | Colloid | Notes |
|---|---|---|---|
| Parkland | 4 mL/kg/% TBSA LR (first 24h) | Albumin after 24h | Most widely used |
| Brooke | 2 mL/kg/% TBSA LR | 0.5 mL/kg/% plasma | |
| Galveston (paediatric) | 5000 mL/m² burned + 1500 mL/m² total BSA | - | Accounts for higher BSA:weight ratio |
Resuscitation endpoint: Urine output 0.5-1 mL/kg/hour in adults; 1 mL/kg/h in children. Invasive haemodynamic monitoring (CVP, arterial line) for major burns.
Fluid creep: A recognised problem with Parkland formula - trend toward over-resuscitation in practice (patients receiving 5-6 mL/kg/% rather than 4 mL/kg/%). This causes abdominal compartment syndrome, pulmonary oedema, and conversion of zone of stasis to necrosis.
Second 24 hours: Capillary integrity partially restored. Colloid (albumin) can now be used. Rate of Hartmann's reduced to maintain urine output. - Sabiston Textbook of Surgery; Miller's Anesthesia 10e
Inhalation Injury
Most important cause of early mortality in burns. Inhalation injury triples mortality compared to burn alone of same TBSA.
Three Components
1. Heat Injury to Upper Airway
- Supraglottic structures primarily affected (larynx, pharynx, oral cavity)
- Steam/hot air → mucosal oedema, erythema, ulceration
- Rapid, progressive swelling → airway obstruction can occur within hours
- Infraglottic thermal injury is rare (heat dissipated in upper airway)
Signs of impending upper airway obstruction:
- Hoarseness, stridor, voice change
- Singed nasal hairs, eyebrows
- Carbonaceous sputum
- Intra-oral soot
- Oropharyngeal burns, erythema, blistering
- Burns to face, neck, anterior chest
Management: Early intubation is paramount - do not wait for complete obstruction. Oedema will worsen over 12-24 hours. A tube that passes easily now may be impossible later.
2. Toxic Gas Inhalation
Carbon Monoxide (CO) Poisoning:
| COHb Level | Symptoms |
|---|---|
| 10-20% | Headache, nausea |
| 20-40% | Confusion, lethargy, syncope |
| 40-60% | Coma, convulsions |
| >60% | Death |
- CO binds haemoglobin with 250 times the affinity of oxygen → shifts oxygen dissociation curve left (Haldane effect) → tissue hypoxia
- SpO₂ by pulse oximetry is falsely normal (cannot distinguish COHb from OxyHb)
- Treatment: 100% O₂ - reduces CO half-life from 4-5 hours (room air) to 60-90 minutes (100% O₂) to 20-25 minutes (hyperbaric O₂ at 3 atm)
- Hyperbaric O₂ indicated for: COHb >25%, unconsciousness, neurological symptoms, pregnancy, cardiac involvement - Morgan & Mikhail's Clinical Anesthesiology, 7e
Cyanide (HCN) Poisoning:
- Formed from combustion of nitrogen-containing polymers (wool, silk, polyurethane, vinyl)
- Binds cytochrome oxidase → uncouples mitochondrial oxidative phosphorylation → profound cellular hypoxia despite adequate O₂ delivery
- Suspect if: unexplained metabolic acidosis with elevated lactate despite adequate oxygenation
- Treatment: Hydroxocobalamin (Cyanokit) - binds cyanide to form cyanocobalamin; 100% O₂; sodium thiosulphate
3. Chemical Burn - Lower Airway
- Carbonaceous particles carry toxic aldehydes, acids deep into bronchi
- Mucosal injury → oedema, ciliary dysfunction, mucus plugging
- Manifestations of acute lung injury (ALI) and ARDS typically appear 2-3 days after injury
- Loss of ciliary activity impairs clearance → bacterial colonization → pneumonia - Morgan & Mikhail's Clinical Anesthesiology, 7e
Anaesthetic Management
Preoperative Assessment - Key Focus Points (Box 83.3, Miller's)
- Time and extent of burn - when did the injury occur? Which phase (ebb or flow)?
- Airway evaluation - contractures, limited mouth opening, oedema, previous difficult intubation, tracheostomy
- Inhalation injury - CO poisoning, airway oedema, bronchospasm, ARDS
- Fluid received - cumulative fluid balance, adequacy of resuscitation, signs of over-resuscitation
- Vascular access - where are viable IV access sites (may need to insert through burned tissue)?
- NPO status and enteral feeding - when last fed? post-pyloric feeding tubes?
- Current medications - opioid tolerance (chronic), antibiotics, vasopressors
- Laboratory results - haemoglobin, electrolytes (K⁺), coagulation, albumin, ABG
Airway Management in Burns
Acute phase concerns:
- Progressive oedema (worst at 8-24 hours) → plan early intubation
- Facial burns → mask seal difficult; exudate contaminates mask
- Neck burns/contractures → limited neck mobility, restricted mouth opening
- Airway distortion from direct burn or oedema
Chronic phase concerns:
- Scar contractures of face, neck, mouth (microstomia)
- Restricted neck extension
- Receding chin from scar tissue
Approach:
- Awake fibreoptic intubation (FOI) - gold standard when difficult airway anticipated
- Pre-oxygenate thoroughly
- Nebulised or spray-as-you-go topical lidocaine for awake FOI
- If uncooperative/paediatric: ketamine sedation (maintains airway tone) + FOI
- Video laryngoscopy as alternative - also permits assessment of hypopharyngeal anatomy
- Tracheostomy under local anaesthesia if airway access is extreme
- Surgeon capable of surgical tracheostomy must be present and scrubbed when airway difficulty is anticipated - Miller's Anesthesia, 10e
Securing the ETT:
- Adhesive tape useless on burned or moist skin
- Options: circumferential tie around head, wire fixation to teeth, arch bars, umbilical tape harness
Tracheostomy:
- Consider early if prolonged mechanical ventilation anticipated
- Indications: large burn, inhalation injury, advanced age, chronic pulmonary disease, facial burns needing repeated OR access
Pharmacology - Altered Drug Responses in Burns (Critical Exam Topic)
Succinylcholine - CONTRAINDICATED after 48 hours
Mechanism: Burn injury causes upregulation and proliferation of acetylcholine receptors (both junctional and extrajunctional/foetal-type). These immature receptors are hypersensitive to succinylcholine and remain open longer → massive K⁺ efflux → potentially lethal hyperkalemia (K⁺ can rise by 5-13 mEq/L).
Timeline:
- Safe within first 24-48 hours of injury
- Contraindicated from 48 hours until full wound healing (may persist for months/years)
- Even small doses (0.1 mg/kg) may cause hyperkalemia - inadequately studied - Miller's Anesthesia, 10e
Key exam fact: Succinylcholine is also contraindicated in: spinal cord injury, prolonged immobilisation, stroke, crush injury, severe sepsis, Guillain-Barré, muscular dystrophy.
Non-Depolarising Muscle Relaxants (NDMRs) - Increased Requirements
- The same upregulation of ACh receptors that makes succinylcholine dangerous also makes NDMRs less effective (more receptors to block)
- Patients require higher doses (often 2-5x normal) and may have shorter duration of action
- Monitor with neuromuscular monitor (train-of-four) - never rely on standard dosing
- Response unpredictable; titrate carefully
Opioids - Increased Requirements
- Hypermetabolism → accelerated drug metabolism
- Opioid tolerance develops rapidly (especially with repeated procedures)
- Increased Vd from fluid resuscitation/protein changes → lower peak concentrations
- May require very high opioid doses; patient-controlled analgesia (PCA) useful
- Methadone useful for opioid rotation in chronic cases
Propofol and Barbiturates
- Increased Vd early (fluid resuscitation, oedema) → larger induction doses needed
- Late phase: normal or decreased requirements due to protein binding changes (decreased albumin)
Volatile Agents
- Generally safe; no specific contraindication
- Maintain normothermia - patients are highly vulnerable to hypothermia (loss of skin, large exposed wound surface)
Local Anaesthetics
- Altered pharmacokinetics: changes in hepatic function, protein binding, Vd
- Caution with neuro/cardiotoxic risk in critically ill patients
- Liposomal bupivacaine offers longer duration with potentially better safety profile - Miller's Anesthesia, 10e
Intraoperative Management
Monitoring
- Standard ASA monitors + arterial line (A-line) for beat-to-beat BP and frequent ABG
- Central venous access (may need to place through burned tissue - tunnelled if possible)
- Temperature monitoring - essential (hypothermia is a major risk)
- Urine output (catheter) - target 0.5-1 mL/kg/h
Temperature Management
- Burns destroy the skin barrier → massive heat and insensible fluid losses
- Operating theatre temperature raised to >28-30°C (feels uncomfortable for staff)
- Warm IV fluids, warm irrigation, forced-air warming, radiation lamps
- Hypothermia worsens coagulopathy (the "lethal triad" also applies in burns surgery)
Blood Loss
- Excision of burned tissue is highly vascular → massive blood loss expected
- Full-thickness burn excision: approximately 0.75-1 mL blood loss per cm² excised
- For large excisions: have cross-matched blood immediately available; cell salvage may be used
- Epinephrine-soaked (1:200,000) dressings applied to donor sites reduce blood loss
- Tumescent technique (subcutaneous injection of dilute epinephrine/LA) reduces donor site bleeding
- Tourniquets used for limb excisions
Positioning
- Large wounds may require frequent repositioning → pressure area care, padding, secure monitoring
- Prone positioning may be required (back burns)
Ventilation
- In patients with inhalation injury: lung-protective ventilation (TV 6 mL/kg IBW, PEEP 5-10, plateau pressure <30 cmH₂O)
- High-frequency oscillatory ventilation (HFOV) for severe ARDS
- Nebulised N-acetylcysteine and heparin alternating 4-hourly: mucolytic + anticoagulant; reduces cast formation and plugging in lower airway
Pain Management in Burns - Multimodal Analgesia
Burns produce the most severe and prolonged pain of any injury. Pain has two components:
- Background pain - continuous; treated with regular opioids ± adjuncts
- Procedural pain - dressing changes, physiotherapy, surgery - treated with additional analgesia
Opioids: Morphine, fentanyl, oxycodone - mainstay. PCA for background pain. High tolerance develops.
Ketamine: Most useful agent in burn anaesthesia.
- NMDA antagonist → dissociative anaesthesia + analgesia + amnesia
- Maintains airway tone and spontaneous ventilation
- Ideal for dressing changes, debridements, minor procedures
- Prevents central sensitisation and opioid-induced hyperalgesia
- IV ketamine: rapid onset; can be run as infusion on ward
- Anti-depressant effect via norketamine metabolite (useful in burns)
- Side effects: emergence delirium (give midazolam concurrently), hallucinations, nausea - Miller's Anesthesia, 10e
Dexmedetomidine: Alpha-2 agonist; sedation + analgesia without respiratory depression; reduces opioid requirements; reduces delirium in ICU (compared to benzodiazepines). Avoid in haemodynamic instability.
Gabapentin/Pregabalin: Useful for neuropathic pain; reduces central sensitisation; adjunct to opioids.
Benzodiazepines: Treat anticipatory anxiety pre-dressing changes; midazolam + opioid combination well-studied.
NSAIDs: Generally avoided - bleeding risk, renal complications (already at risk from hypovolaemia and myoglobinuria), GI effects.
Regional Anaesthesia:
- Peripheral nerve blocks (lateral femoral cutaneous nerve, fascia iliaca block) - ideal for thigh donor sites
- TAP blocks and paravertebral blocks for trunk donor sites; catheters for prolonged analgesia
- Central neuraxial (spinal/epidural) - possible but concerns about infection risk in heavily colonised patients
- Tumescent local anaesthesia for donor sites pre-harvest - Miller's Anesthesia, 10e
Electrical Burns
Severity depends on: Voltage, current type (AC more dangerous than DC), path of current, duration, tissue resistance.
AC vs DC:
- AC (household) at 50 Hz → tetanic muscle contraction → cannot release hold → prolonged contact
- DC (lightning) → single strong contraction → usually thrown away from contact → shorter exposure
High vs Low voltage:
- Low voltage (<1000V): damage at contact site
- High voltage (>1000V): deep tissue damage, especially muscle around bone (bone has highest resistance → most heat)
Specific concerns:
- Rhabdomyolysis → myoglobinuria → acute kidney injury (AKI)
- If myoglobinuria present: urine output 1-2 mL/kg/h until urine clears
- NaHCO₃ to alkalinise urine, mannitol ± furosemide to facilitate excretion
- Cardiac arrhythmias - sinus tachycardia most common; VF and cardiac standstill in severe cases
- Compartment syndrome - limbs may need fasciotomy within 24 hours
- Spinal cord injury from tetanic contraction (vertebral fractures)
- Cutaneous burn often underestimates the true extent of deep injury - formula-based fluid resuscitation is inadequate; must titrate to urine output and clinical response
- Entry and exit wounds always present - look for them - Miller's Anesthesia, 10e
Chemical Burns
- Acid burns: Coagulation necrosis - self-limiting protein layer prevents deeper penetration
- Alkali burns: Liquefaction necrosis - no limit to penetration, continue to deepen → often deeper than acid burns of same contact time
- Immediate treatment: Copious water irrigation for at least 20-30 minutes (do not neutralise - neutralisation reactions generate heat)
- Hydrofluoric acid (HF): unique - fluoride ions penetrate deeply; chelates Ca²⁺ and Mg²⁺; causes hypocalcaemia, hypomagnesaemia, life-threatening arrhythmias; treat with IV/topical calcium gluconate
Perioperative Complications and the "Burn Triad"
Analogous to trauma's lethal triad:
Hypothermia
/\
/ \
/ \
Coagulopathy --- Metabolic Acidosis
Each worsens the others. Anaesthetic strategy must break this cycle:
- Aggressive warming throughout
- Damage control approach for massive haemorrhage (1:1:1 blood products)
- Correct acidosis (adequate resuscitation, not sodium bicarbonate)
Infection and Sepsis
- Leading cause of late morbidity and mortality
- Loss of skin barrier + immunosuppression + invasive devices = major infection risk
- Most common sources: pneumonia, central line infection, burn wound infection
- Do NOT give prophylactic systemic antibiotics - promotes resistance
- Topical antimicrobials for wound: silver sulfadiazine, silver nitrate, mafenide acetate
- SIRS criteria unreliable in burns (>90% meet criteria regardless of infection status)
- Antibiotics should be culture-directed; dose-adjust for altered pharmacokinetics
- Miller's Anesthesia, 10e
Summary: Key Exam Points
| Topic | Key Fact |
|---|---|
| Succinylcholine | Contraindicated >48 hours post-burn; lethal hyperkalemia via upregulated ACh receptors |
| NDMRs | Increased dose required (2-5x); upregulated receptors; monitor TOF |
| Parkland formula | 4 mL/kg/% TBSA LR; half in first 8h, half in next 16h |
| Inhalation injury | Triples mortality; early intubation; 100% O₂ for CO poisoning |
| CO poisoning | COHb 250x affinity; SpO₂ falsely normal; treat with 100% O₂ |
| Airway strategy | Awake FOI / video laryngoscopy / ketamine + FOI in children |
| Ketamine | Agent of choice for procedures; NMDA antagonist; maintains airway |
| Hypermetabolism | Begins >48h; elevated CO, BMR up to 200%; persists years |
| Electrical burns | Rhabdomyolysis; underestimate depth; fasciotomy; ECG monitoring |
| Temperature | Raise OT to >28°C; warm all fluids; hypothermia is major risk |
| Jackson zones | Coagulation (centre), Stasis (rescuable), Hyperaemia (outer) |
| Critical burn (ICU) | >25% TBSA adult; >20% elderly/child; full thickness >10%; inhalation |
Sources: Miller's Anesthesia 10e (Chapter 83 - Burns) | Morgan & Mikhail's Clinical Anesthesiology 7e | Sabiston Textbook of Surgery | Tintinalli's Emergency Medicine | Schwartz's Principles of Surgery 11e
This is a shared conversation. Sign in to Orris to start your own chat.