Teach me supraventricular tachycardia starting from basics till treatment complete orders in detail like you are my professor who wants me to be a good topper and proper descendant to u
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Alright, student - sit down, open your notebook, and pay close attention. We are going to go through SVT the way a topper should understand it: from first principles, to mechanisms, to ECG, to every drug and dose. By the end, you should be able to manage any SVT case that walks through your door.
SUPRAVENTRICULAR TACHYCARDIA (SVT) - A Complete Professor's Lecture
CHAPTER 1: THE BASICS - WHERE DOES THE HEART BEAT COME FROM?
Before you understand SVT, you must understand normal cardiac conduction.
Normal Conduction Pathway (Memorize This Sequence)
SA Node → Atrial Myocardium → AV Node (DELAY!)
→ Bundle of His → Right & Left Bundle Branches
→ Purkinje Fibers → Ventricular Myocardium
The AV node is your gatekeeper. It introduces a deliberate delay (PR interval, normally 120-200 ms) to allow the atria to empty into the ventricles BEFORE the ventricles contract. This is brilliant engineering.
Key point: Anything that originates above (supra) the bundle of His is called supraventricular. This includes the SA node, atrial tissue, and the AV node itself.
CHAPTER 2: WHAT IS SVT?
Definition: SVT is a broad umbrella term for any tachyarrhythmia (rate > 100 bpm) that originates above the bundle of His - i.e., in the atria or AV node.
In clinical practice, when doctors say "SVT" without qualification, they usually mean Paroxysmal SVT (PSVT) - which refers specifically to AVNRT or AVRT (explained below). Sinus tachycardia, atrial fibrillation, and atrial flutter are technically SVTs but are discussed separately.
The SVT Family - Classification
| Category | Specific Arrhythmias |
|---|---|
| AV Node-Dependent (require AV node in circuit) | AVNRT, AVRT (orthodromic) |
| AV Node-Independent (AV node is bystander) | Sinus tachycardia, Atrial tachycardia (AT), Atrial flutter, Atrial fibrillation |
| Preexcited | Antidromic AVRT (WPW), Atriofascicular tachycardia |
Teaching Point: Why does this matter? Because drugs that block the AV node (adenosine, beta-blockers, verapamil) will terminate AV node-dependent SVTs, but in AV node-independent SVTs they only transiently slow the rate (exposing the underlying P waves, giving you a diagnostic clue!).
CHAPTER 3: ELECTROPHYSIOLOGY ESSENTIALS
The Three Mechanisms of Arrhythmias
To understand SVT deeply, you must know WHY abnormal rhythms occur:
1. Reentry (Most common - responsible for 90%+ of SVTs)
- Requires: (a) Two separate conduction pathways, (b) Unidirectional block in one, (c) Slow conduction in the other
- The impulse goes down one path, finds the other pathway has recovered, comes back up - and loops endlessly
- Think of it like a rotating door that never stops spinning
2. Enhanced Automaticity
- Cells fire spontaneously at a faster-than-normal rate (like the SA node speeding up, or an ectopic focus taking over)
- Example: Atrial tachycardia from an ectopic focus
3. Triggered Activity
- Early or delayed afterdepolarizations - abnormal voltage spikes off the back of a normal action potential
- Associated with digoxin toxicity, hypokalemia
CHAPTER 4: THE THREE MAJOR SVTs IN CLINICAL PRACTICE
SVT-1: AVNRT (AV Nodal Reentrant Tachycardia)
The most common SVT you will encounter. Represents ~60% of all PSVT cases referred for ablation.
The Anatomy You Must Know
The AV node has two functional inputs - this is the key to AVNRT:
| Pathway | Speed | Refractory Period |
|---|---|---|
| Fast pathway | Fast conduction | Long refractory period |
| Slow pathway | Slow conduction | Short refractory period |
Both pathways converge at the compact AV node. The slow pathway runs along the tricuspid annulus toward the coronary sinus ostium, within the Triangle of Koch (bounded by: tricuspid annulus anteriorly, tendon of Todaro posteriorly, CS ostium inferiorly, His bundle at the apex).
Mechanism of Typical AVNRT (Slow-Fast): Step by Step
- A premature atrial beat (PAC) arrives when the fast pathway is still refractory (just finished conducting)
- The PAC can only go down the slow pathway (short refractory = already recovered)
- By the time it reaches the bottom and turns around, the fast pathway has recovered
- The impulse shoots back up the fast pathway rapidly
- This activates the atria and ventricles nearly simultaneously
- The circuit keeps spinning: down slow, up fast, down slow, up fast...
Epidemiology: Most common in women (2:1 female-to-male ratio), typically manifests in the 2nd-4th decade. NOT associated with structural heart disease.
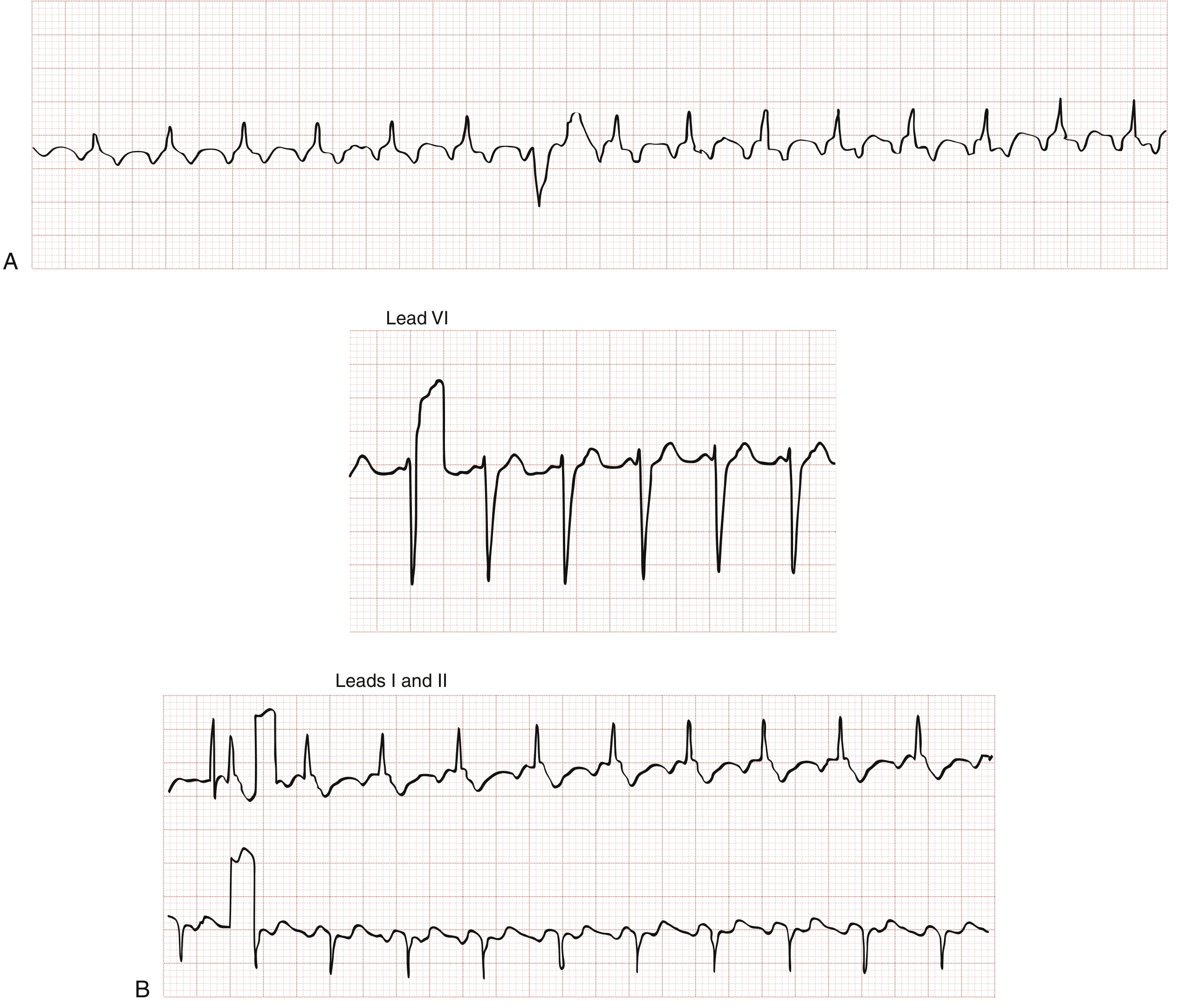
ECG of Typical AVNRT
- Rate: 150-250 bpm (average ~170 bpm)
- QRS: Narrow (< 100 ms) - because ventricular conduction is normal
- P waves: "Buried" in the QRS in ~70% (atria and ventricles activate simultaneously)
- In 30%: a retrograde P wave appears as a pseudo-r' in V1 and pseudo-S wave in leads II, III, aVF - look for this! Compare with the patient's baseline ECG
- Short RP tachycardia (RP < PR)
- Cannon A waves in JVP - because atria contract against closed tricuspid valve
- Post-tachycardia polyuria - due to ANP release from stretched atria
Here is the ECG showing AVNRT with P waves buried in the QRS (transition from sinus to tachycardia visible):
Atypical AVNRT (Fast-Slow or Slow-Slow)
- Less common
- Conduction goes DOWN the fast pathway, UP the slow pathway
- P wave falls LATE in the R-R interval - this is a long RP tachycardia
- Differential: focal AT, PJRT (permanent junctional reciprocating tachycardia)
SVT-2: AVRT (AV Reentrant Tachycardia) and WPW Syndrome
The second most common SVT. Most common in the first decade of life. Requires an accessory pathway (AP) - an anomalous extra muscle bundle connecting atria to ventricles, bypassing the AV node.
What is an Accessory Pathway?
A thin strand of subendocardial tissue with conductive properties - essentially a "short-circuit wire" around the AV node. Unlike the AV node, it does NOT delay conduction.
Types:
- Manifest AP: Conducts both anterograde and retrograde - visible as delta wave on resting ECG
- Concealed AP: Conducts retrograde only - no delta wave during sinus rhythm, but can cause SVT
WPW Syndrome = manifest AP + episodes of PSVT. ECG in sinus rhythm shows: short PR interval + delta wave (slurred upstroke of QRS) + wide QRS
Mechanism of AVRT
Here is a visual showing all three situations - sinus rhythm with AP, orthodromic AVRT, and antidromic AVRT:
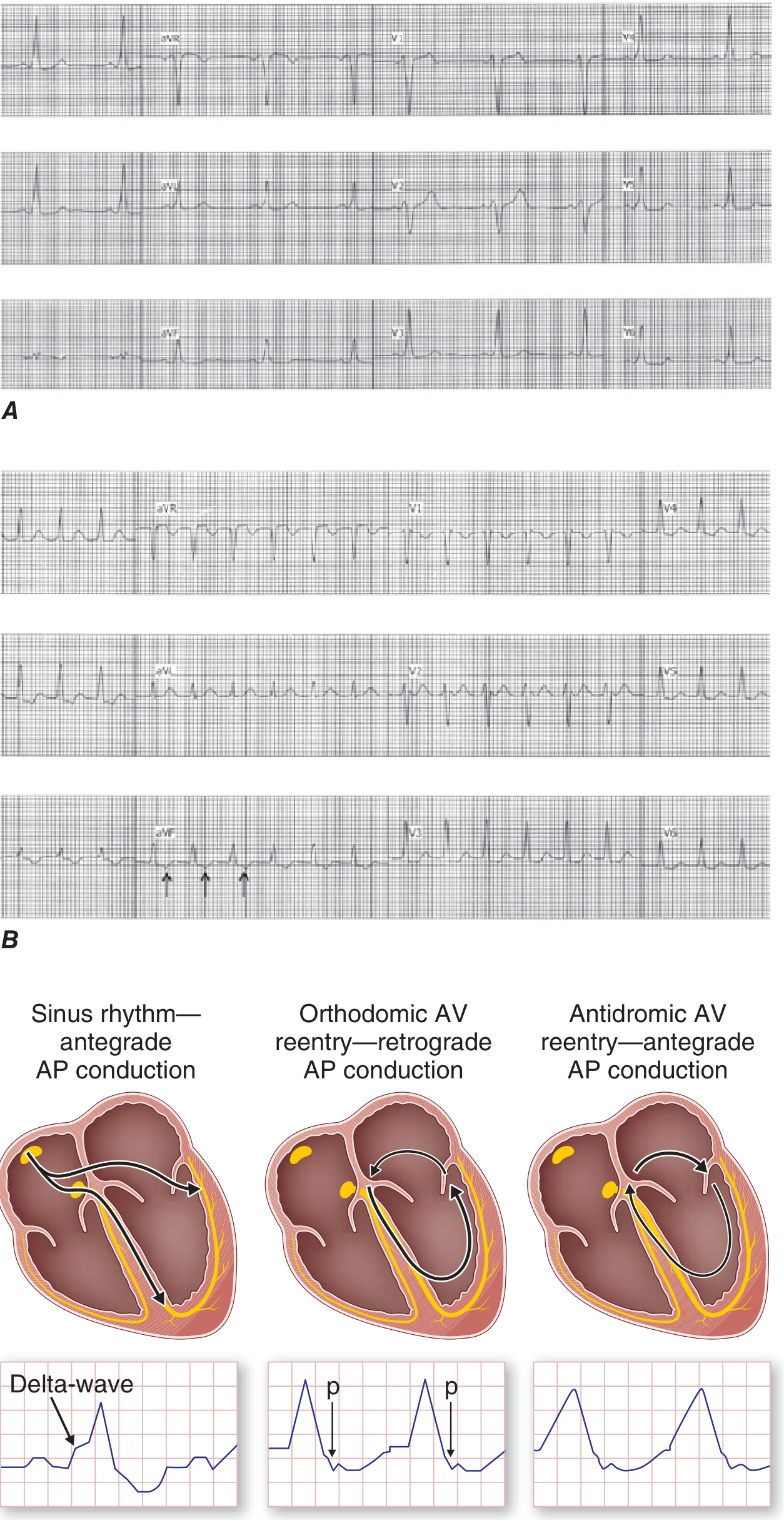
Orthodromic AVRT (95% of AVRT):
- Antegrade: Down the AV node (normal)
- Retrograde: Back UP the accessory pathway
- Result: Narrow QRS (normal ventricular conduction via His-Purkinje)
- P waves visible AFTER QRS, separated by >70 ms (RP interval is short but distinguishable from QRS)
- This is a short RP tachycardia
Antidromic AVRT (< 5% of AVRT):
- Antegrade: DOWN the accessory pathway (bypasses AV node)
- Retrograde: Back up the AV node
- Result: Wide QRS (fully preexcited ventricle, no normal His-Purkinje activation)
- Can look identical to VT - dangerous trap!
- NEVER use AV nodal blockers (adenosine, verapamil, beta-blockers) if you suspect antidromic AVRT with AF/flutter - removing AV nodal block lets AF conduct rapidly via the AP, potentially causing VF
DANGER ZONE: In WPW + AF - the AP can conduct extremely fast (300+ bpm to ventricles), causing hemodynamic collapse and VF. Treat with IV procainamide or cardioversion. Adenosine is relatively contraindicated.
SVT-3: Atrial Tachycardia (AT)
- Focal origin in atrial tissue (often pulmonary vein ostia, crista terminalis, coronary sinus)
- Mechanism: enhanced automaticity or triggered activity (not reentry through AV node)
- Rate: 130-250 bpm
- P waves: VISIBLE before QRS, morphology different from sinus P
- AV node is a bystander - vagal maneuvers/adenosine slow the rate transiently but DO NOT terminate (this is your key diagnostic clue - it exposes the underlying P waves and confirms AT)
- Long RP tachycardia (RP > PR)
CHAPTER 5: ECG INTERPRETATION - THE SYSTEMATIC APPROACH
When you see a narrow-complex tachycardia on an ECG, ask these questions in sequence:
Step 1: Is the QRS narrow (< 100 ms) or wide (> 100 ms)?
- Narrow = supraventricular in origin (ventricular conduction is normal)
- Wide = VT until proven otherwise; can also be SVT with aberrancy or preexcited tachycardia
Step 2: Is the rhythm regular or irregular?
- Regular narrow-complex: AVNRT, AVRT, AT, atrial flutter with fixed block, sinus tachycardia
- Irregular narrow-complex: AF, multifocal AT, atrial flutter with variable block
Step 3: Where are the P waves and what do they look like?
| P wave Location | Likely Diagnosis |
|---|---|
| Buried in QRS / pseudo-r' in V1 | Typical AVNRT |
| Just after QRS, RP < 70 ms | AVNRT |
| After QRS, RP 70-100 ms | Orthodromic AVRT |
| Before QRS, different morphology from sinus | Atrial tachycardia |
| P after QRS, RP > 50% of RR interval | Atypical AVNRT, PJRT, AT |
| No P waves, fibrillatory baseline | AF |
| Sawtooth pattern at 300 bpm | Atrial flutter |
ECG Features of PSVT (AVNRT/AVRT) - Summary Table
| Feature | Finding |
|---|---|
| Rate | 130-300 bpm (usually 170-180 bpm) |
| Rhythm | Regular |
| QRS | Narrow (< 100 ms), unless aberrancy |
| P waves | Absent/buried (70%) or retrograde (30%) |
| Onset/offset | Abrupt ("paroxysmal") |
| Effect of vagal maneuvers | Terminates (AVNRT, AVRT) or transiently slows (AT, flutter) |
CHAPTER 6: CLINICAL PRESENTATION
Typical symptoms:
- Palpitations - rapid, regular "fluttering" - sudden onset and sudden termination (paroxysmal)
- Light-headedness (most common at onset)
- Dyspnea, chest discomfort (high rates, especially elderly)
- Syncope - rare; if present, think WPW + AF or structural disease
- Post-event fatigue for up to 24 hours
- Polyuria post-episode (ANP release)
- Neck pounding / visible jugular pulsations - from cannon A waves (AVNRT)
Common triggers:
- Sudden movements, exercise, emotional stress
- Caffeine, alcohol, stimulants
- Premature atrial or ventricular beats initiating the reentrant circuit
Who gets it?
- AVNRT: young to middle-aged women, no structural heart disease
- AVRT: youngest group (infants, children, young adults), congenital accessory pathway
- AT: older adults, structural heart disease, lung disease
Important: Female patients with PSVT are frequently misdiagnosed with anxiety or panic attacks. Keep SVT in your differential for any woman with episodic palpitations.
CHAPTER 7: DIAGNOSIS AND WORKUP
Investigations:
- 12-lead ECG - during tachycardia AND in sinus rhythm (compare QRS morphology, look for delta waves, bundle branch blocks)
- Continuous ECG monitoring - during all acute management
- Vagal maneuver response (diagnostic AND therapeutic)
- Holter monitor / event recorder - for paroxysmal events not caught on routine ECG
- Electrophysiologic study (EPS) - gold standard for mechanism; done before catheter ablation
- Echo - to exclude structural heart disease
- Troponin - mild elevation can occur from rapid rate; must rule out ACS in appropriate patients
CHAPTER 8: TREATMENT - THE COMPLETE ORDERS
This is what separates a topper from an average student. Memorize the algorithm, know the doses, know the contraindications.
ACUTE MANAGEMENT ALGORITHM
Here is the official treatment algorithm from Harrison's 22nd edition - study this carefully:
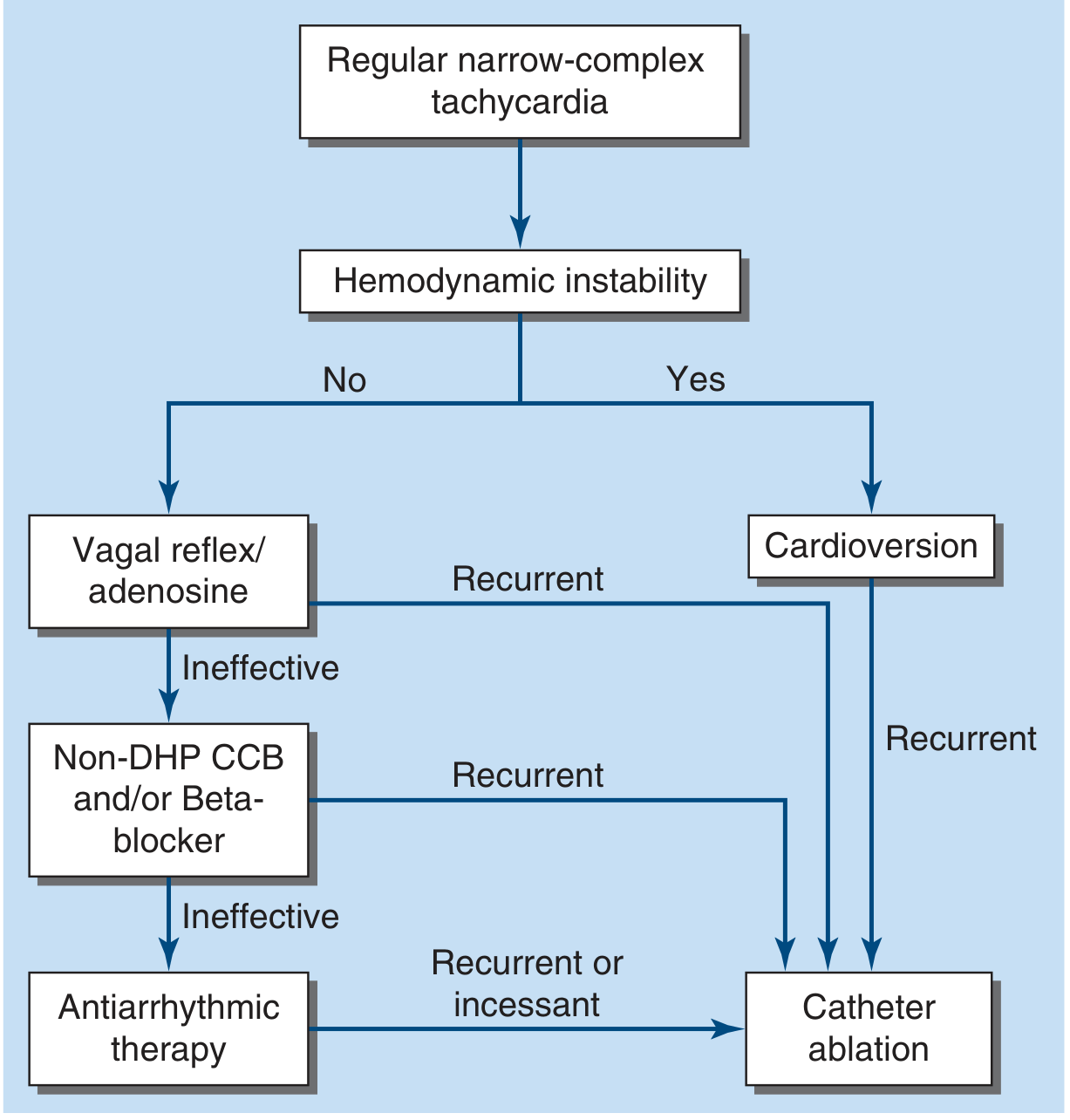
STEP 1: Assess Hemodynamic Stability FIRST
Unstable (hypotension, altered consciousness, pulmonary edema, severe chest pain)?
- → IMMEDIATE SYNCHRONIZED DC CARDIOVERSION
- Start at 100-200 J (biphasic preferred)
- Sedate with IV midazolam or propofol if conscious
- No time for drugs
Stable? → Proceed step-by-step below
STEP 2: Vagal Maneuvers (First-Line for Stable SVT)
Why they work: Increase vagal tone → slow AV node conduction → interrupt the reentry circuit
Valsalva Maneuver (most effective):
- Ask the patient to strain as if having a difficult bowel movement for 15-20 seconds
- Do this in SUPINE position
- Then immediately have the patient lie flat with legs raised (modified Valsalva / "REVERT technique") - this increases venous return and reflex vagal tone
- Success rate: up to 40-50% when done properly
- Patient can be taught to self-perform at home for future episodes
Carotid Sinus Massage:
- Firm circular pressure on the carotid sinus (at the angle of the jaw, where the common carotid bifurcates) for 5-10 seconds
- Check for carotid bruits FIRST - contraindicated if present
- Contraindicated in: prior stroke, carotid stenosis, prior carotid endarterectomy
- Do NOT massage both sides simultaneously (risk of cerebral ischemia)
Other vagal maneuvers: Diving reflex (ice water to face), gagging, coughing
STEP 3: Adenosine (Drug of Choice for Stable SVT)
Mechanism: Adenosine activates A1 receptors on the AV node → hyperpolarizes nodal cells → transient AV block → breaks the reentry circuit. Half-life = 10 seconds (ultra-short).
Dose (Rosen's / Harrison's):
- First dose: 6 mg IV rapid bolus - given as fast as possible through a large-bore IV (antecubital or central, NOT hand vein)
- Immediately followed by 20 mL normal saline rapid flush
- If no response within 1-2 minutes: second dose: 12 mg IV rapid bolus + flush
- If still no response: third dose: 12 mg IV (some centers give a second 12 mg)
- Success rate: 85-90% of AV node-dependent SVTs
Why rapid injection + proximal IV? Adenosine is cleared extremely fast in the bloodstream. It must reach the heart before it is inactivated. Peripheral hand veins with slow injection = drug never reaches AV node.
Important side effects to warn the patient about (they WILL occur and are terrifying):
- Transient chest tightness/pressure
- Sense of impending doom / anxiety
- Flushing, dyspnea
- All last < 30 seconds due to ultra-short half-life
Monitoring after adenosine:
- Run a continuous ECG rhythm strip
- You may see: (a) Termination of SVT and return to sinus - success; (b) Slowing with continued P waves visible - suggests AT or flutter (diagnostic); (c) Brief AF after adenosine (15% of patients) - usually self-terminates
Contraindications:
- Prior cardiac transplantation (hypersensitivity due to surgical denervation - can cause profound bradycardia)
- High-degree AV block or sick sinus syndrome (without pacemaker)
- WPW + preexcited AF/flutter (relative - can trigger fast ventricular response via AP)
- Severe asthma (can trigger bronchospasm - use with caution)
- IV theophylline/caffeine (competitive antagonists - larger doses needed)
- Dipyridamole POTENTIATES adenosine (blocks degradation) - use much smaller dose (1-2 mg)
Special note in WPW/preexcited tachycardia: If the tachycardia is irregular and wide-complex, strongly suspect preexcited AF. DO NOT give adenosine - it removes AV nodal block and can cause life-threatening acceleration via the AP. Use DC cardioversion or IV procainamide instead.
STEP 4: If Adenosine Fails (Second-Line Pharmacologic)
Option A: Verapamil (Non-DHP Calcium Channel Blocker)
- Dose: 5 mg IV over 2 minutes; repeat 5-10 mg IV after 15-30 minutes if needed; maximum 20 mg
- Mechanism: L-type Ca²⁺ channel blockade → slows AV nodal conduction
- Effective in ~90% of AV node-dependent SVT
- Side effects: Hypotension (can be significant), bradycardia
- Contraindications: Hypotension, wide-complex tachycardia (it can cause cardiovascular collapse in VT), WPW + AF, heart failure with reduced EF, patients on beta-blockers (risk of severe bradycardia and heart block)
Option B: Diltiazem (Non-DHP CCB)
- Dose: 0.25 mg/kg IV over 2 minutes (typical 15-20 mg); if inadequate, 0.35 mg/kg after 15 minutes
- Maintenance infusion: 5-15 mg/hour
- Similar efficacy to verapamil, possibly less hypotension
Option C: Beta-Blockers
- Metoprolol: 5 mg IV over 2 minutes, repeat every 5 minutes up to 15 mg total
- Esmolol: 500 mcg/kg IV bolus over 1 minute, then 50-200 mcg/kg/min infusion (ultra-short acting - excellent for titration)
- Mechanism: Beta-1 blockade → decreases AV node conduction velocity and automaticity
- Contraindications: Active bronchospasm/severe asthma, acute decompensated heart failure, bradycardia, hypotension, cocaine toxicity
Verapamil + Beta-blocker together = DANGEROUS (profound bradycardia/AV block/hypotension). Never combine.
STEP 5: Hemodynamically Unstable or Drug-Refractory SVT
Synchronized DC Cardioversion
- Energy: Start at 50-100 J biphasic (or 100-200 J monophasic) - lower energies often effective for SVT vs. VT
- "Synchronized" = machine times the shock to the R wave (avoids delivering shock during T wave which can cause VF)
- Sedate conscious patients (IV benzodiazepine ± propofol)
- Have crash cart, intubation equipment ready
- Rarely needed for AVNRT/AVRT as adenosine almost always works
SUMMARY TABLE: Acute Treatment of Stable SVT
| Step | Treatment | Dose | Notes |
|---|---|---|---|
| 1 | Vagal maneuvers | Valsalva / carotid massage | Do supine; teach patient for home use |
| 2 | Adenosine | 6 mg IV bolus → 12 mg → 12 mg | Rapid push + flush; warn about side effects |
| 3 | Verapamil | 5 mg IV over 2 min (repeat to max 20 mg) | Avoid if hypotension or wide complex |
| 3 | Diltiazem | 0.25 mg/kg IV over 2 min | Maintenance infusion available |
| 3 | Metoprolol | 5 mg IV q5min up to 15 mg | |
| 3 | Esmolol | 500 mcg/kg bolus → infusion | Titratable, short-acting |
| 4 | DC cardioversion | 50-100 J synchronized biphasic | For instability or drug failure |
CHAPTER 9: LONG-TERM / CHRONIC MANAGEMENT
After the acute episode is terminated, you must address the question: what do we do next?
Infrequent, well-tolerated episodes with minimal symptoms:
- Reassurance and education
- Teach the Valsalva maneuver for home use
- Avoid known triggers (caffeine, alcohol, stimulants)
- Pill-in-the-pocket: oral verapamil or diltiazem for self-termination of episodes
Frequent, symptomatic, or patient preference for definitive therapy:
Option 1: Catheter Ablation (TREATMENT OF CHOICE for recurrent SVT)
For AVNRT: Radiofrequency ablation of the slow pathway (posterior approach in the Triangle of Koch, near the CS ostium)
- Success rate: > 95% in experienced centers
- Complication: AV block in 0.1-0.4% (risk of needing a permanent pacemaker)
- A randomized trial confirmed superiority of ablation over antiarrhythmics: at 5 years, 0% ablation patients had recurrence requiring hospitalization vs. > 75% medical arm by 2 years
- Pediatric preference: Cryoablation (lower AV block risk, but higher recurrence rate)
For AVRT: Ablation of the accessory pathway
- Location determined by delta wave morphology and EPS
- High success rate; recurrence ~5%
For AT: Ablation of the focal ectopic site
- Requires mapping during EP study
Option 2: Long-Term Medical Therapy (if patient declines ablation)
| Drug | Class | Dose | Target |
|---|---|---|---|
| Verapamil | Non-DHP CCB | 120-360 mg/day oral (long-acting) | Rate control, circuit suppression |
| Diltiazem | Non-DHP CCB | 120-360 mg/day oral | Rate control, circuit suppression |
| Metoprolol | Beta-blocker | 25-200 mg/day oral (long-acting) | Rate control, circuit suppression |
| Atenolol | Beta-blocker | 25-100 mg/day oral | |
| Flecainide | Class IC antiarrhythmic | 50-150 mg twice daily | Na+ channel block; maintain SR |
| Propafenone | Class IC antiarrhythmic | 150-300 mg 3x/day | Na+ channel block |
| Sotalol | Class III | 80-160 mg twice daily | K+ channel block; maintain SR |
Note: Medical therapy reduces frequency and duration but rarely abolishes AVNRT completely. 20-50% of patients discontinue due to inefficacy or side effects. Ablation is strongly preferred for young patients, athletes, and those wanting definitive cure.
Flecainide/propafenone are contraindicated if structural heart disease is present (increased mortality - CAST trial).
CHAPTER 10: SPECIAL SCENARIOS - THE EXAM FAVORITES
WPW with AF (the Dangerous One)
- Wide, irregular, fast tachycardia (can reach 300 bpm)
- DO NOT give adenosine, verapamil, diltiazem, or digoxin
- These drugs block the AV node but leave the accessory pathway unblocked - AF conducts rapidly via AP → VF
- CORRECT TREATMENT:
- Unstable: Immediate DC cardioversion
- Stable: IV procainamide (blocks accessory pathway conduction) or ibutilide
- Long-term: Catheter ablation of accessory pathway
Wide-Complex Tachycardia - The Core Rule
"Wide complex tachycardia is VT until proven otherwise"
Differential: VT vs. SVT with aberrancy (bundle branch block) vs. preexcited tachycardia
- Never give verapamil for wide-complex tachycardia of unknown origin - if it's VT, verapamil causes cardiovascular collapse
- A trial of IV adenosine is reasonable for regular wide-complex tachycardia in a stable patient to help differentiate
SVT in Pregnancy
- Most SVTs are hemodynamically tolerated
- Adenosine is safe in pregnancy (does not cross placenta significantly)
- DC cardioversion is also safe in pregnancy (fetal monitoring required)
- Avoid: beta-blockers (fetal bradycardia/growth restriction), amiodarone (fetal thyroid toxicity)
- Verapamil is relatively safe in second/third trimester
SVT in Pediatrics / Infants
- Rate > 220 bpm in infant or > 180 bpm in child = suspicious for SVT
- Vagal maneuver: Ice bag to face (diving reflex)
- Adenosine: 0.1 mg/kg IV rapid bolus (maximum 6 mg first dose; 0.2 mg/kg for second dose, max 12 mg)
- AVRT with WPW most common mechanism in this age group
CHAPTER 11: MASTER MEMORY AID
"SVT PATHWAY" - what I want you to memorize:
S - Site: Above bundle of His (AV node, atria)
V - Varieties: AVNRT (most common), AVRT, AT
T - Triangle of Koch: AVNRT slow pathway ablation here
P - P waves: Buried/pseudo-r' (AVNRT); after QRS (orthodromic AVRT); before QRS (AT)
A - Adenosine: 6 mg → 12 mg → 12 mg rapid IV bolus (first-line drug)
T - Termination by AV block = AV node-dependent SVT (AVNRT/AVRT)
H - Hemodynamic instability = immediate synchronized cardioversion
W - WPW with AF: No AV nodal blockers! Use procainamide/DC cardioversion
A - Ablation: >95% success for AVNRT (slow pathway); definitive cure
Y - Your long-term Rx: Beta-blocker or CCB if no ablation
CHAPTER 12: THE EXAMINER'S FAVORITE QUESTIONS
Q: A 28-year-old woman presents with sudden-onset palpitations at 180 bpm, regular narrow QRS, pseudo-r' in V1. Most likely diagnosis?
A: Typical AVNRT (slow-fast). The pseudo-r' in V1 is the retrograde P wave buried at the end of the QRS.
Q: Same patient, adenosine 6 mg given - brief termination but SVT restarts. What next?
A: Adenosine 12 mg. If that fails, verapamil 5 mg IV.
Q: ECG shows short PR, delta wave, wide QRS. Patient develops fast irregular wide-complex tachycardia at 280 bpm. Management?
A: WPW with AF. Do NOT give adenosine, verapamil, or digoxin. Give synchronized DC cardioversion if unstable; IV procainamide if stable. Refer for accessory pathway ablation.
Q: During adenosine infusion for SVT, the rate transiently slows, P waves become visible at a regular rate of 250 bpm with sawtooth pattern, then SVT resumes. Diagnosis?
A: Atrial flutter (adenosine exposed the flutter waves by blocking AV node conduction). Adenosine did NOT terminate because the AV node is not in the circuit.
Q: What is the target of ablation in AVNRT?
A: The slow pathway (posterior AV nodal extension in the Triangle of Koch, near coronary sinus ostium).
Q: Name one drug that potentiates adenosine and one that blocks it.
A: Dipyridamole potentiates (blocks adenosine deaminase - use smaller dose). Theophylline and caffeine block it (competitive A1 receptor antagonists - larger dose needed).
SOURCES
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 256: PSVT and WPW
- Braunwald's Heart Disease, Chapters on AVNRT and Treatment of AVNRT
- Tintinalli's Emergency Medicine, Chapter 18: ECG Features of PSVT
- Rosen's Emergency Medicine, Chapter 65: Atrioventricular Nodal Reentrant Tachycardia
- Washington Manual of Medical Therapeutics: AVNRT and AVRT
- Harriet Lane Handbook (Pediatrics): SVT management in children
That is your complete lecture on SVT. Study the mechanisms first - if you understand WHY the circuit exists and WHY the ECG looks the way it does, the treatment follows logically. Memorize the adenosine protocol cold - it comes up on every exam and every clinical rotation. And never forget the WPW with AF trap - it is the one SVT that can kill if you treat it the wrong way.
This is a shared conversation. Sign in to Orris to start your own chat.