WBC morphology
Reading File
search_medical_text
WBC white blood cell morphology types normal abnormal
search_medical_image
WBC white blood cell morphology peripheral blood smear
GradeResponse
GradeResponse
Based on my knowledge and the retrieved content, here is a comprehensive overview of WBC Morphology.
White Blood Cell (WBC) Morphology
Normal WBC Types on Peripheral Smear
| Cell Type | Size | Nucleus | Cytoplasm / Granules | Normal % |
|---|---|---|---|---|
| Neutrophil | 12–15 µm | 2–5 lobes, connected by thin filaments | Pale pink; fine lilac (azurophilic) granules | 50–70% |
| Band Neutrophil | 12–15 µm | Horseshoe/U-shaped, unsegmented | Same as mature neutrophil | 0–5% |
| Eosinophil | 12–17 µm | Bi-lobed | Large, bright orange-red granules | 1–4% |
| Basophil | 10–14 µm | Bi/tri-lobed (often obscured) | Large, dark purple-blue granules (may overlay nucleus) | 0–1% |
| Monocyte | 14–20 µm (largest normal WBC) | Kidney/horseshoe-shaped, folded | Gray-blue, vacuolated; fine azurophilic granules | 2–8% |
| Lymphocyte | 7–18 µm | Large, round, dense; scant halo of cytoplasm | Pale blue, scant | 20–40% |
| Plasma Cell | 8–20 µm | Eccentric, "clock-face" chromatin | Deep blue; perinuclear hof (pale zone) | Rare in blood |
Abnormal WBC Morphology
Neutrophil Abnormalities
| Finding | Morphology | Clinical Association |
|---|---|---|
| Hypersegmentation | ≥5 lobes or ≥5% of neutrophils with ≥5 lobes | Megaloblastic anemia (B12/folate deficiency), renal failure |
| Toxic granulation | Coarse, dark primary granules | Severe infection, sepsis, inflammatory states |
| Döhle bodies | Small, pale blue cytoplasmic inclusions (periphery) | Infection, burns, pregnancy, cytotoxic therapy |
| Vacuolization | Cytoplasmic vacuoles | Sepsis, alcohol toxicity, ethylene glycol poisoning |
| Pseudo-Pelger-Huët | Bilobed "pince-nez" or unilobed nucleus | Myelodysplastic syndrome (MDS), drug effect |
| Pelger-Huët anomaly (hereditary) | Same bilobed appearance, but benign | Autosomal dominant, no clinical significance |
| Left shift | Increased bands ± metamyelocytes, myelocytes in blood | Infection, inflammation, leukemoid reaction, CML |
| Auer rods | Pink/red needle-like cytoplasmic inclusions | AML (pathognomonic) |
Lymphocyte Abnormalities
| Finding | Morphology | Clinical Association |
|---|---|---|
| Reactive (atypical) lymphocytes | Large, irregular, abundant pale cytoplasm that indents around RBCs | EBV (infectious mononucleosis), CMV, viral hepatitis, drug reactions |
| Smudge cells | Disrupted, smeared nucleus | CLL (fragile lymphocytes) |
| Large granular lymphocytes (LGL) | Abundant cytoplasm with azurophilic granules | LGL leukemia, NK-cell disorders, reactive states |
| Hairy cells | Irregular cytoplasmic projections ("hairy" outline) | Hairy cell leukemia |
Monocyte Abnormalities
| Finding | Clinical Association |
|---|---|
| Monocytosis with immature forms | Chronic myelomonocytic leukemia (CMML), AML-M4/M5 |
| Marked vacuolization | Infection, storage disorders |
Blasts
| Feature | Description |
|---|---|
| Myeloblast | Large cell, fine chromatin, prominent nucleoli (2–5), scant cytoplasm ± Auer rods |
| Lymphoblast | Similar to myeloblast but nucleoli less prominent; immunophenotyping required |
| Blasts in peripheral blood | Always abnormal → suggest acute leukemia; requires urgent workup |
Key Morphologic Patterns and Their Diagnoses
| Pattern on Smear | Diagnosis to Consider |
|---|---|
| Hypersegmented neutrophils | B12 / folate deficiency |
| Toxic granulation + Döhle bodies + left shift | Sepsis, severe bacterial infection |
| Atypical lymphocytes (>10%) | EBV mononucleosis |
| Smudge cells | CLL |
| Auer rods | AML |
| Pseudo-Pelger-Huët + dysplastic cells | MDS |
| Circulating blasts | Acute leukemia |
| Leukoerythroblastic picture (blasts + nucleated RBCs + tear-drop cells) | Bone marrow infiltration (metastatic cancer, myelofibrosis) |
| Hairy cells | Hairy cell leukemia |
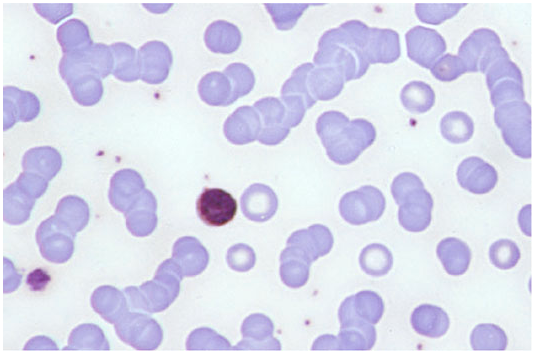
Peripheral Blood Smear (Harrison's, p. 1724)
The image below illustrates a representative peripheral smear under Wright/Giemsa stain, with a lymphocyte visible among normal erythrocytes:
Approach to WBC Morphology on a Smear
- Identify all cell types present — confirm normal lineages and proportions
- Look for left shift — presence of bands, metamyelocytes, myelocytes
- Check for blasts — any blast = urgent pathology until proven otherwise
- Assess neutrophil quality — toxic changes, hypersegmentation, Pelger-Huët
- Examine lymphocytes — reactive vs. neoplastic (smudge cells, hairy cells, LGLs)
- Note monocytes — excess or immature forms
- Correlate with CBC — absolute counts + morphology together guide diagnosis
This is a shared conversation. Sign in to Orris to start your own chat.