Roa
It seems like your message got cut off. Could you finish your thought? Were you asking about:
- ROA (Return on Assets)?
- Roa as a name or place?
- Something medical or clinical?
Let me know what you meant!
Road traffic accident ATLS PROTOCOL
Reading File
search_medical_text
ATLS Advanced Trauma Life Support primary survey ABCDE protocol
search_medical_text
road traffic accident trauma management secondary survey resuscitation
search_medical_image
ATLS trauma primary survey algorithm flowchart
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive breakdown of the ATLS Protocol as applied to Road Traffic Accidents (RTAs):
ATLS Protocol in Road Traffic Accidents
Advanced Trauma Life Support (ATLS) provides a systematic, time-critical framework for managing trauma patients. The core principle is "time dependence" — identify life-threatening problems rapidly and treat them in order of priority (Bailey & Love's Surgery, 28th Ed., p. 365).
Scene & Pre-Hospital
- Ensure scene safety (traffic control, fire hazards)
- C-spine immobilization immediately — assume cervical injury in all RTAs
- Activate trauma team / tertiary trauma center alert
- Hemorrhage control (direct pressure, tourniquets for limb injuries)
- Rapid transport — "load and go" for unstable patients
PRIMARY SURVEY — A B C D E
The primary survey is performed simultaneously with resuscitation. The goal is to identify and treat immediately life-threatening conditions.
A — Airway (with C-spine Protection)
| Action | Detail |
|---|---|
| Assess patency | Look, listen, feel; check for obstruction (blood, vomit, foreign body) |
| C-spine control | Manual in-line stabilization; apply hard collar |
| Open airway | Jaw thrust (NOT head-tilt in trauma) |
| Definitive airway | Endotracheal intubation if GCS ≤8, airway compromise, or risk of obstruction |
| Surgical airway | Cricothyroidotomy if intubation fails |
B — Breathing & Ventilation
Expose the chest; assess respiratory rate, chest movement, and SpO₂.
| Life-Threatening Condition | Signs | Treatment |
|---|---|---|
| Tension pneumothorax | Absent breath sounds, tracheal deviation, hypotension | Immediate needle decompression (2nd ICS, MCL) → chest drain |
| Open pneumothorax | Sucking chest wound | 3-sided occlusive dressing → chest drain |
| Massive hemothorax | Dullness, hemodynamic shock | Large-bore chest drain |
| Flail chest + pulmonary contusion | Paradoxical movement, hypoxia | O₂, ventilatory support |
All trauma patients receive high-flow O₂ (15 L/min via non-rebreather mask).
C — Circulation & Hemorrhage Control
The leading cause of preventable death in RTAs is uncontrolled hemorrhage.
- 2 large-bore IV cannulas (14–16G, antecubital) or IO access
- Send bloods: FBC, U&E, clotting, crossmatch, ABG, β-hCG (females)
- Massive transfusion protocol if needed: packed RBCs : FFP : platelets = 1:1:1
- Permissive hypotension (SBP ~80–90 mmHg) until surgical hemorrhage control — avoid aggressive crystalloid
- Tranexamic acid: 1g IV within 3 hours of injury (CRASH-2 Trial)
| Hemorrhage Class | Blood Loss | HR | BP | RR | GCS |
|---|---|---|---|---|---|
| Class I | <750 mL | <100 | Normal | 14–20 | Normal |
| Class II | 750–1500 mL | 100–120 | Normal/↓ | 20–30 | Anxious |
| Class III | 1500–2000 mL | 120–140 | ↓ | 30–40 | Confused |
| Class IV | >2000 mL | >140 | Very ↓ | >35 | Lethargic |
D — Disability (Neurological Status)
- GCS (Eyes + Verbal + Motor, max 15)
- Pupils: size, equality, reactivity
- AVPU scale (Alert / Voice / Pain / Unresponsive) — quick bedside tool
- Blood glucose (rule out hypoglycemia mimicking altered consciousness)
E — Exposure & Environment
- Fully undress the patient (cut clothing)
- Log-roll with C-spine control to examine posterior
- Prevent hypothermia: warm blankets, warm IV fluids — the "lethal triad" of hypothermia + acidosis + coagulopathy must be avoided
ADJUNCTS TO PRIMARY SURVEY
| Investigation | Purpose |
|---|---|
| eFAST ultrasound | Pericardial effusion, pneumothorax, hemoperitoneum |
| CXR (AP) | Pneumo/hemothorax, mediastinal widening (aortic injury), rib fractures |
| Pelvic XR | Pelvic ring disruption (major hemorrhage source) |
| ECG | Cardiac contusion, arrhythmia |
| Urinary catheter | Urine output monitoring (0.5 mL/kg/hr target); exclude urethral injury first |
| NG tube | Gastric decompression; avoid if base of skull fracture suspected |
RESUSCITATION PHASE
Runs concurrently with the primary survey:
- Airway secured
- IV access + fluids / blood products
- Chest drain if indicated
- Pelvic binder for suspected pelvic fracture
- Limb splinting
- Monitor: SpO₂, EtCO₂, BP, HR, urine output, temperature
SECONDARY SURVEY
Performed only after the primary survey is complete and the patient is hemodynamically stable (Bailey & Love's Surgery, 28th Ed., p. 296).
- AMPLE history: Allergies, Medications, Past history, Last meal, Events/mechanism
- Head-to-toe examination: scalp, face, ears (hemotympanum), eyes, neck, chest, abdomen, perineum, back, limbs, neurology
- Mechanism-specific injuries in RTAs:
- Seatbelt sign → bowel/mesenteric/lumbar spine injury
- Steering wheel impact → aortic injury, cardiac contusion, sternal fracture
- Pedestrian hit → tibial fracture (bumper), femoral/pelvic fracture, head injury
- Ejection from vehicle → high-energy, multisystem injury
TERTIARY SURVEY
- Performed at 24–72 hours after admission
- Repeat full examination to detect missed injuries
- Review all imaging
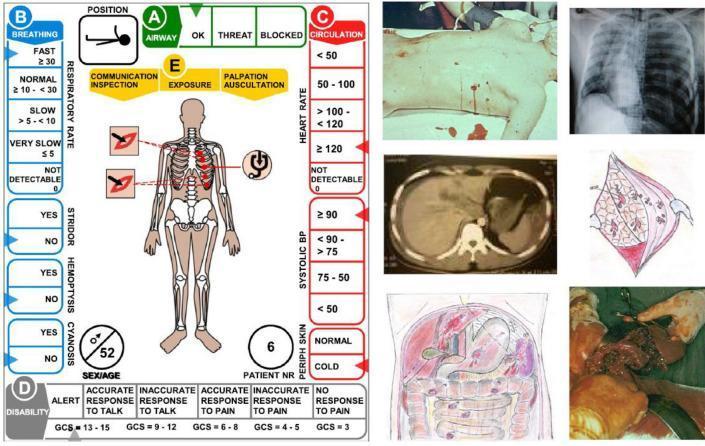
ATLS Casualty Card (ABCDE Training Reference)
Key Mnemonics
| Mnemonic | Meaning |
|---|---|
| ABCDE | Airway, Breathing, Circulation, Disability, Exposure |
| AMPLE | Allergies, Medications, Past Hx, Last meal, Events |
| FAST/eFAST | Focused Assessment with Sonography in Trauma |
| Lethal Triad | Hypothermia + Acidosis + Coagulopathy |
References:
- Bailey & Love's Short Practice of Surgery, 28th Edition, pp. 296, 365
- ATLS Student Course Manual, 10th Edition (American College of Surgeons)
- CRASH-2 Trial — Tranexamic Acid in Trauma
This is a shared conversation. Sign in to Orris to start your own chat.