Short note answer 5 marks mbbs on decorticate and decrebrate rigidity
Reading File
Finding Sources
Searching the Web
decorticate decerebrate rigidity MBBS neurology short note
Reading File
Reading File
Reading File
Reading File
I have everything needed. Here is the complete short note answer:
Decorticate and Decerebrate Rigidity
Definition
Decorticate and decerebrate rigidity (posturing) are stereotyped, abnormal motor responses seen in comatose patients, reflecting severe disruption of descending motor pathways. They may occur spontaneously or be provoked by noxious stimuli, and represent progressive rostrocaudal deterioration of the nervous system.
Historical Background
First described by Sherrington in cats and monkeys after transection of the brainstem at the intercollicular level. These experimental patterns were later recognized in humans with brain injuries. The anatomical dividing point is the red nucleus in the upper midbrain.
1. Decorticate Rigidity (Abnormal Flexion Posturing)
Level of lesion: Above the red nucleus - dysfunction of the forebrain extending down to the rostral midbrain (cerebral white matter, internal capsule, thalamus / diencephalon-midbrain junction).
Clinical features:
- Upper extremities: flexion of arm, wrist, and fingers + adduction at shoulder
- Lower extremities: extension, internal rotation, and plantar flexion
- Head may be extended
Mechanism: Loss of corticospinal and corticobulbar input; rubrospinal tract remains intact, causing flexion dominance in the arms. The facilitatory reticulospinal pathway drives extension in the legs.
Mnemonic: "deCORticate = brings arms to CORE (chest)" - arms flex inward.
2. Decerebrate Rigidity (Abnormal Extension Posturing)
Level of lesion: At or below the red nucleus - damage to the lower midbrain and upper pons (intercollicular level).
Clinical features:
- Upper extremities: extension, pronation of forearms, fingers flexed
- Lower extremities: extension, internal rotation, plantar flexion (toes pointed inward)
- Opisthotonus (neck and back extended), jaw clenching
Mechanism: Transection interrupts corticospinal, corticobulbar, and rubrospinal tracts. Excitatory drive from ascending sensory pathways to the excitatory reticulospinal pathway leads to hyperactivity of extensor muscles in all four limbs. The spasticity is due to facilitation of the stretch reflex via the gamma loop (gamma motor neurons -> Ia spindle afferents -> alpha motor neurons).
Mnemonic: "dEcErEbratE = lots of E's = EXTENSION" - arms and legs extend outward.
Key Differences at a Glance
| Feature | Decorticate | Decerebrate |
|---|---|---|
| Lesion level | Above red nucleus (rostral midbrain/forebrain) | At/below red nucleus (lower midbrain-upper pons) |
| Arms | Flexed, adducted | Extended, pronated |
| Legs | Extended | Extended |
| Prognosis | Serious but less severe | More ominous |
| Mechanism | Rubrospinal tract intact | Rubrospinal also disrupted |
Diagram (Ganong's Physiology)
Below: A = Decerebrate (upper pontine/lower midbrain damage); B = Decorticate (upper midbrain damage)
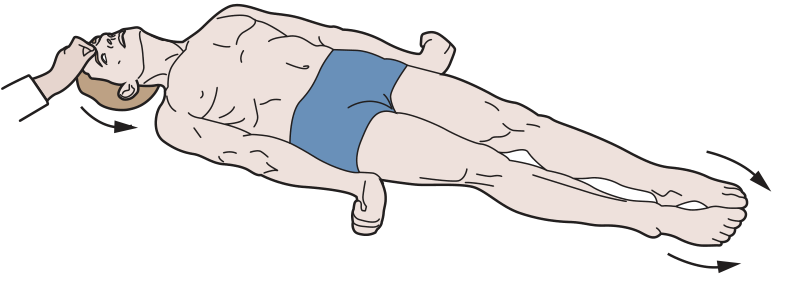
Decerebrate posturing (A): All four limbs extended, forearms pronated, toes inward
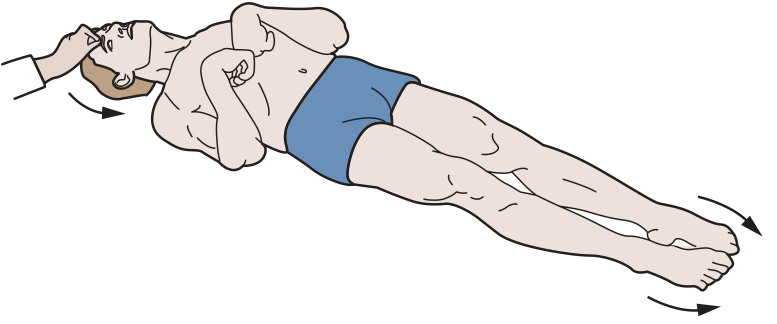
Decorticate posturing (B): Upper limbs flexed, lower limbs extended
Etiology (Common Causes)
- Traumatic brain injury (TBI) - most common
- Cerebral hemorrhage or infarct
- Uncal herniation from supratentorial mass (tumor, hematoma)
- Anoxic brain injury / hypoglycemia
- Hepatic coma (rare)
- Severe drug/alcohol intoxication (rare)
Clinical Significance
- Rostrocaudal deterioration: Progression from decorticate -> decerebrate posturing indicates downward herniation and worsening brainstem compromise.
- Decerebrate -> flaccidity: If posturing gives way to complete flaccidity, the lesion has descended below the vestibular nuclei, indicating impending brain death.
- Both responses are ominous in the setting of head injury, carrying high mortality.
- GCS scoring: Decorticate = M3 (abnormal flexion); Decerebrate = M2 (extension) on the motor component of the Glasgow Coma Scale.
- Metabolic causes (anoxia, hypoglycemia, hepatic coma) can produce either pattern and may be reversible.
Sources: Ganong's Review of Medical Physiology 26e, p. 248-250; Adams & Victor's Principles of Neurology 12e; Plum & Posner's Diagnosis and Treatment of Stupor and Coma.
Stages i Of spinal shock
Finding Sources
Searching the Web
stages of spinal shock Ditunno 4 phases MBBS neurology
Reading File
Reading File
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK448163
Reading File
Reading Web Page
https://en.wikipedia.org/wiki/Spinal_shock
I now have comprehensive information from multiple authoritative sources. Here is the complete short note:
Stages of Spinal Shock
Definition
Spinal shock is the sudden, complete suppression of all spinal cord functions (motor, sensory, reflex, and autonomic) below the level of an acute spinal cord injury (SCI). The word "shock" here does NOT refer to circulatory collapse - it describes physiological depression of isolated spinal cord segments. It must not be confused with neurogenic shock (hemodynamic instability from loss of sympathetic tone).
Cause: Sudden interruption of descending supraspinal facilitatory tracts - primarily the reticulospinal, vestibulospinal, and corticospinal tracts - that normally keep spinal motor neurons in a state of tonic excitability.
Classical Description: Two Stages (Adams & Victor)
Stage 1 - Stage of Spinal Shock (Areflexia)
Onset: Immediately after complete cord transection
Duration: Days to weeks (rarely permanent); in humans, 2 weeks to several months
Features:
- Flaccid paralysis below the level of lesion
- Complete loss of all deep tendon reflexes (areflexia)
- Loss of all sensation below the lesion
- Bladder: atonic detrusor, contracted sphincter → overflow incontinence
- Bowel: paralytic ileus, fecal retention
- Autonomic: hypotension (BP may drop to 40 mmHg), loss of vasomotor tone, loss of sweating and piloerection below lesion
- Genital reflexes abolished (bulbocavernosus, cremasteric)
- Priapism may occur
First reflex to return: Bulbocavernosus reflex (polysynaptic), followed by anal reflex → this signals the END of spinal shock
Stage 2 - Stage of Heightened Reflex Activity (Spasticity)
Onset: Weeks after injury
Features:
- Spasticity gradually replaces flaccidity
- Deep tendon reflexes return and become hyperactive (hyperreflexia)
- Extensor plantar response (Babinski sign)
- Mass reflex (flexor spasms in response to cutaneous stimuli)
- Bladder and bowel become spastic (automatic/reflex bladder)
- Autonomic dysreflexia may develop (in lesions above T6)
Modern 4-Phase Model (Ditunno et al., 2004)
This is the current standard model taught in most updated curricula:
| Phase | Timing | Examination Finding | Underlying Mechanism |
|---|---|---|---|
| Phase 1 | 0-1 day | Areflexia / Hyporeflexia | Loss of descending facilitation |
| Phase 2 | 1-3 days | Initial reflex return (polysynaptic first) | Denervation supersensitivity (↑ receptor expression) |
| Phase 3 | 1-4 weeks | Initial hyperreflexia | Axon-supported synapse growth (shorter axons, interneurons) |
| Phase 4 | 1-12 months | Hyperreflexia + Spasticity | Soma-supported synapse growth (longer axons, growth factors) |
Phase 1 - Areflexia (0-1 day)
- All reflexes below SCI are absent or markedly reduced
- Neurons lose supraspinal excitatory input → hyperpolarization → unresponsive to stimuli
- Flaccid paralysis, sensory loss, autonomic dysfunction
Phase 2 - Return of Polysynaptic Reflexes (1-3 days)
- Polysynaptic reflexes return first (e.g., bulbocavernosus reflex)
- Monosynaptic DTRs not yet restored
- Mechanism: denervation supersensitivity - upregulation of neurotransmitter receptors on post-synaptic neurons
- Recovery is polysynaptic → monosynaptic (NOT rostral to caudal as previously believed)
Phase 3 - Hyperreflexia Begins (1-4 weeks)
- Monosynaptic DTRs return and become exaggerated
- Interneuron axon sprouting creates new synapses below the injury
- Early spasticity appears
Phase 4 - Established Spasticity (1-12 months)
- Full hyperreflexia and spasticity
- Soma-mediated sprouting: longer axons with soma-transported growth factors form new synaptic connections
- Autonomic dysreflexia may appear in high thoracic/cervical lesions
Order of Reflex Return (Guyton & Hall)
- Stretch reflexes (DTRs) - first monosynaptic reflexes
- Flexor reflexes
- Postural antigravity reflexes
- Rudimentary stepping reflexes
Key Points for Exam
- Spinal shock is NOT neurogenic shock (do not confuse)
- Duration is longer in humans and higher primates than in lower animals
- The end of spinal shock is marked by return of the bulbocavernosus reflex
- Incomplete or slow-developing lesions produce little or no spinal shock
- Permanent spinal shock (no reflex recovery) occurs in ~5/29 cases (Kuhn) - suggests secondary vascular injury to cord segments below the lesion
- Above T6 injuries: neurogenic shock + spinal shock can coexist acutely; autonomic dysreflexia in the chronic phase
Sources: Adams & Victor's Principles of Neurology 12e; Guyton & Hall Medical Physiology; Ditunno JF et al., "Spinal shock revisited: a four-phase model," Spinal Cord, 2004 [PMID 15037862]; StatPearls - Spinal Shock (NIH/NCBI)
Classical decerevrate and ischemic rigidity
Finding Sources
Searching the Web
classical decerebrate rigidity vs ischemic rigidity alpha rigidity gamma rigidity difference physiology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
classical decerebrate rigidity ischemic rigidity Sherrington gamma loop alpha rigidity dorsal root section physiology
Reading File
Reading File
Reading File
Loading Image
Excellent - that's the perfect Ganong circuit diagram. I now have everything needed for a thorough answer.
Classical Decerebrate Rigidity vs. Ischemic (Alpha) Rigidity
This comparison is a classic physiology question distinguishing two types of decerebrate rigidity based on the neural mechanism involved - specifically whether the rigidity depends on the gamma loop or bypasses it through direct alpha motor neuron activation.
Background: Normal Motor Control
Extensor muscle tone is regulated by a balance of descending pathways:
| Pathway | Origin | Effect on Extensors |
|---|---|---|
| Pontine reticulospinal tract | Pons | Excitatory (++) |
| Lateral vestibulospinal tract (Deiters' nucleus) | Lateral vestibular nucleus | Excitatory (++) |
| Medullary reticulospinal tract | Medullary RF | Inhibitory (--) |
| Corticospinal, Rubrospinal, Corticoreticular | Cortex / Red nucleus | Drive inhibitory medullary RF |
Under normal conditions, the cortex and red nucleus tonically excite the medullary inhibitory reticular formation, counterbalancing the pontine excitatory drive.
Classical Decerebrate Rigidity (Gamma Rigidity)
Experimental Basis
First described by Sherrington (1898) in cats and monkeys by intercollicular transection - a cut between the superior and inferior colliculi, at the midcollicular level.
Mechanism
The transection interrupts:
- Corticospinal tract
- Corticobulbar tract
- Rubrospinal tract
- Corticoreticular fibers to medullary inhibitory RF
This leaves intact:
- Pontine excitatory reticulospinal tract
- Lateral vestibulospinal tract (Deiters' nucleus)
Result: The medullary inhibitory reticulospinal system becomes nonfunctional (loses cortical/rubral drive). The pontine excitatory and vestibulospinal systems now dominate unopposed → hyperactivity of extensor gamma (γ) motor neurons.
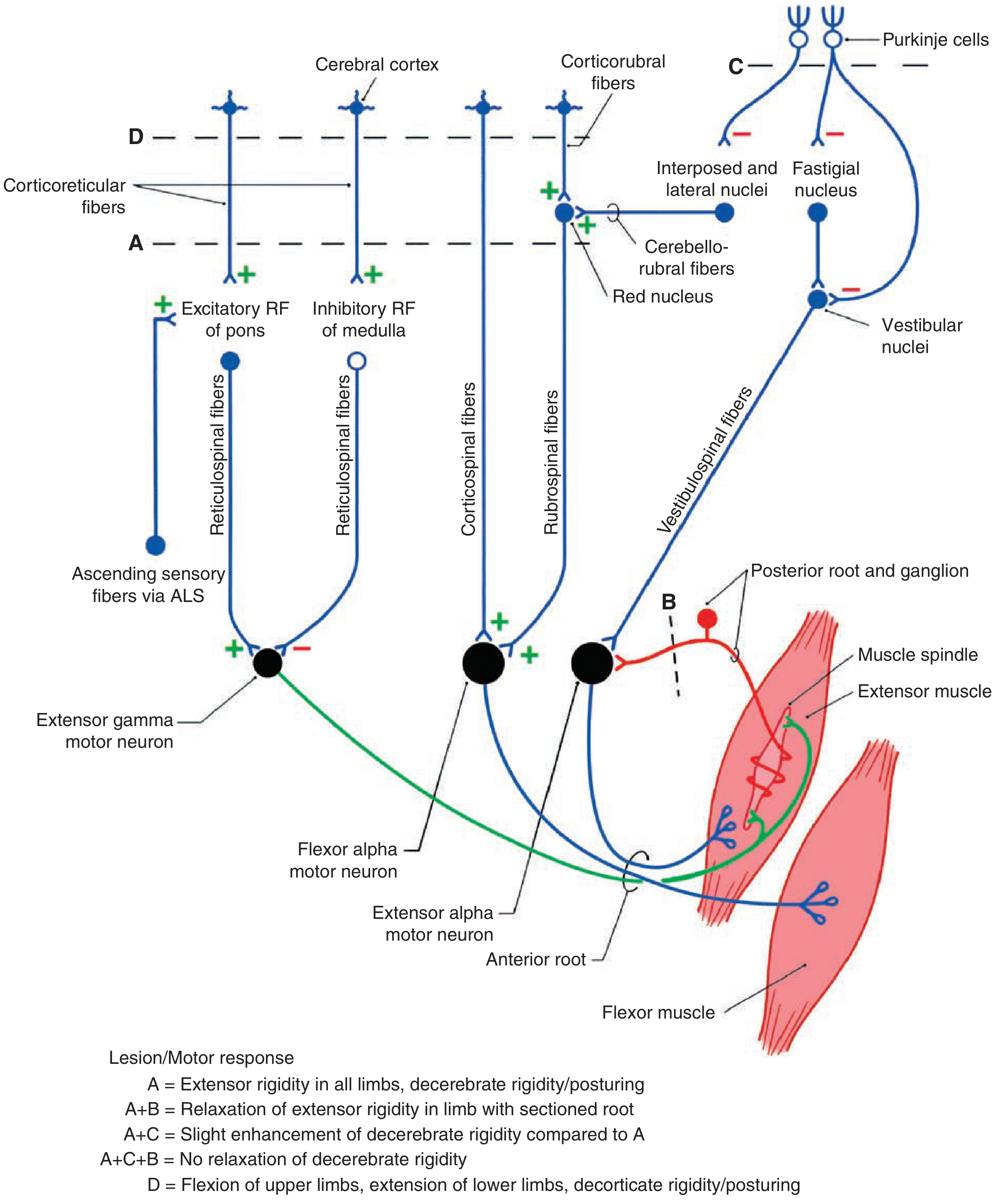
Figure (Ganong): A = intercollicular transection → decerebrate rigidity. A+B = dorsal root section abolishes rigidity. A+C = cerebellar anterior lobe removal enhances rigidity. A+C+B = rigidity NOT abolished by dorsal root section (alpha rigidity).
The Gamma Loop (Key Mechanism)
Reticulospinal excitation → γ-motor neurons activated → muscle spindle (intrafusal fibers) stretched → Ia afferent signals → α-motor neurons fired → extensor muscle contraction.
This is an indirect pathway: γ → spindle → Ia → α
Proof - Dorsal Root Section (Lissauer, Sherrington):
- Cutting the dorsal roots (section B in diagram) of a limb in a midcollicular decerebrate animal immediately abolishes the rigidity in that limb
- This is because dorsal root section interrupts the Ia afferent spindle feedback, breaking the gamma loop
- Therefore classical decerebrate rigidity is GAMMA rigidity - it depends on the intact gamma loop
Features of Classical Decerebrate Rigidity
| Feature | Detail |
|---|---|
| Lesion site | Intercollicular (between superior and inferior colliculi) |
| Antigravity muscles | Affected - neck, trunk, limb extensors |
| Abolished by | Dorsal root section, deafferentation |
| Dependent on | Gamma loop (γ → Ia spindle → α) |
| Inhibitory RF | Nonfunctional (lost cortical/rubral drive) |
| Type | Gamma (γ) rigidity |
Ischemic (Alpha) Rigidity - Decerebellate Rigidity
Experimental Basis
If the anterior lobe of the cerebellum is removed in a midcollicular decerebrate animal (lesion C in the Ganong diagram above), the extensor hyperactivity is greatly exaggerated (called decerebellate rigidity). This is the experimental model of ischemic/alpha rigidity.
Clinically, ischemic rigidity refers to decerebrate rigidity produced by global brainstem ischemia (e.g., cardiac arrest, severe anemia, or anoxia) where the entire brainstem, including the pontine and medullary reticular systems, is rendered ischemic - causing uncontrolled, direct alpha motor neuron activation.
Mechanism
Removing the cerebellar anterior lobe eliminates:
- Purkinje cell inhibitory output to the fastigial nucleus
- This disinhibits the fastigial nucleus → increased excitatory output → vestibular nuclei (Deiters') become hyperexcited
- This enormously enhances excitation of α-motor neurons directly (not via gamma loop)
In ischemic conditions, the massive neuronal excitation from ischemia itself drives direct α-motor neuron firing.
Proof - Dorsal Root Section Does NOT Abolish Ischemic Rigidity:
- Subsequent dorsal root section (B after A+C) does NOT reverse the rigidity
- This proves it is independent of the gamma loop - alpha motor neurons are being activated directly
- Therefore ischemic/decerebellate rigidity is ALPHA rigidity
Features of Ischemic (Alpha) Rigidity
| Feature | Detail |
|---|---|
| Lesion | Anterior cerebellar lobe removal / global brainstem ischemia |
| Mechanism | Direct α-motor neuron activation (independent of spindle) |
| Abolished by | Dorsal root section does NOT abolish it |
| Dependent on | Direct drive to α-motor neurons |
| Vestibular nuclei | Greatly hyperexcited |
| Type | Alpha (α) rigidity |
Key Comparison Table
| Feature | Classical Decerebrate Rigidity | Ischemic (Alpha) Rigidity |
|---|---|---|
| Also called | Gamma rigidity | Alpha rigidity / Decerebellate rigidity |
| Transection level | Intercollicular (mid-collicular) | Intercollicular + anterior cerebellar lobe removed (or global ischemia) |
| Mechanism | γ-motor neuron → Ia spindle afferent → α-motor neuron (gamma loop) | Direct α-motor neuron activation |
| Dorsal root section | Abolishes rigidity | Does NOT abolish rigidity |
| Severity | Less severe | More severe (exaggerated rigidity) |
| Cerebellar influence | Anterior lobe intact (inhibits fastigial → partially dampens rigidity) | Anterior lobe removed → fastigial disinhibited → Deiters' nucleus hyperactive |
| Clinical correlate | Intercollicular lesions, uncal herniation | Global anoxia, severe ischemia, phenytoin toxicity (rare) |
Summary Mnemonic
"Gamma - Gone with dorsal root section" (classical decerebrate - gamma rigidity is abolished by cutting dorsal roots) "Alpha - Always stays" (ischemic/alpha rigidity persists even after dorsal root section)
Clinical Points
- Both types produce the same posture: neck extended (opisthotonus), jaws clenched, arms and legs extended, forearms pronated, feet plantar flexed
- Classical decerebrate rigidity clinically correlates with midbrain/upper pontine lesions, herniation, or metabolic causes
- Ischemic/alpha rigidity is seen after cardiac arrest, severe hypoxia/anoxia and carries an extremely poor prognosis
- The distinction is experimentally important for understanding stretch reflex physiology and the role of the gamma loop
Sources: Ganong's Review of Medical Physiology 26e, pp. 248-250; Guyton & Hall Medical Physiology (Vestibular Nuclei, Decerebrate Rigidity); Costanzo Physiology 7e; StatPearls - Decerebrate Rigidity (NCBI)
This is a shared conversation. Sign in to Orris to start your own chat.