Thoracic duct
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Excellent. I now have comprehensive textbook content and two great diagrams. Let me compile the full answer.
Thoracic Duct
Overview
The thoracic duct is the largest and principal lymphatic vessel in the body, measuring 38-45 cm long and 2-5 mm in diameter. It serves as the common drainage channel for lymph from most of the body and returns it to the venous system. - Fischer's Mastery of Surgery, p. 2442; Gray's Anatomy for Students, p. 270
Course and Relations
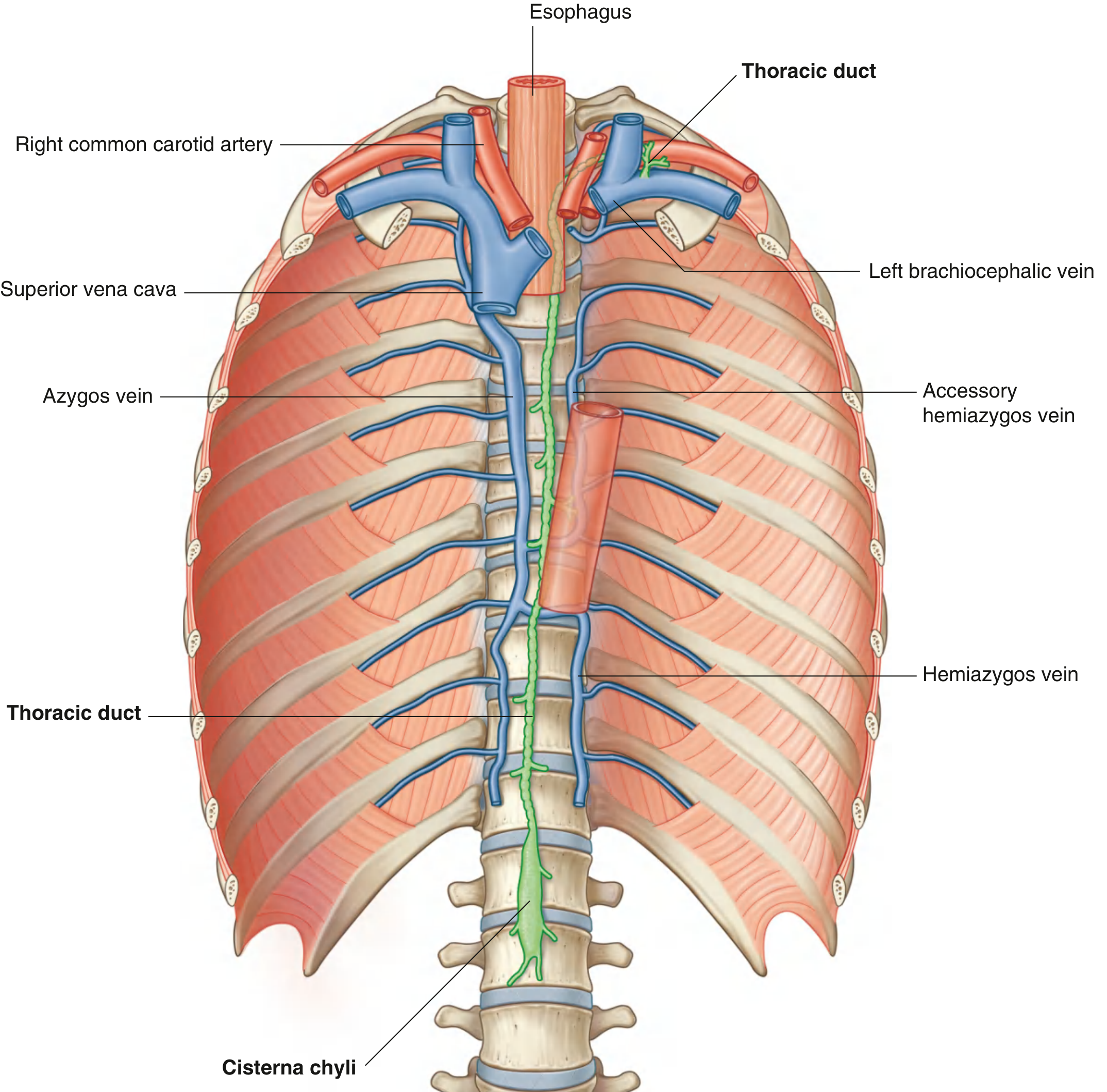
Fig. 3.106 - Thoracic Duct (Gray's Anatomy for Students)
The duct follows a well-defined course with key anatomical landmarks:
| Segment | Level | Relations |
|---|---|---|
| Origin | L1-L2 (retrocrural abdomen) | Cisterna chyli |
| Enters thorax | T12 (aortic hiatus) | Posterior to aorta |
| Posterior mediastinum | T12 - T5 | Right of midline: aorta (left), azygos vein (right), esophagus (anterior), vertebral bodies (posterior) |
| Crossover | T5 (TV) | Shifts from right to left of midline |
| Superior mediastinum / root of neck | T5 upward | Left of esophagus |
| Termination | Left venous angle | Junction of left internal jugular vein + left subclavian vein |
In the root of the neck, before entering the venous angle, the duct arches laterally and passes:
- Posterior to the carotid sheath
- Anterior to the thyrocervical trunk, phrenic nerve, and vertebral artery
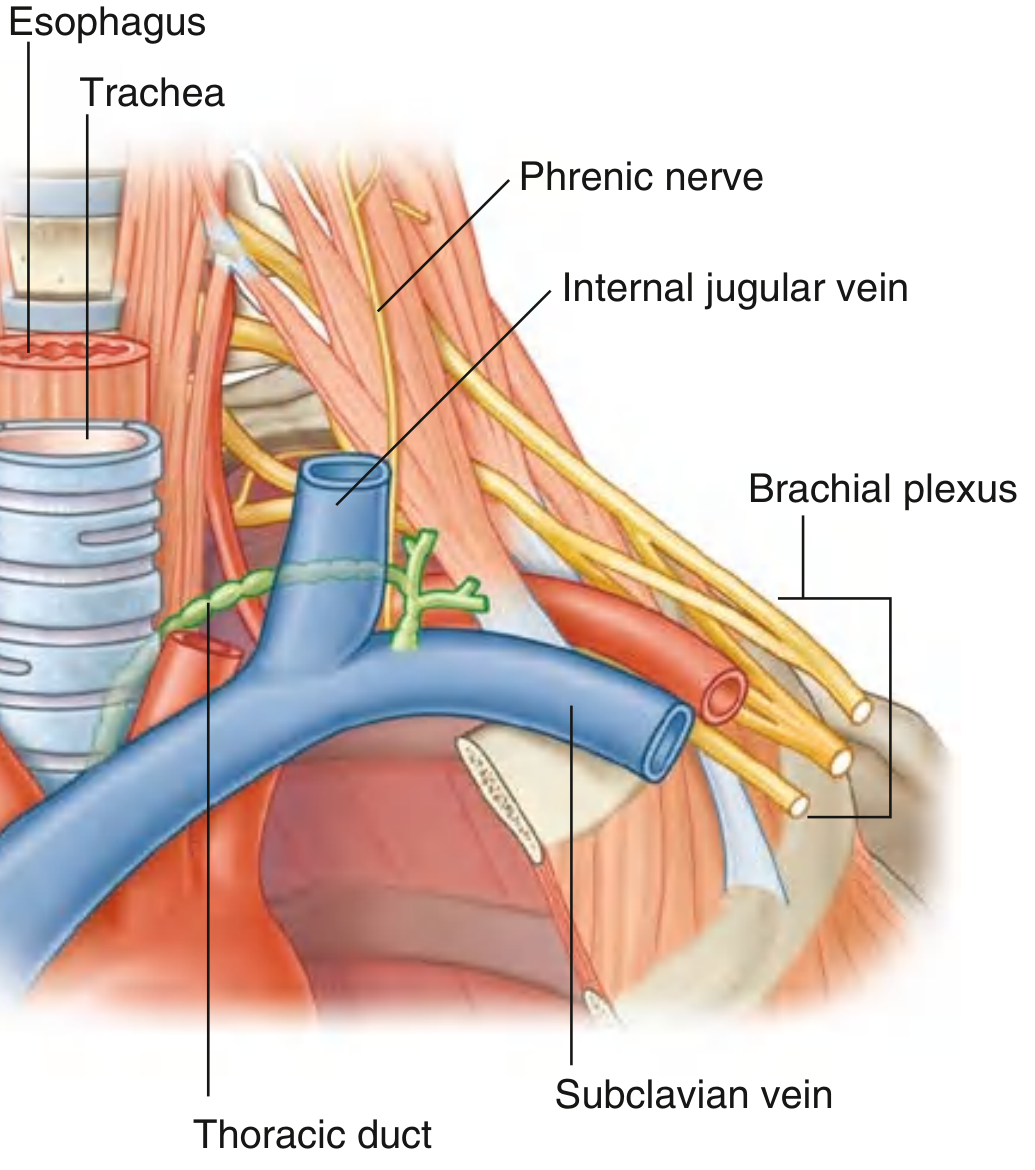
Fig. 8.198 - Thoracic Duct in the Root of the Neck (Gray's Anatomy for Students)
Drainage Territories
The thoracic duct drains all of the body except the right upper extremity, right breast, right lung, and right half of the head and neck (which drain via the right lymphatic duct). - Fischer's Mastery of Surgery
Specifically, the thoracic duct receives:
- Cisterna chyli (abdominal viscera, walls, pelvis, perineum, lower limbs)
- Lower 6-7 intercostal spaces (both sides)
- Upper left 5-6 intercostal spaces
- Posterior mediastinal lymph nodes
- Left jugular trunk (left head and neck)
- Left subclavian trunk (left upper limb)
- Occasionally: left bronchomediastinal trunk (left thoracic structures)
Termination - Right Side Comparison
On the right, a mirror arrangement drains into the right venous angle:
- Right jugular trunk (right head and neck)
- Right subclavian trunk (right upper limb)
- Right bronchomediastinal trunk (right thoracic structures)
These may unite into a single right lymphatic duct, or enter as three separate trunks - there is considerable variability. - Gray's Anatomy for Students, p. 1177
Development (Embryology)
The thoracic duct forms from:
- The caudal part of the right thoracic duct
- The anastomosis between the left and right thoracic ducts
- The cranial part of the left thoracic duct
Because of this complex developmental origin, there are many variations in its course and termination. The right lymphatic duct derives from the cranial part of the right thoracic duct. - The Developing Human, p. 885
Clinical Relevance
Chylothorax
Injury to the thoracic duct causes chyle (lymph rich in chylomicrons/triglycerides) to leak into the pleural space. Key diagnostic threshold: triglycerides >110 mg/dL is pathognomonic for chylothorax. - Fischer's Mastery of Surgery, p. 2442
Common causes: esophagectomy, neck dissection (level IV), thoracic surgery, trauma. The site most amenable to surgical ligation is where the duct enters the chest through the aortic hiatus (T10-T12) - a relatively consistent anatomical landmark.
Thoracic Duct Injury during Neck Dissection
- Usually iatrogenic, left-sided, at level IV lymph node dissection
- Leakage can reach up to 2 L/day with profound nutritional consequences
- Recognized intraoperatively: ligate the proximal duct (safe because lymphovenous anastomoses exist in the lower neck)
- Low-output leak (<500 mL/day): low-fat diet + octreotide (conservative)
- High-output leak: total parenteral nutrition, surgical re-exploration - Bailey & Love's Surgery, p. 829
Thoracic Duct Ligation (Surgical)
For chylothorax management, mass ligation near the aortic hiatus is the standard approach - this is effective due to the consistent single-duct anatomy at that level.
Key memory aid: The thoracic duct crosses from right to left at T5 - below T5 it is right-sided, above T5 it is left-sided. This explains why right-sided chylothorax is more common with injuries below T5, and left-sided chylothorax with injuries above T5.
This is a shared conversation. Sign in to Orris to start your own chat.