Myelopathy hand mechanisms
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"myelopathy hand" cervical mechanisms
Searching PubMed
"myelopathy hand" cervical spondylotic myelopathy
Searching the Web
myelopathy hand mechanisms cervical spondylotic myelopathy finger escape sign pathophysiology
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC10982913/
Searching Images
myelopathy hand finger escape sign cervical myelopathy
Here is a comprehensive breakdown of myelopathy hand — the constellation of hand dysfunction arising from cervical cord compression, originally described by Ono et al. (1987).
Myelopathy Hand: Mechanisms
Definition & Origin
"Myelopathy hand" is a term coined by Ono et al. (1987) to describe the specific pattern of upper-extremity dysfunction caused by cervical cord damage, distinct from radiculopathy. It is a hallmark of cervical spondylotic myelopathy (CSM) and results from injury to multiple cord pathways simultaneously.
Pathophysiological Mechanisms
1. Corticospinal Tract (Lateral) Compression
The lateral corticospinal tract runs in the lateral funiculus and carries voluntary motor commands to the hand. Compression (from disc herniation, osteophytes, ligamentum flavum hypertrophy, or dynamic stenosis) disrupts:
- Fine motor control — difficulty with keyboard typing, writing, buttoning shirts, using keys
- Rapid alternating movements — impaired grip-and-release cycling
- Spastic co-contraction — muscles cannot smoothly transition between flexion and extension
The corticospinal tracts are somatotopically arranged, with cervical fibers in the most central/medial position. Cord compression at C3–C7 selectively injures these fibers early.
2. Anterior Horn Cell Damage (Lower Motor Neuron Component)
Compression also injures the anterior horn cells of the cervical enlargement, which supply the intrinsic hand muscles (interossei, lumbricals, thenar/hypothenar muscles):
- Intrinsic muscle wasting — atrophy of interossei and hypothenar muscles
- The combination of UMN spasticity + LMN wasting gives the myelopathy hand its mixed picture
3. Posterior Column (Dorsal Column) Dysfunction
Compression of the dorsal columns disrupts proprioception and fine-touch discrimination:
- Impaired joint position sense in the fingers
- Contributes to clumsiness even when motor strength is relatively preserved
- Patients struggle with tasks requiring sensory feedback (e.g., doing up buttons without looking)
4. Vascular Ischemia
Dynamic and static compression reduces blood flow in the pial arterial plexus and penetrating arteries supplying the cord gray matter:
- The C5–C7 region is the most vascularly tenuous zone of the cervical cord
- Ischemia of anterior horn cells → selective intrinsic muscle loss
- Venous congestion further exacerbates gray matter injury (the "snake-eyes" or "owl-eyes" MRI appearance reflects bilateral anterior horn ischemia)
Clinical Manifestations of Myelopathy Hand
| Feature | Mechanism | Test |
|---|---|---|
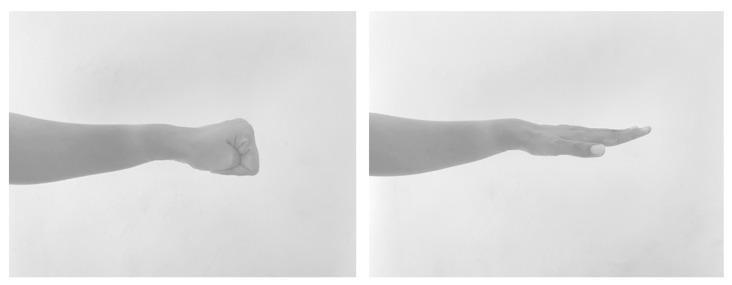
| Finger escape sign | Weakness of intrinsic muscles (interossei) → ulnar 2 digits drift into abduction/flexion when attempting sustained extension/adduction | Hold fingers extended & adducted for 60 s; positive if small/ring finger escapes (sensitivity 55%, specificity 100%) |
| Grip-and-release test | Corticospinal tract dysfunction → inability to rapidly coordinate grip/extension cycling | <20 cycles in 10 s = abnormal (normal ≥20) |
| Intrinsic muscle wasting | Anterior horn cell + ischemic damage at cervical enlargement | Inspection of interossei and thenar/hypothenar |
| Fine motor loss | Combined corticospinal + dorsal column disruption | Writing, typing, buttoning |
| Hoffmann sign | Loss of corticospinal inhibition of C8 flexor reflex arc | Flick middle fingernail → thumb flexion/adduction = positive |
| Inverted radial reflex | Arc at C5-C6 compressed (LMN), with preserved C7/C8 reflexes disinhibited (UMN); brachioradialis tap triggers finger flexion instead of elbow flexion | Eliciting brachioradialis reflex |
Why the Small Finger Escapes First
The finger escape sign is highly specific (100%) because:
- The abductor digiti minimi and palmar interossei to the 5th digit are innervated by the deep ulnar nerve (C8–T1), whose anterior horn cells lie in the most vulnerable medial zone of the cervical enlargement
- Corticospinal control of ulnar intrinsics is the first to fail because these fibers traverse a relatively more compressed region of the cord
- The result: when attempting to extend and adduct the fingers, the small (and sometimes ring) finger "escapes" into flexion and abduction
Grip-and-Release Test: Mechanism
Normal individuals complete ≥20 cycles in 10 seconds. In myelopathy hand:
- The corticospinal tract cannot rapidly alternate between activation of flexors (grip) and extensors (release)
- Spastic co-contraction and delays in reciprocal inhibition slow the cycle
- A 2026 surgical series (PMID 41808140) confirmed level-specific impairment — cord compression at C5–C6 most severely reduces grip-and-release scores
Summary Pathway
Cervical canal stenosis
↓
Cord compression (static + dynamic)
↓
┌─────────────────────────────────────────────────┐
│ Lateral corticospinal tract → spasticity, │
│ impaired rapid grip-release │
│ Anterior horn cells → intrinsic wasting, │
│ finger escape sign │
│ Dorsal columns → proprioceptive loss, │
│ fine motor clumsiness │
│ Vascular ischemia → gray matter necrosis │
│ (snake-eyes sign on MRI) │
└─────────────────────────────────────────────────┘
↓
"Myelopathy Hand"
Sources:
- Miller's Review of Orthopaedics 9th Edition, p. 761
- Ono K et al. J Bone Joint Surg Br 1987 (original description)
- Clinical review of hand manifestations of CSM — PMC10982913
- Kobayashi H et al. BMC Musculoskelet Disord 2026 [PMID 41808140] — level-specific grip-and-release impairment
This is a shared conversation. Sign in to Orris to start your own chat.