Benzodiazepam explain me
Reading File
Finding Sources
Finding Sources
Searching the Web
benzodiazepines pharmacology mechanism of action clinical uses
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from the textbooks to provide a thorough answer. Let me compile it all.
Benzodiazepines - Complete Overview
1. What Are Benzodiazepines?
The term "benzodiazepine" refers to the chemical structure: a benzene ring fused to a seven-membered diazepine ring, with a phenyl group attached at position 5. They are CNS depressants that have largely replaced barbiturates as sedative-hypnotics because they have fewer side effects, cause less liver enzyme induction, and are much safer in overdose.
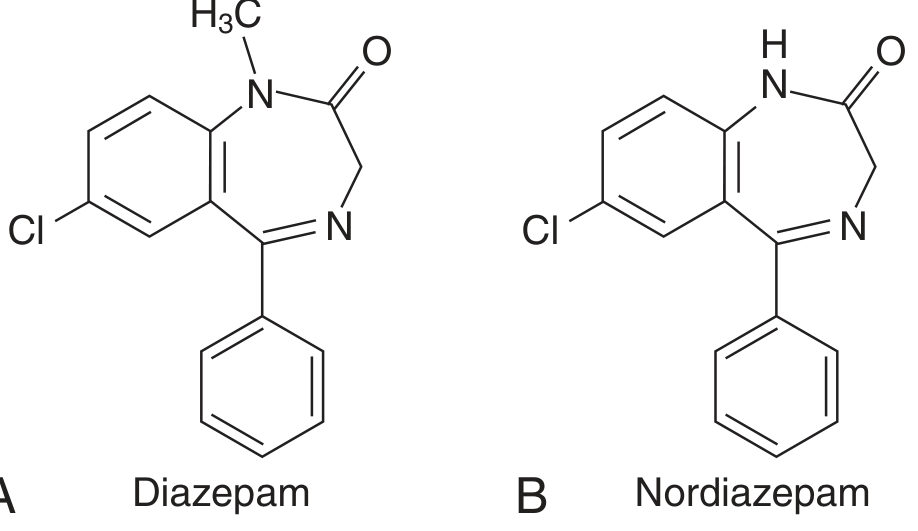
Structures of diazepam and its active metabolite nordiazepam - Tietz Textbook of Laboratory Medicine, 7th Ed.
2. Mechanism of Action
Benzodiazepines act at the GABA-A receptor, which is a ligand-gated chloride (Cl-) ion channel and a heteropentamer (most commonly 2α + 2β + 1γ subunits).
Key points:
- Benzodiazepines bind to a distinct allosteric site at the interface between the α- and γ-subunits (NOT the GABA binding site itself)
- They increase the frequency of Cl- channel opening in response to GABA
- They do NOT directly activate the receptor - they only enhance GABA's effect (positive allosteric modulators)
- The result is an influx of Cl- ions → membrane hyperpolarization → reduced neuronal excitability
Compare to barbiturates:
| Feature | Benzodiazepines | Barbiturates |
|---|---|---|
| Channel effect | Increase frequency of opening | Increase duration of opening |
| Mechanism | Indirect (need GABA) | Direct activation at high doses |
| Overdose safety | Much safer | Can cause fatal respiratory depression |
Subunit-specific effects (from mutational studies):
| Subunit | Effect mediated |
|---|---|
| α1 | Sedation, amnesia |
| α2 | Anxiolysis |
| α3 | Fear reduction |
| α5 | Muscle relaxation |
This explains why drugs like zolpidem (selective for α1) cause sedation with fewer anxiolytic/muscle relaxant side effects.
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry and Goodman & Gilman's Pharmacological Basis of Therapeutics
3. Pharmacokinetics
Absorption: Well absorbed orally; bind strongly to plasma proteins
Metabolism: Hepatic (CYP enzymes) - many have active metabolites
- Diazepam → nordazepam (active, long-acting)
- Flurazepam → long-acting active metabolites (t½ ~74 h)
- Lorazepam, oxazepam, temazepam - metabolized by direct glucuronide conjugation (safe in liver disease, elderly - "LOT" drugs)
Duration of action (half-lives):
| Category | Drug | t½ |
|---|---|---|
| Ultra-short | Midazolam | ~2 h |
| Short | Triazolam, alprazolam | 12 h |
| Intermediate | Lorazepam, oxazepam | 14 h |
| Long | Diazepam | 43 h |
| Very long | Flurazepam, chlordiazepoxide | 74+ h |
4. Clinical Uses
| Drug | Indication |
|---|---|
| Diazepam | Anxiety, alcohol withdrawal, status epilepticus, muscle relaxation, preanesthesia |
| Lorazepam | Anxiety, alcohol withdrawal, seizures, preanesthesia |
| Clonazepam | Seizure disorders, panic disorder, acute mania |
| Alprazolam | Anxiety disorders, panic/agoraphobia |
| Midazolam | Procedural sedation, induction |
| Flurazepam/temazepam | Insomnia |
| Chlordiazepoxide | Anxiety, alcohol withdrawal |
| Clobazam | Lennox-Gastaut syndrome |
A newer agent, remimazolam, was FDA-approved in 2020 for short procedural sedation. It has faster onset/offset than midazolam and is reversible with flumazenil.
- Goodman & Gilman's, Table 22-2
5. Adverse Effects
- CNS effects: Light-headedness, lassitude, slowed reaction time, motor incoordination, confusion, anterograde amnesia
- Impaired driving: 60-80% increased risk of traffic accidents; alcohol + benzodiazepine gives a 7.7-fold increase
- Disinhibition: Can trigger impulsive, aggressive, or suicidal behavior in vulnerable patients
- Paradoxical reactions: Hyperactivity, agitation (especially in children/elderly)
- Respiratory depression: Less than barbiturates, but serious when combined with opioids or alcohol
- Overdose fatality: Low when taken alone; dramatically increases with co-ingestion of opioids or alcohol
6. Tolerance, Dependence, and Withdrawal
Tolerance develops most easily to:
- Sedation (most common)
- Psychomotor impairment
- Less commonly to anxiolytic effects
Mechanism of tolerance: Prolonged receptor occupation triggers intracellular Ca2+ signaling → receptor downregulation/uncoupling.
Three discontinuation syndromes:
| Syndrome | Onset | Features |
|---|---|---|
| Relapse | Weeks-months | Return of original illness |
| Rebound | Days-weeks | Worse-than-original anxiety/insomnia |
| Withdrawal | Hours-days (short-acting) / 1-2 weeks (long-acting) | Sweating, tachycardia, tremor, nausea, myoclonus, seizures, delirium |
Risk of severe withdrawal is highest with high-potency, short-acting drugs (alprazolam, triazolam) and in long-term users.
7. The Antagonist: Flumazenil
- Competitive antagonist at the benzodiazepine binding site
- Used to reverse benzodiazepine overdose and post-procedural sedation
- Can precipitate acute withdrawal seizures in physically dependent patients
- Short t½ (~1 h) - re-sedation can occur; multiple doses often needed
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
8. Special Concerns
- Elderly: Avoid or use the lowest possible dose. Risk of falls, hip fractures, cognitive impairment, and overuse-related problems are highest in this population.
- Pregnancy: Associated with neonatal withdrawal; use only if clearly necessary.
- Dementia risk: Recent studies suggest an association between chronic benzodiazepine use and dementia.
- Opioid co-prescription: The U.S. rate of combined BZD + opioid use rose from 9.8 to 62.5/100,000 between 1993-2014, correlating with increased overdose deaths.
Quick video overview:
This is a shared conversation. Sign in to Orris to start your own chat.