Explain me 10 common heart diseases with ech changes and ecg images of these diseases
Reading File
Finding Sources
Finding Sources
Searching the Web
common heart diseases ECG changes electrocardiogram findings images
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
Searching the Web
heart block Wolff Parkinson White LVH pulmonary embolism ECG changes findings site:litfl.com OR site:ecgwaves.com
Reading Web Page
https://litfl.com/ecg-differential-diagnosis-ecg-library
Loading Image
I have enough information from the textbooks and my medical knowledge to write a comprehensive, well-illustrated answer. Let me now compose the full response.
10 Common Heart Diseases: ECG Changes and Images
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causes transmural ischemia. Three electrical events occur: rapid repolarization, decreased resting membrane potential, and delayed depolarization - all producing current flow that elevates the ST segment in overlying leads.
ECG Changes:
- Hyperacute T waves (earliest sign, within minutes)
- ST segment elevation (convex "tombstone" shape) in leads overlying the infarct
- Reciprocal ST depression in opposite leads
- Q waves develop over hours-days (necrosis marker)
- T-wave inversion follows as infarct evolves
- Location by lead:
- Anterior (LAD): V1-V4
- Inferior (RCA): II, III, aVF
- Lateral (LCx): I, aVL, V5-V6
- Posterior: tall R in V1-V2 + ST depression V1-V3
Serial ECG changes in anterior infarction (Ganong's Review of Medical Physiology, p. 534):
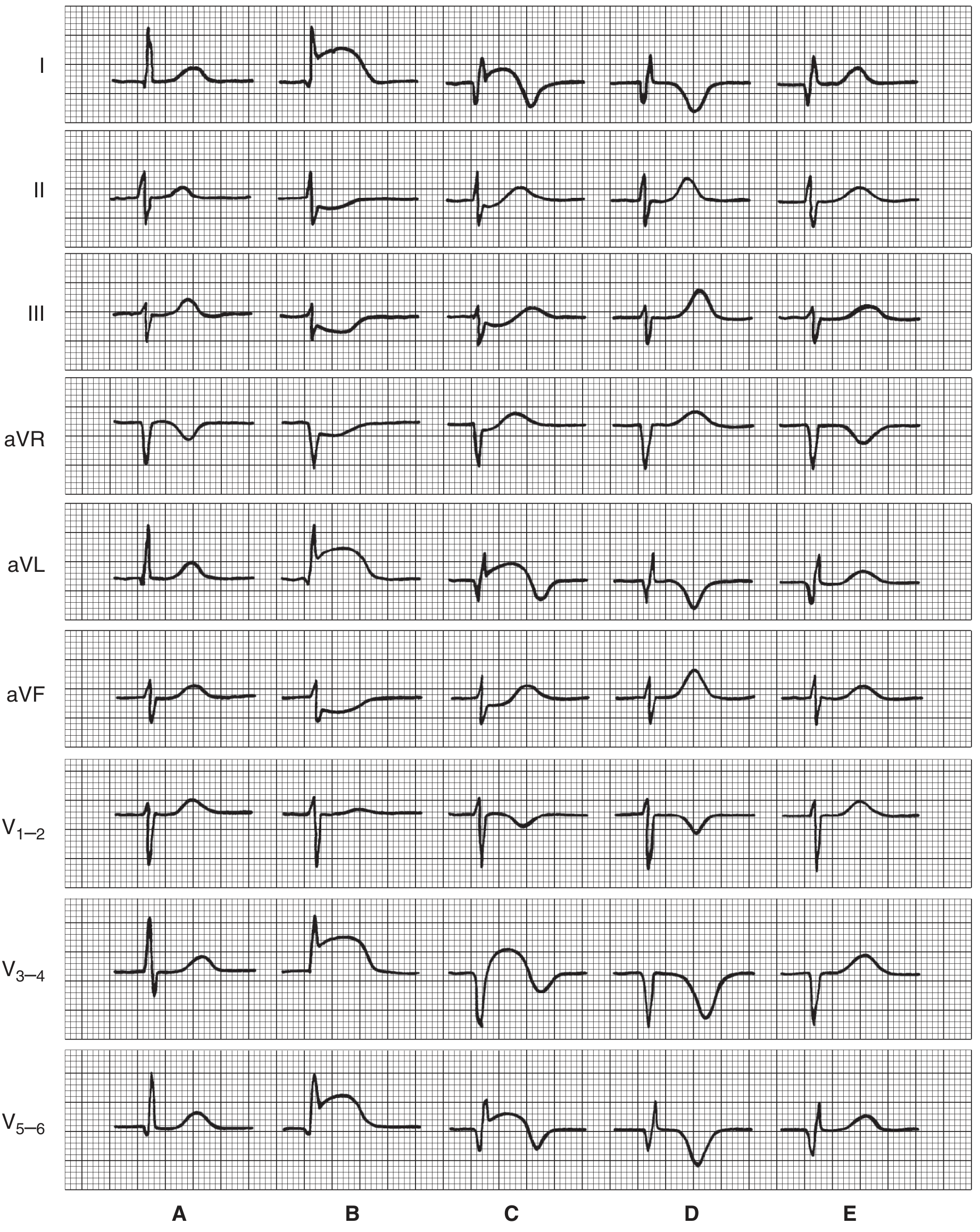
Figure: Serial ECG patterns in anterior infarction. A = normal; B = early ST elevation in I, aVL, V3-5 with reciprocal depression in III/aVF; C = Q waves and QS complexes in V3-4; D = deepening T-wave inversions; E = late recovery pattern.
2. Non-ST Elevation Myocardial Infarction (NSTEMI) / Unstable Angina
Pathophysiology: Subtotal or transient coronary occlusion causing subendocardial ischemia. The ST vector shifts toward the subendocardium, producing ST depression rather than elevation in overlying leads.
ECG Changes:
- ST segment depression (horizontal or downsloping, ≥0.5 mm)
- T-wave inversion (may be deep and symmetrical)
- Wellens' T-wave sign: deep symmetric T-wave inversions in V1-V4 indicate critical proximal LAD stenosis - a high-risk pattern
- Transient ST elevation possible with vasospasm (Prinzmetal's angina)
- ECG may be normal in up to 6% of confirmed NSTEMIs (Harrison's, p. 1916)
Wellens' T-wave pattern - deep symmetric precordial T-wave inversions from severe LAD stenosis (Harrison's 22E):

Figure: Severe anterior wall ischemia - deep T-wave inversions in precordial leads V1-V6. This Wellens' pattern strongly predicts high-grade LAD stenosis.
3. Atrial Fibrillation (AF)
Pathophysiology: Chaotic, disorganized atrial electrical activity with multiple re-entrant circuits. Associated with ischemic heart disease, valvular disease, cardiomyopathy, thyrotoxicosis, and alcohol ("holiday heart"). Left atrial enlargement is a common predisposing feature.
ECG Changes (from Tintinalli's, p. 149):
- Absent P waves - flat or chaotic/fibrillatory baseline (most important feature)
- Irregularly irregular ventricular rhythm (hallmark)
- Narrow QRS complexes (unless pre-existing BBB or WPW pre-excitation)
- Ventricular rate typically 100-180 bpm if uncontrolled
- No two R-R intervals are equal
| ECG Feature | Detail |
|---|---|
| P waves | Absent; baseline replaced by fine fibrillatory waves |
| Rhythm | Irregularly irregular |
| QRS | Narrow (unless aberrant conduction) |
| Rate | Variable (60-180+ bpm) |
4. Atrial Flutter
Pathophysiology: A macro-re-entrant circuit in the right atrium (typically around the tricuspid annulus), producing regular rapid atrial activity at ~300 bpm.
ECG Changes (Tintinalli's, p. 150):
- "Sawtooth" flutter waves at ~300 bpm, best seen in inferior leads (II, III, aVF) and V1
- Flutter waves are negative (downward) in inferior leads
- Regular atrial rate ~250-350 bpm
- Ventricular rate usually 150 bpm (2:1 AV block) - a regular narrow-complex tachycardia at exactly 150 bpm should always prompt suspicion for flutter
- QRS narrow unless pre-existing BBB
- Carotid sinus massage reveals hidden flutter waves by slowing AV conduction
Atrial flutter - sawtooth waves in leads II, III, aVF (Tintinalli's Emergency Medicine):
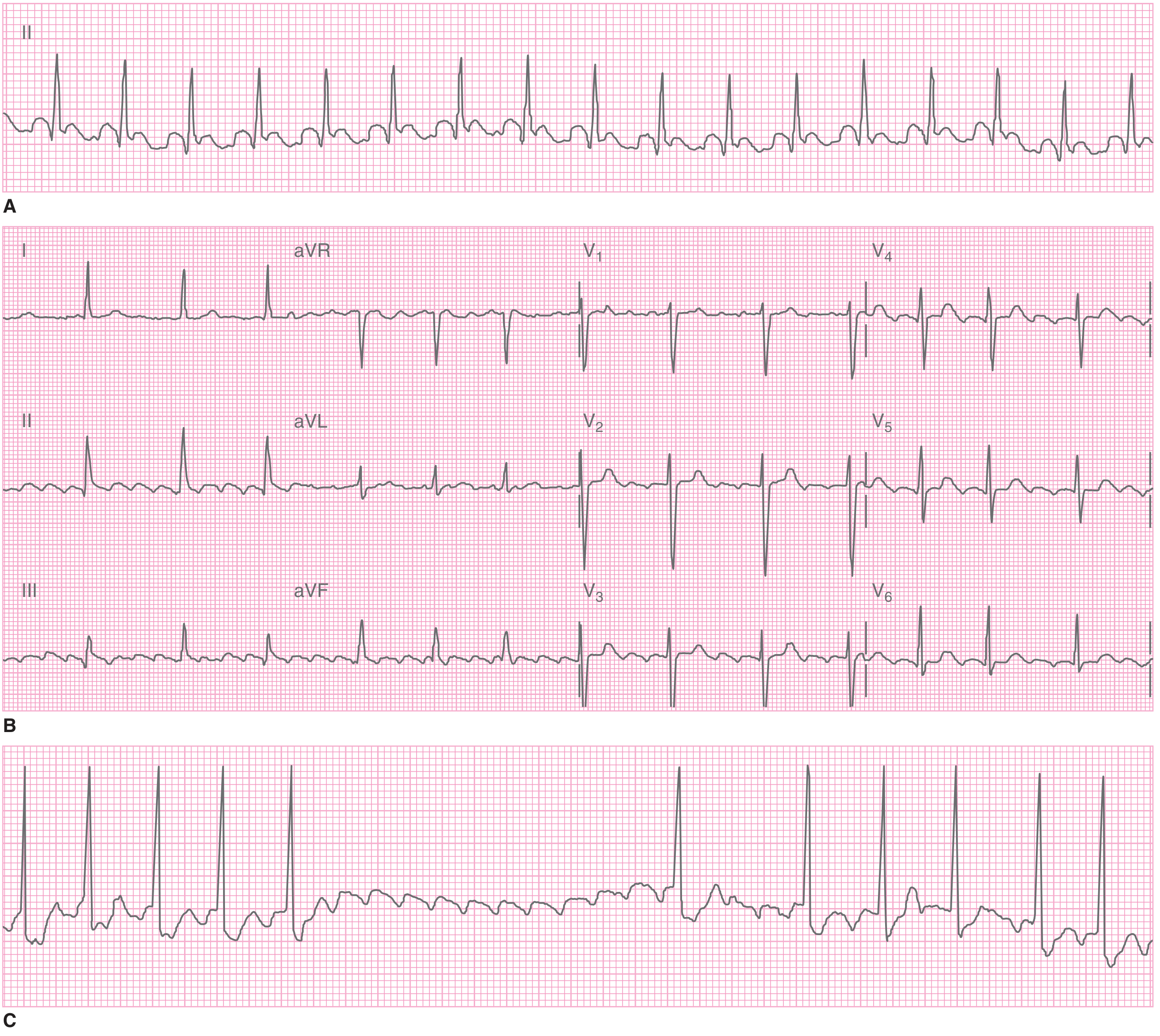
Figure: Atrial flutter. A = Regular narrow-complex tachycardia at 155 bpm. B = Sawtooth flutter waves in leads II, III, aVF. C = Carotid sinus massage induces transient AV block, unmasking flutter waves.
5. Acute Pericarditis
Pathophysiology: Inflammation of the pericardium (most commonly viral) irritates the epicardial surface of the myocardium, producing a diffuse, non-territory-specific electrical injury pattern across multiple leads.
ECG Changes - 4 Stages (Fuster & Hurst's Heart, p. 1667; Goldman-Cecil, p. 2218):
| Stage | Timing | ECG Finding |
|---|---|---|
| Stage 1 | Hours to days | Diffuse ST elevation (concave up/saddle-shaped) + PR depression in nearly all leads; aVR shows ST depression + PR elevation |
| Stage 2 | Days | ST and PR return to baseline |
| Stage 3 | Weeks | Diffuse T-wave inversions |
| Stage 4 | Weeks-months | ECG normalizes |
Key distinguishing features from STEMI:
- ST elevation is diffuse (not territory-specific)
- ST shape is concave upward (vs. convex in STEMI)
- PR depression is strongly characteristic of pericarditis
- No reciprocal ST changes (except aVR/V1)
- No Q waves
Stage 1 acute pericarditis ECG (Fuster & Hurst's Heart, 15th Ed):
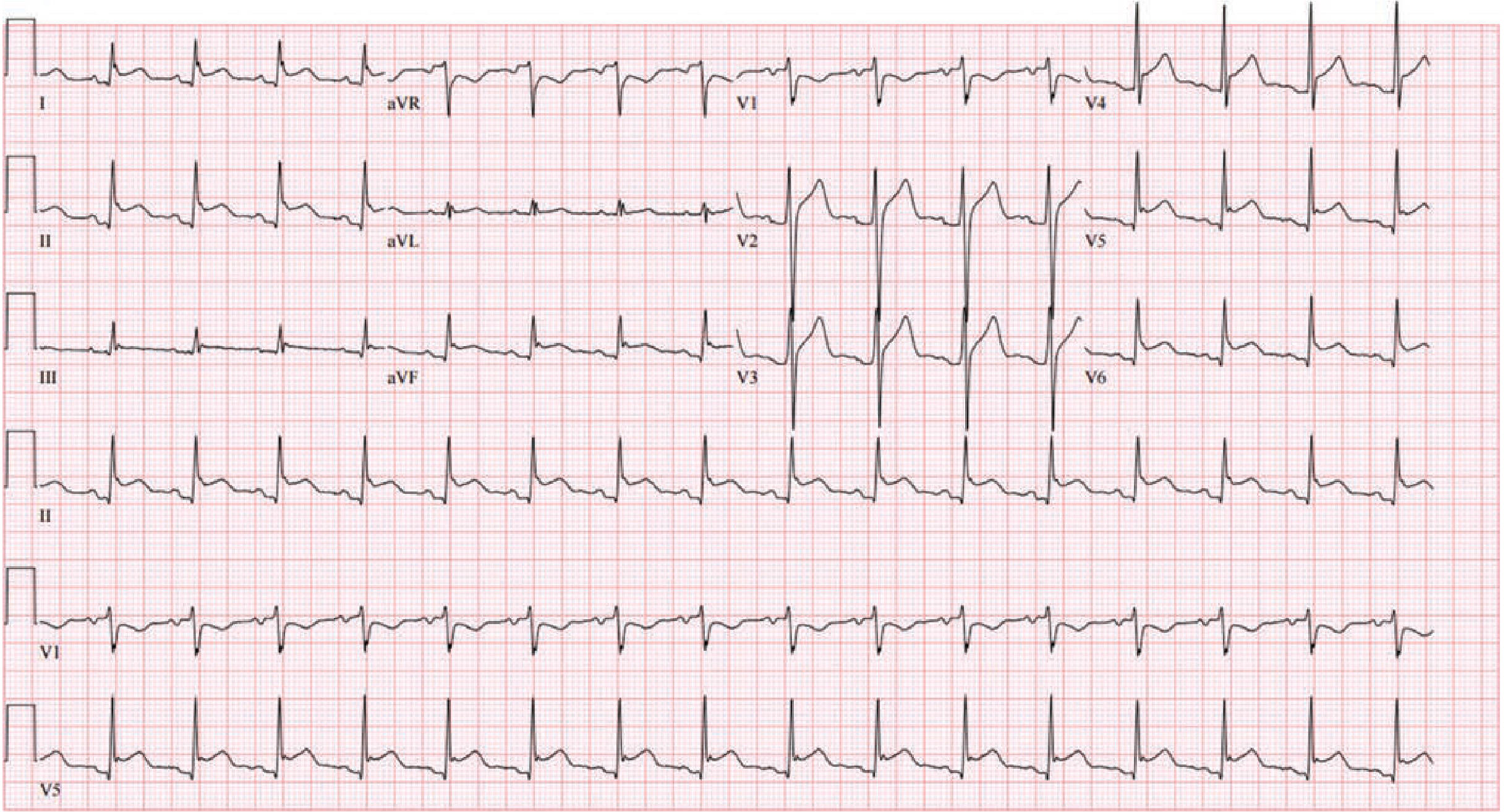
Figure: Stage I acute pericarditis. Diffuse ST elevation with concordant PR depression in a non-territory-specific distribution. aVR shows classic ST depression with PR elevation.
6. Left Ventricular Hypertrophy (LVH)
Pathophysiology: Increased left ventricular muscle mass (from hypertension, aortic stenosis, HCM) increases the electrical voltage generated during depolarization and alters repolarization.
ECG Changes:
- High voltage QRS - classic criteria:
- Sokolow-Lyon: S in V1 + R in V5 or V6 ≥35 mm
- Cornell: R in aVL + S in V3 >20 mm (women) or >28 mm (men)
- Left axis deviation
- "LV strain" pattern: ST depression and asymmetric T-wave inversion in lateral leads (I, aVL, V5-V6) - the repolarization abnormality of LVH
- Left atrial enlargement: Broad bifid P waves in lead II ("P mitrale"); negative terminal deflection of P in V1
- Poor R-wave progression may be present
- Increased QRS duration may approach 0.10-0.11 s
7. Complete (Third-Degree) AV Heart Block
Pathophysiology: Complete dissociation between atrial and ventricular conduction. The atria beat independently (sinus P waves at normal rate) and the ventricles beat independently driven by a subsidiary escape pacemaker (junctional or ventricular).
ECG Changes:
- P waves present at normal rate (60-100 bpm), regular
- QRS complexes present at slow escape rate (20-45 bpm), regular
- P waves and QRS are completely dissociated - no fixed PR relationship
- QRS morphology depends on escape pacemaker location:
- Junctional escape (His bundle): narrow QRS, rate 40-60 bpm
- Ventricular escape: wide bizarre QRS (>120 ms), rate 20-40 bpm
- More P waves than QRS complexes
- The PR interval varies continuously - no P always precedes each QRS
Compare with other blocks:
- 1st degree: prolonged PR >200 ms, every P followed by QRS
- 2nd degree Mobitz I (Wenckebach): progressively lengthening PR until a QRS is dropped
- 2nd degree Mobitz II: fixed PR with sudden dropped QRS (more dangerous)
- 3rd degree: complete dissociation as above
8. Ventricular Tachycardia (VT)
Pathophysiology: Rapid firing of a ventricular focus (re-entry, triggered activity, or enhanced automaticity), often on a substrate of prior MI, cardiomyopathy, or channelopathy. A life-threatening arrhythmia.
ECG Changes:
- Wide QRS tachycardia (>120 ms), typically bizarre morphology
- Rate 100-250 bpm, usually regular
- AV dissociation: P waves march through at independent sinus rate, unrelated to QRS (diagnostic when present)
- Fusion beats: sinus impulse partially activates ventricles, creating a hybrid QRS (diagnostic)
- Capture beats: a sinus impulse fully captures the ventricle, producing a narrow QRS amid wide complexes (diagnostic)
- Concordance in precordial leads (all QRS positive or all negative) favors VT
- Northwest axis (QRS negative in both I and aVF) favors VT
- Brugada criteria used to differentiate from SVT with aberrancy
Ventricular Fibrillation (VF):
- Chaotic, irregular, no identifiable QRS complexes
- Baseline appears as sinusoidal undulations of varying amplitude
- No cardiac output - immediately fatal without defibrillation
9. Wolff-Parkinson-White Syndrome (WPW)
Pathophysiology: An accessory pathway (Bundle of Kent) bypasses the AV node, allowing premature ventricular pre-excitation. This creates a short PR interval and a delta wave. The critical danger is that if AF develops, the accessory pathway can conduct at very rapid rates (200-300 bpm) directly to the ventricles, potentially causing VF.
ECG Changes (classic WPW triad):
- Short PR interval (<120 ms) - bypass of AV nodal delay
- Delta wave - slurred initial upstroke of QRS from pre-excitation of ventricular myocardium
- Wide QRS (>120 ms) - total duration of delta + normal QRS
- Secondary ST-T changes - discordant repolarization opposite to delta/QRS
- Pseudo-infarct patterns: delta waves can mimic Q waves in inferior leads
- Pathway location determines delta wave polarity:
- Left lateral pathway: negative delta in I/aVL, positive in V1
- Right-sided pathway: positive delta in I, negative in V1/V2
10. Pulmonary Embolism (PE)
Pathophysiology: Acute obstruction of pulmonary vasculature causes right heart pressure overload, right ventricular dilation and strain. The stretched RV rotates the heart clockwise, shifts the QRS axis rightward, and causes RV conduction delay.
ECG Changes:
- Sinus tachycardia - most common and most sensitive finding (present in ~44% of PE)
- S1Q3T3 pattern (classic but present in only ~20%):
- S wave in lead I
- Q wave in lead III
- T-wave inversion in lead III
- Right heart strain pattern: T-wave inversions in V1-V4 (right precordial leads)
- Incomplete or complete RBBB - from RV dilation and conduction delay
- P pulmonale: tall peaked P waves in II from right atrial pressure overload
- Right axis deviation
- Atrial arrhythmias (AF, flutter) from atrial stretch
- Normal ECG does NOT exclude PE
Key points:
- S1Q3T3 is specific but not sensitive - its absence does NOT rule out PE
- The combination of sinus tachycardia + T-wave inversions V1-V4 + new RBBB is highly suggestive of massive PE
Quick Reference Summary Table
| Disease | Key ECG Change | Hallmark Pattern |
|---|---|---|
| STEMI | ST elevation, Q waves, T inversion | Convex ST elevation in territory |
| NSTEMI/UA | ST depression, T inversion | Horizontal/downsloping ST depression |
| Atrial Fibrillation | No P waves, irregular RR | Irregularly irregular |
| Atrial Flutter | Sawtooth flutter waves | 300 bpm flutter, 150 ventricular |
| Pericarditis | Diffuse concave ST elevation, PR depression | Saddle-shaped diffuse ST, PR depression |
| LVH | High voltage, strain pattern | Sokolow-Lyon ≥35 mm, lateral ST depression |
| Complete Heart Block | AV dissociation, slow escape | No P-QRS relationship |
| Ventricular Tachycardia | Wide QRS tachycardia | AV dissociation, fusion/capture beats |
| WPW | Short PR, delta wave, wide QRS | Pre-excitation triad |
| Pulmonary Embolism | Sinus tach, S1Q3T3, RV strain | T inversions V1-V4, new RBBB |
Sources: Ganong's Review of Medical Physiology 26E; Harrison's Principles of Internal Medicine 22E; Tintinalli's Emergency Medicine; Fuster and Hurst's The Heart 15E; Goldman-Cecil Medicine; LITFL ECG Library.
This is a shared conversation. Sign in to Orris to start your own chat.